
Abstract
Objective
The aim of this study is to compare outcomes between octogenarians and non-octogenarians undergoing thoracic endovascular aortic repair (TEVAR)
Methods
Using the National Inpatient Sample database, we identified octogenarians (≥80 years) and non-octogenarians (<80 years) who had undergone thoracic endovascular aortic repair between 2012 and 2017. We compared patients’ demographic, socioeconomic, comorbidity data between the two groups as well as the procedure indications and perioperative outcomes. A multivariable logistic regression analysis was conducted to evaluate the impact of advanced age (≥80 years) on the in-hospital mortality rates in patients who underwent TEVAR. This analysis was also performed for a separate cohort which included only patients who underwent TEVAR for ruptured thoracic aortic aneurysm.
Results
A total of 4108 patients were included in our study; 3432 (83.5%) patients were <80 years (37.9% female; median age, 64 years; 34.3% non-white) and 676 (16.5%) patients were ≥80 years (50.7% female; median age, 83 years; 20.4% non-white). Non-ruptured thoracic aortic aneurysm was the most common indication for TEVAR in older patients (61.4%), whereas type B aortic dissection was the most common indication in younger patients (36.4%). In-hospital complications were comparable between the two groups except for respiratory complications that were higher in the younger patients (21.2% vs. 15.2%; P <.001). The multivariable analysis demonstrated that advanced age had no association with increased in-hospital mortality rates (adjusted odds ratio [aOR], 1.41; 95% confidence interval [CI], .97-2.05), However, in ruptured thoracic aortic aneurysm cohort, octogenarians had higher in-hospital mortality rates (aOR, 1.86; 95% CI, 1.04-3.32).
Conclusions
Octogenarians have acceptable rates of perioperative morbidity and mortality compared to the younger group and should be considered for TEVAR. Octogenarians are at higher risk for in-hospital mortality in the setting of ruptured thoracic aortic aneurysm, supporting the appropriateness of elective TEVAR in selected Octogenarians.
Introduction
The elderly population is the fastest growing population in the United States. By 2034, older Americans (≥65 years of age) are expected to outnumber children for the first time in the U.S. history (77 vs. 76.5 million). 1 Through advancements in preventative care and modern-day medicine, survival into the 9th decade of life has become increasingly common. 2 High-income countries, such as the United States, are facing the sharpest increases in longevity.2,3 With a rapidly growing octogenarian population, the prevalence and incidence of cardiovascular disease and aortic pathologies will continue to rise.4-6
Since receiving U.S. Food and Drug Administration authorization in 2005, thoracic endovascular aortic repair (TEVAR) has offered broad applications in the management of thoracic aortic pathologies.7,8 Through its minimally invasive approach, TEVAR offers numerous benefits over open surgical repair including decreased blood loss, decreased end-organ ischemia, decreased risk of paraplegia, decreased length of stay and avoidance of aortic cross-clamping.9-11 In years following FDA approval, TEVAR indications have expanded to include treatment of Type B aortic dissection (TBAD) with malperfusion or rupture, traumatic aortic injury (TAI), and penetrating aortic ulcers (PAU).9,10 With a technical success rate of roughly 98% and fewer perioperative complications and mortality than that of open repairs, TEVAR remains a leading approach for surgical management of thoracic aortic pathologies with suitable anatomy. 12
Previous research has shown that mortality risk from TEVAR in the elderly population is strongly correlated with timing and age. Compared to younger patients, elderly patients demonstrate a three to five times greater mortality risk in settings of urgent or emergent TEVAR.13-15 Increased risks of emergent TEVAR in elderly patients have been associated with greater incidences of hematomas, dysrhythmias, and extracardiac arteriopathies in comparison to younger patients.14,15 However, octogenarians undergoing TEVAR for non-ruptured thoracoabdominal aneurysm or dissections are shown to have comparable mortality and morbidity rates to younger patient populations.14,15 Early diagnosis and elective management of TEVAR in elderly patients can help mitigate the surgical risk and poor outcomes seen in the emergent setting.14,15
Although data in support of elective TEVAR in the elderly population is growing, little is known about the peri-operative morbidity and mortality rates in this population. While single-institution studies, including high-volume centers, have assessed TEVAR outcomes in elderly patients, their conclusions were drawn from small sample sizes. In this study, the National Inpatient Sample (NIS) database was used to present the largest comparative study, to date, of perioperative outcomes in octogenarians vs. non-octogenarians undergoing TEVAR.
