
Abstract
Congenital anomalies of the superior and inferior vena cava result from abnormal embryogenesis of cardinal veins. Duplication of superior vena cava (SVC) occurs in 0.3% of the general population of which only 8% drain into the left atrium. The prevalence of double inferior vena cava (IVC) is around 0.2–3%. The reported incidence of unilateral renal agenesis ranges from 1:1100 to 1:5000, and the association of double IVC with renal agenesis has been reported in only 11 cases in the literature. The conglomeration of such rare anomalies incidentally noted in a single patient is reported in this study. A 32-year-old man was referred to our department for Computed Tomography (CT) scan of the thorax. The patient was found to have dorsal kyphoscoliosis with hemivertebrae. The SVC was duplicated with the right SVC draining into the right atrium and the left SVC draining into the left atrium. The left kidney was not visualized in the abdomen. There was dual IVC with no intercommunicating interiliac vein. The right IVC maintained its normal course, while the left IVC continued as hemiazygos vein and joined left SVC in the thorax. Also noted was the aberrant origin of the right subclavian artery. This is the first reported case of combined superior and inferior vena caval anomalies along with left renal agenesis in a single patient in the literature. A review on the embryological basis is also described in this article.
Keywords
Case Report
A 32-year-old man with congenital scoliosis was referred to our radiology department for Computed Tomography (CT) scan of the thorax. The patient had history of bilateral pedal edema about 4–5 months back, for which he had undergone ultrasound of the abdomen. The ultrasound showed absence of left kidney with small right kidney. The blood investigations revealed raised creatinine levels. The patient was then referred to nephrology for dialysis and is currently on maintenance hemodialysis. The patient now has complaints of breathlessness and productive cough.
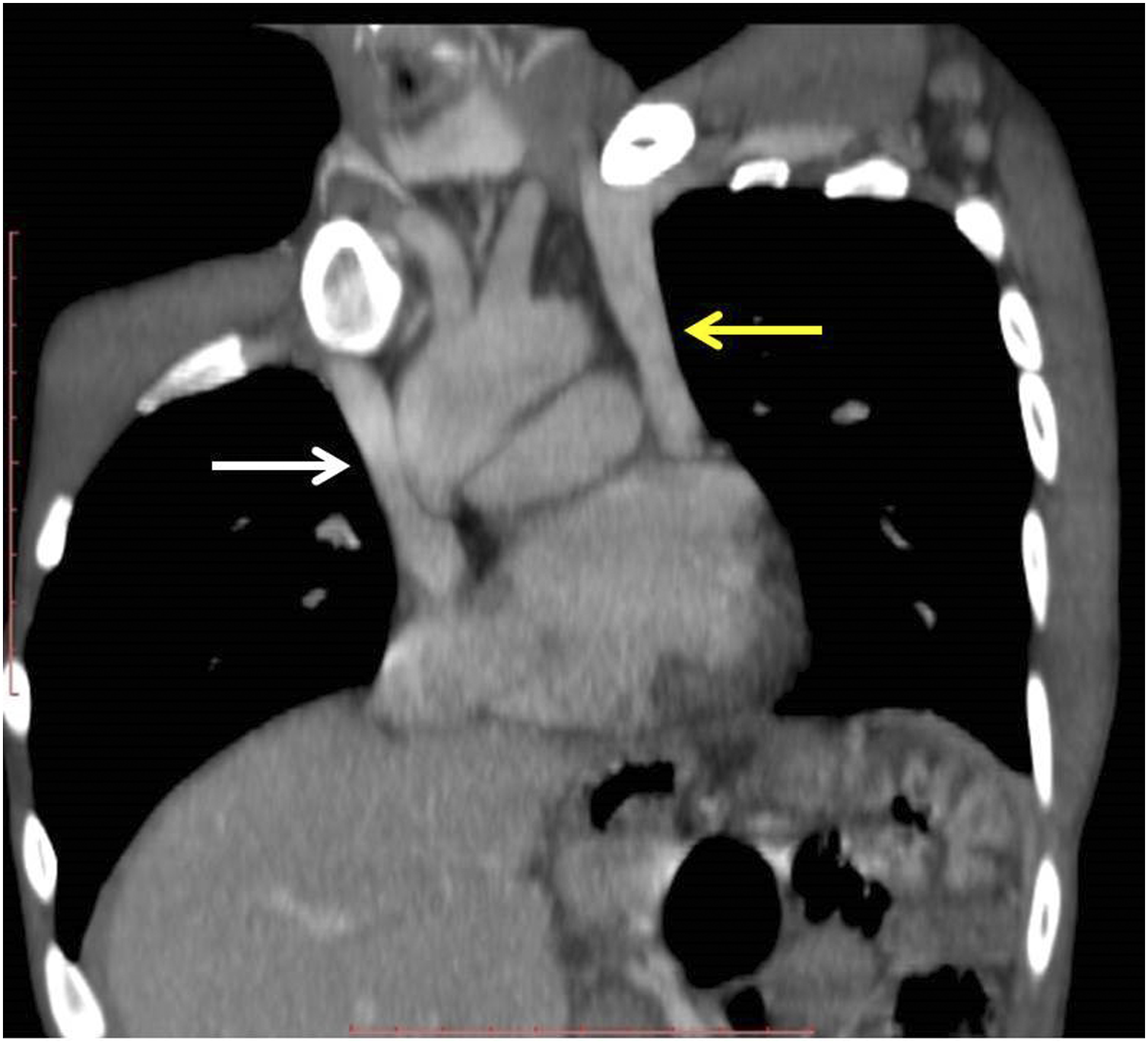
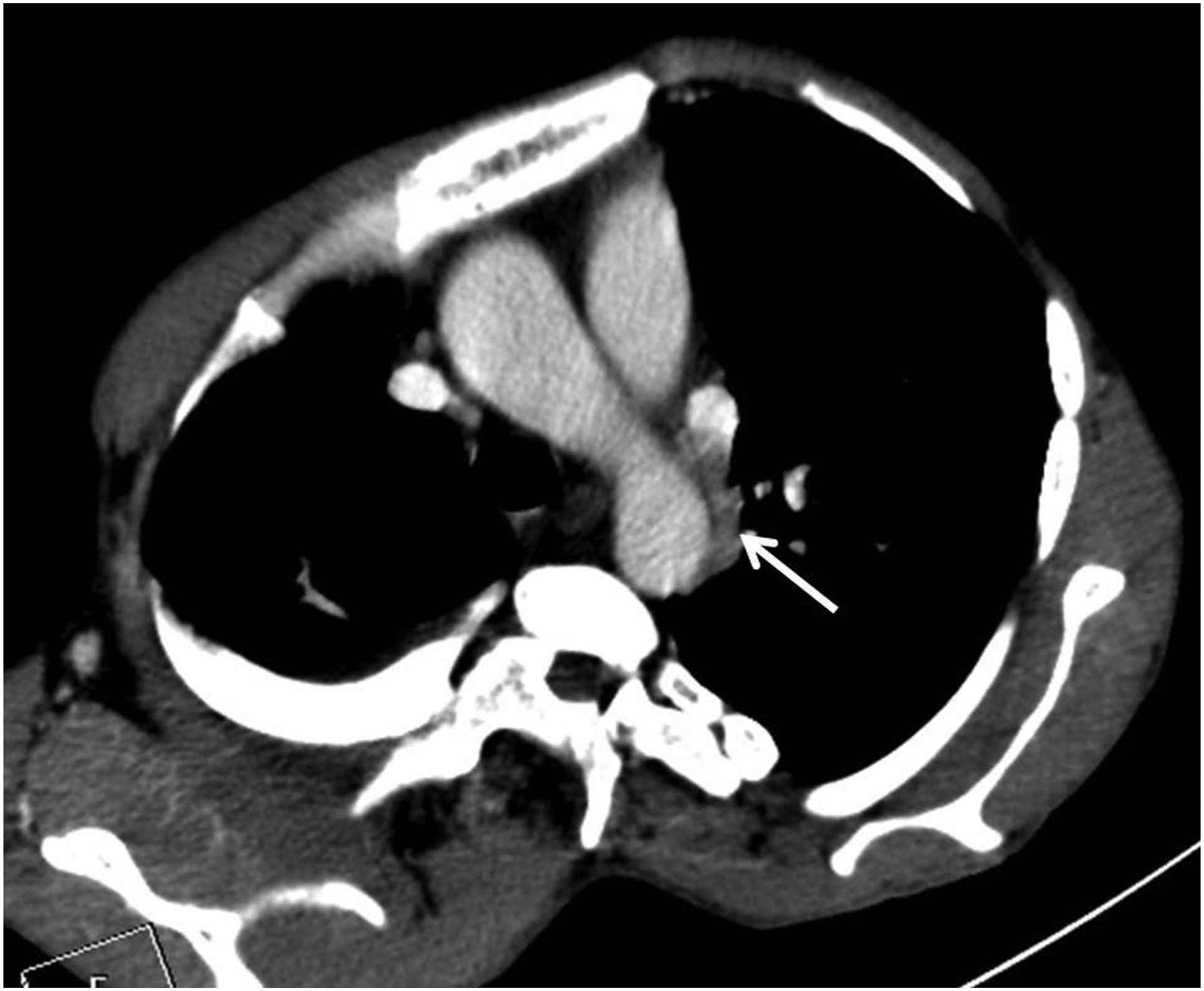
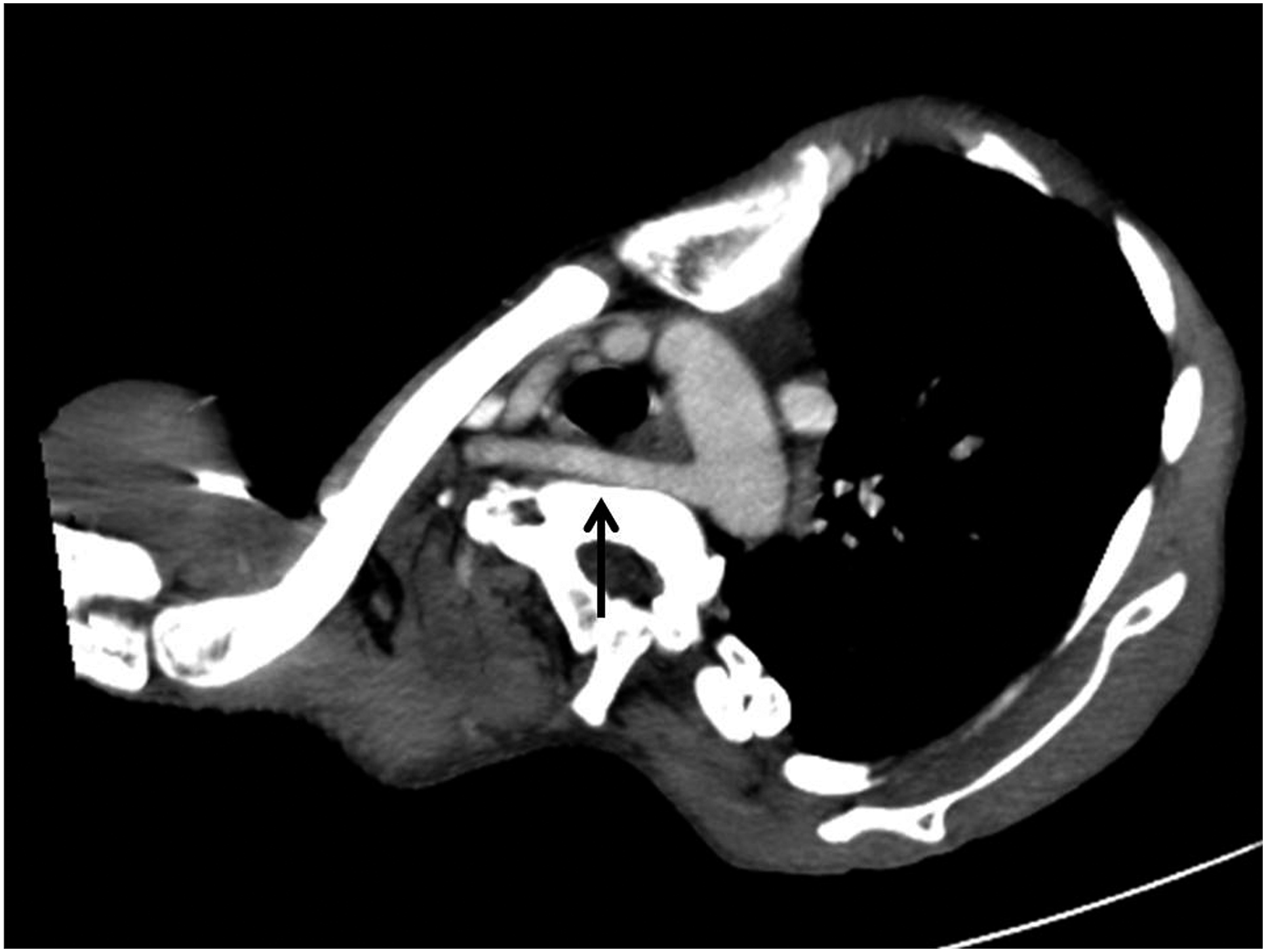
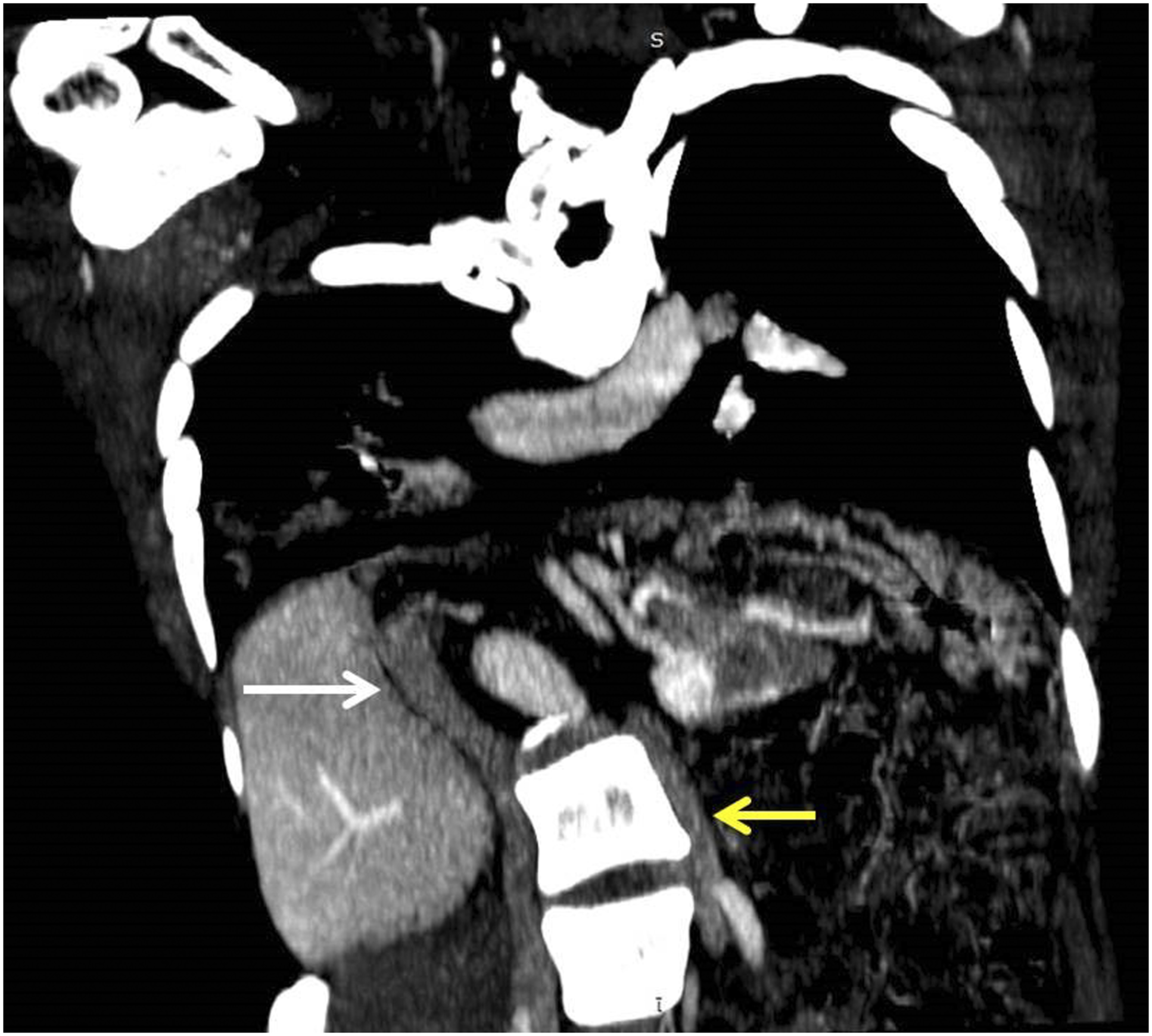
Contrast enhanced CT scan of the chest was performed, after consulting with nephrology department regarding contrast injection. The study showed marked kyphoscoliosis of the dorsal spine with lateral hemivertebrae and multiple fusion of the body and posterior elements of upper dorsal vertebra (Figure 1). Patchy areas of consolidation with few centrilobular nodules were noted in the bilateral lower lobes. It was incidentally noted that the