Methods
Institutional Review Boards of Tufts Medical Center approved this study (ID: STUDY00001523), and no consent was needed because no identifiable data has been recorded in the NIS database.
Data Source
We performed a retrospective analysis of the NIS dataset between 2012 and 2017 for all patients who underwent TEVAR. NIS is the largest available all-payer inpatient care database in the United States. It contains discharge-level data for over seven million hospital admissions each year, representing 20% of all admissions in U.S. hospitals, excluding long-term acute care centers and rehabilitation hospitals. This dataset provides clinical and non-clinical information at the discharge-level for each hospital admission. NIS database captures up to 40 medical diagnoses and 25 procedures coded using the International Classification of Diseases Clinical Modification, Ninth (ICD-9-CM) and 10th revisions (ICD-10-CM/procedures (PCS)) based on the year of the dataset. The transition into ICD-10-CM/PCS was starting from the last quarter of 2015, while ICD-9-CM was used in all datasets prior to that date. NIS was developed for Health care Cost and Utilization Project (H-CUP) sponsored by the Agency for Health care Research and Quality (AHRQ). More information can be found on the NIS’s webpage: https://www.hcup-us.ahrq.gov/nisoverview.jsp.
Patients
Patients were identified using the TEVAR procedure code(s) (ICD-9-CM: 39.73; ICD-10-CM/PCS: 02VW3 or 02VW4). All patients age 18 years and older who underwent TEVAR as their primary procedure were included in our study. Exclusion criterion was any patient who underwent both open aortic repair and TEVAR, or had a concomitant diagnosis of abdominal or thoracoabdominal aortic aneurysm (intact, ruptured, or with repair), or their primary indication of the procedure was aortic coarctation. Additionally, any patient with connective tissue disease was excluded. Patients with ruptured thoracic aortic aneurysms were excluded from our main analysis and analyzed separately for their in-hospital mortality rates. Our target population was then separated into two cohorts for comparison: Patients with an age of 80 years and older vs. those younger than 80 years (Figure 1). Algorithm describing our study cohorts and the exclusion criteria. The solid line represents our main analysis group while the dashed line represents ruptured thoracic aortic aneurysm group.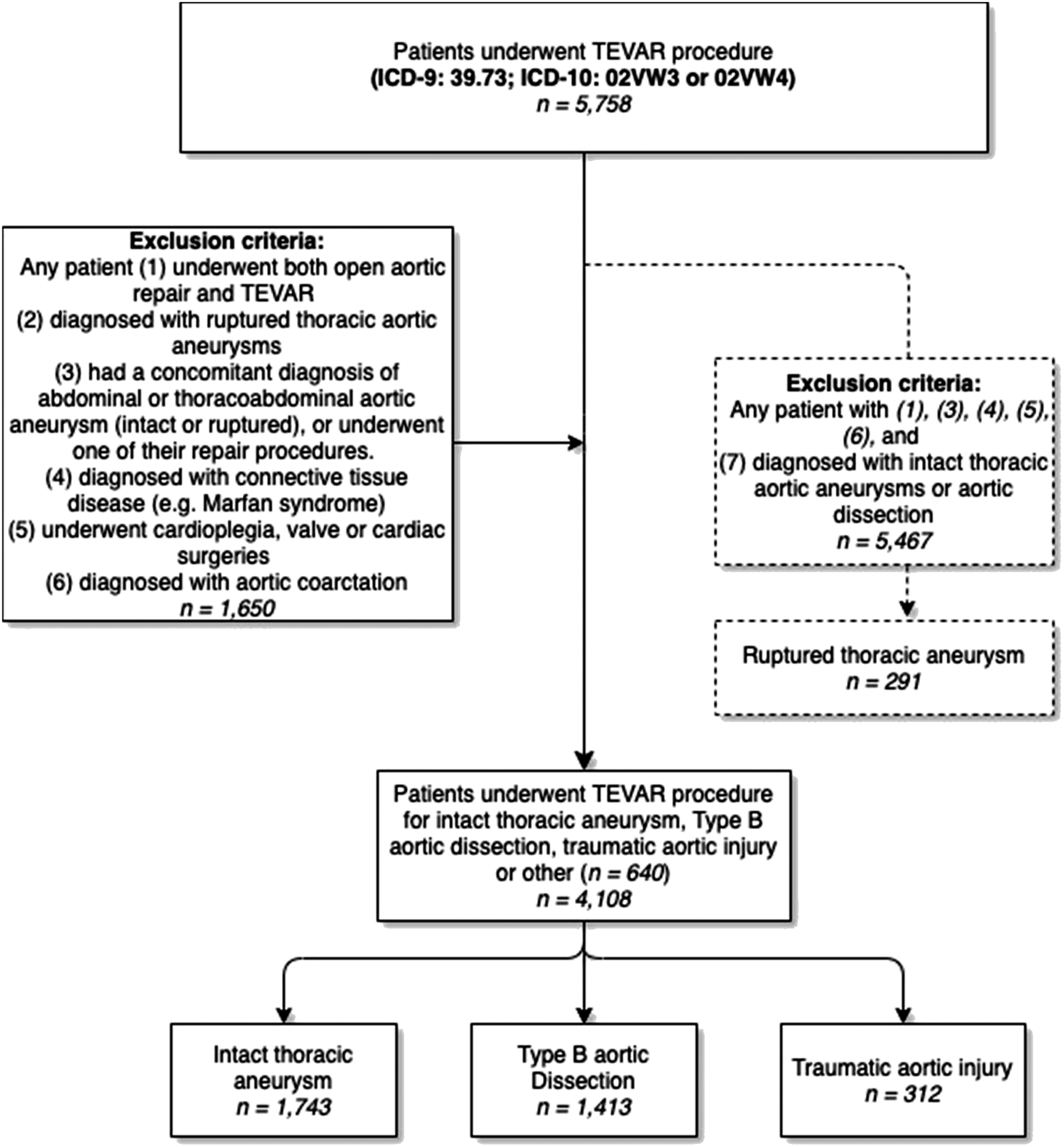