left brachiocephalic vein formed from left internal jugular vein, and left subclavian vein did not cross to right side to join with right brachiocephalic vein. It continued as persistent left superior vena cava (SVC) anterior and lateral to the arch of aorta, which drained into the left atrium (Figure 2). The right SVC drained normally into the right atrium (Figure 2). The left SVC before its drainage into the left atrium received another vessel which was found to be hemiazygos vein (Figure 3). Also noted was the anomalous origin of the right subclavian artery (SCA) from the arch of aorta distal to the origin of left subclavian artery. The right SCA then traversed posterior to the esophagus to reach the right side (Figure 4) and continued into the axilla. Volume-rendered image showing kyphoscoliosis with lateral hemivertebrae (arrow). Oblique coronal reformatted image showing duplicated SVC—right SVC (white arrow) draining into the right atrium, persistent left SVC (yellow arrow) draining into the left atrium. Oblique axial reformatted image showing hemiazygos vein draining into persistent left SVC (arrow). Oblique axial reformatted image showing aberrant right subclavian artery (arrow) passing behind the trachea and esophagus.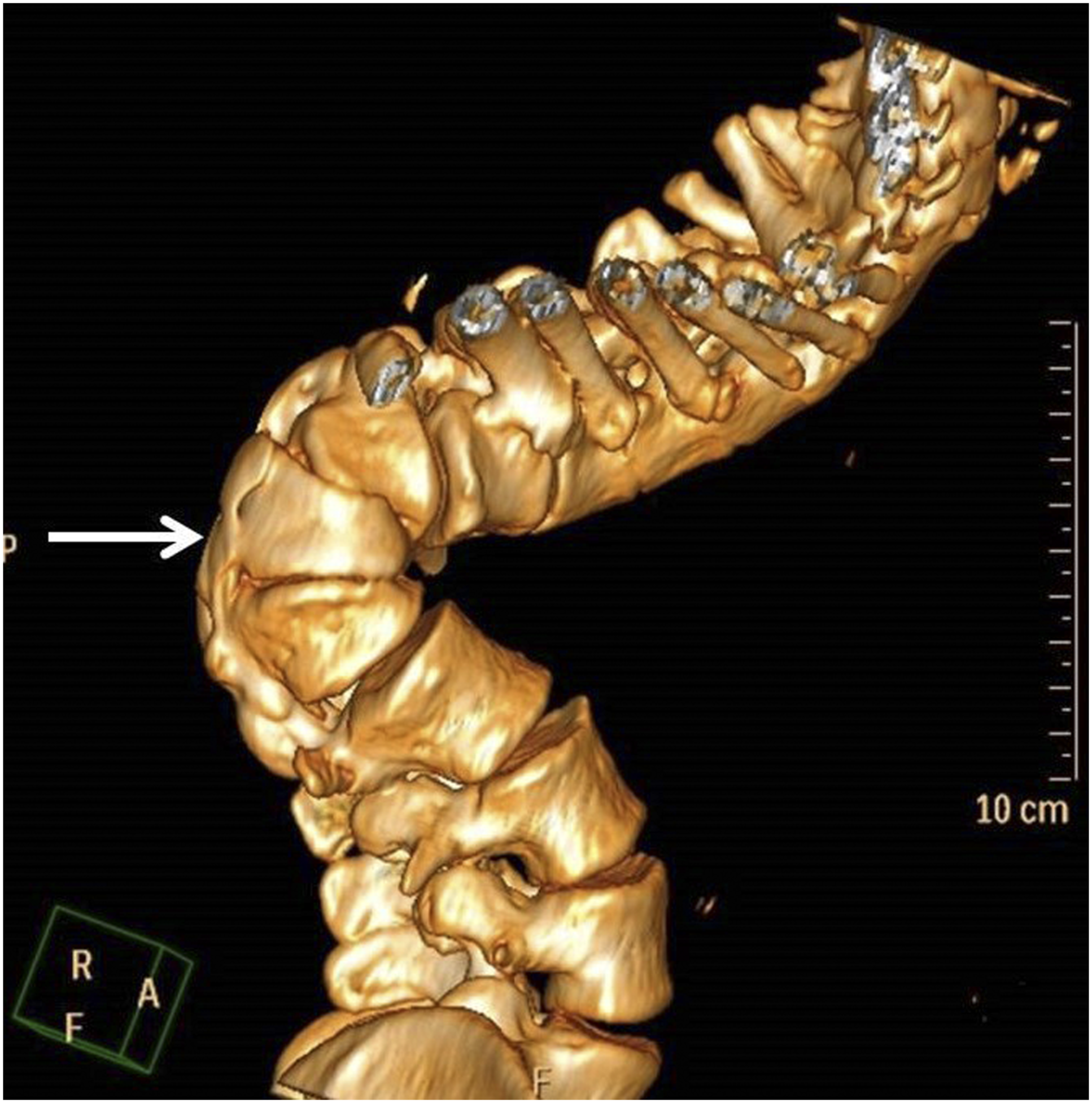
Due to severe scoliosis, the scan included part of the abdomen upto the iliac blades. The left kidney was not visualized in its orthotopic location or along the site of its embryological ascent. The right kidney was smaller in size and measured 6.7 cm along its long axis and showed decreased contrast enhancement (Figure 5). The right and the left iliac veins did not unite to form a single inferior vena cava (IVC) but continued cephalad as two inferior venae cavae on both sides of the abdominal aorta (Figure 6). The right IVC received the right renal vein and continued as intrahepatic portion draining into the right atrium. The hepatic veins were found to drain separately into the right atrium. The left IVC continued cephalad as hemiazygos vein alongside the aorta which joined the left SVC at vertebral level (Figure 6). Oblique axial reformatted image showing small contracted right kidney with absent left kidney. Oblique coronal reformatted image showing bilateral IVC; right IVC—intrahepatic portion (white arrow), and left IVC—hemiazygos continuation (yellow arrow).
Based on these findings, a diagnosis of complex congenital anomalies was made—duplicated superior and inferior vena cava, hemiazygos continuation of left inferior vena cava joining the persistent left superior vena cava, persistent left superior vena cava draining into the left atrium, aberrant right subclavian artery, left renal agenesis, and dorsal kyphoscoliosis.
Discussion
The knowledge of the variations in the venous system is necessary to avoid erroneous diagnosis and also in therapeutic management. A brief review of the embryogenesis of the thoracic and abdominal venous system is essential to understand the developmental anomalies presented in our patient. The embryogenesis of SVC and IVC is a complex process involving the three main systems of paired cardinal veins or somatic veins—anterior and posterior cardinal, supracardinal, and subcardinal veins. These veins arise in chronological order during fourth to eighth week of embryogenesis.1-4 The anterior cardinal veins drain the cranial part of the embryo including the brain; and the posterior cardinal veins drain the caudal part. The posterior cardinal veins are the dominant veins of the abdomen till sixth week. By seventh week, the subcardinal veins become dominant, arising ventromedial to the posterior cardinal veins. During eighth week, the supracardinal veins predominate which are located lateral to the subcardinal veins. Cranially, the supracardinal veins extend above the diaphragm forming the azygos and hemiazygos system of veins.
The superior vena cava is formed from the right anterior cardinal vein and the right common cardinal vein. The left anterior cardinal vein normally regresses.1,4 The incidence of duplicated SVC in general population is 0.3% and 10% in patients with congenital heart disease.4,5 Double SVC is the most common form of anomalous systemic venous return. Duplicated SVC occurs when the left anterior cardinal vein fails to regress, giving rise to left-sided SVC. The left SVC passes anterior and lateral to the aortic arch before joining the circulatory system. The persistent left SVC drains into the right atrium via the coronary sinus in 92% of the cases. In the remaining 8%, the left SVC drains into the left atrium, as the case in our patient.4,6,7
The inferior vena cava is derived in caudo-cranial direction from the caudal portion of the right posterior cardinal vein, the lowest portion of right supracardinal vein (infrarenal segment), the right supracardinal–subcardinal anastomosis, the right subcardinal vein receiving both renal veins (renal segment), the subcardinal–hepatocardiac anastomosis (suprarenal segment), and the right hepatocardiac channel (hepatic segment), draining into the right atrium.2,3,8 Caudal to this IVC development, an oblique transverse anastomosis between the right and left posterior cardinal veins results in the formation of common iliac veins.
A classification system for IVC anomalies was proposed by Huntington and McLure based on abnormal regression or persistence of various embryonic veins.3 Double IVC is the most common variant of IVC anomaly. Duplication of IVC results from persistence of both the supracardinal veins below the level of renal veins with a prevalence of 0.2–3%.3,8 In a recent study, Morita et al 9 reviewed the pelvic venous variations in patients with congenital IVC anomalies and proposed a classification system for double IVC anomalies based on the interiliac communicating vein. In that study, double IVC with no communicating interiliac vein was classified as type 2a, which was also the most common type of double IVC anomaly in that study (39.3%). Our case was also partly similar to the type 2a; however, there was a major difference in our case. All the variations defined by Morita et al involved left IVC joining the left renal vein and crossing to other side and continuing as intrahepatic IVC, which was not the case in our patient. The left renal agenesis in our patient added further to the complexity.
The association of IVC anomalies with renal agenesis is very rare and has been mentioned in only 11 patients in the literature; and only one case has been reported in the literature so far about IVC duplication with left renal aplasia.10,11 It has been postulated that developing kidneys profoundly affect the development of IVC. Lack of space for expanding metanephric tissues causes regression of some of the venous structure in the caudal end of the embryo. The agenesis of the left kidney might cause the left supracardinal vein to persist resulting in anomalous development of the left IVC.
In most of the cases of double IVC seen in the literature, the left IVC joins the left renal vein and crosses the midline to join with right IVC. The prevalence of interruption of IVC with azygos or hemiazygos continuation is around 0.6%.3,12 A rare case of double IVC with hemiazygos continuation of the left-sided IVC and normal course of right-sided IVC has also been described. However in that case, the left IVC joined the left renal vein, which is not present in our patient. 13 The hemiazygos continuation might be due to the persistence of the left suprasubcardinal anastomosis. The hemiazygos vein normally ascends upto D8/D9 vertebra and crosses the midline anterior to vertebra to drain into azygos vein. The hemiazygos vein, in our patient, continued cephalad without crossing over and drained into the left SVC. Only one case has been reported so far regarding the hemiazygos continuation of the left IVC joining the persistent left SVC and draining into the right atrium. 8 Our case is different in the main finding that the left SVC in our patient drains into the left atrium.
The arteries of the embryo arise from the aortic arches which begin to form from fourth week of gestation.1,14 Initially, double aortic arch is present which gives rise to right and left subclavian and common carotid arteries. Under normal circumstances, the right aortic arch distal to right subclavian artery regresses and right subclavian and common carotid form the brachiocephalic trunk. If the right aortic arch between the right subclavian and common carotid artery regresses, the brachiocephalic trunk does not form, with right subclavian arising distal to the origin of the left subclavian artery. The incidence of aberrant right subclavian artery (ARSA) is approximately 0.5–1.5%.14,15 Only one case has been reported in the literature regarding the aberrant right subclavian artery with persistent left superior vena cava. 16
The major clinical significance of these anomalies is the potential for misdiagnosis of the venous structures. Cases are reported where radiographic duplication of the IVC has been confused with saccular aortic aneurysms, para aortic lymphadenopathy, left ureteric dilatation, and retroperitoneal cysts. 3 However with development of multidetector computed tomography and magnetic resonance imaging, the identification of such anomalies has become easier.
The conglomeration of such vascular malformations is also of immense surgical importance, especially during renal and liver transplantation, renal venous sampling, or in the treatment of thromboembolic diseases. In the chest, hemiazygos continuation of IVC can mimic mediastinal lymphadenopathy. Accidental ligation of the hemiazygos vein during thoracic surgery might result in disastrous consequences. 13 There are a few case reports of lower limb thromboembolic diseases associated with duplicated IVC. In patients with deep venous thromboembolism requiring vena caval filters, it is necessary to identify such venous variations as it might require placement of separate filters for both IVC.3,9
The drainage pattern of the persistent left SVC into the left atrium is of particular importance when performing transthoracic echocardiography using agitated saline via the left arm. There has been a case report where the agitated saline given through the left arm entered the left atrium via the persistent left SVC and bubbles entered the brain, causing a transient ischemic attack. 7 The measurement of central venous pressure or gaining access to hepatic veins via the left jugular vein will also pose a problem. 4
Conclusion
The complex ontogenesis of SVC and IVC, with multiple anastomoses formed between the three paired cardinal veins, can result in wide array of congenital malformations. Some of these anomalies have important clinical and surgical significance. The radiologists should be familiar with the anatomy of various venous anomalies in order to guide the clinicians and surgeons in providing proper treatment to the patient.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.