All ICD-9-CM and ICD-10-CM-PCS codes were used to identify the patient’s comorbidities, procedure indications, and in-hospital complications are summarized in Supplementary Table S1. Also, ICD codes used for the exclusion criteria were included (Supplementary Table S2).
Variables and Definitions
Patient’s demographics and comorbidities data such as age at admission, sex, race, smoking, hypertension, diabetes mellitus, chronic kidney disease (defined as glomerular filtration rate <60 mL/min/1.73 m2), coronary artery disease, chronic obstructive pulmonary disease, and cerebrovascular disease were included. Additionally, patients’ socioeconomic data, hospital characteristics, and admission details such as length of stay and admission status were included in our analysis.
Age at admission is the age of the patient in years coded 0-90, patients aged 90 years and more were coded 90 to avoid identification. Therefore, a comparison between the octogenarians and nonagenarians was not possible.
There are no direct ICD-9-CM or ICD-10-CM/PCS codes for TA/BAD; therefore, in order to identify TBAD only, patients who underwent valve repair or surgeries on vessels of the heart were excluded, since these procedures were more likely associated with TAAD. 16
Median household income for patient’s ZIP code is represented by quartiles (bottom quartile, 0-25th percentile (poorest); bottom middle quartile, 26th to 50th percentile; top middle quartile, 51st to 75th percentile; top quartile, 76th to 100th percentile (wealthiest)). Classifying hospitals was based on bed size, location/teaching status and geographic region. Detailed information can be found on the aforementioned dataset’s website according to its year.
Outcomes
Our primary outcome was the comparison of rates of in-hospital complications between the octogenarians and non-octogenarians. Our secondary outcomes were, besides, a comparison of the baseline patients’ demographic and co-morbidities, the analysis of the socioeconomic data, hospital characteristics, and admission details in the two groups.
Statistical Analysis
Continuous variables were reported as mean (±standard deviation) or median (interquartile range (IQR)) where appropriate while categorical variables were expressed as frequency (percentage). The difference in the reported findings between the two groups was assessed using Pearson chi-squared, Fisher exact, student t-, and/or Mann–Whitney U tests where appropriate. A multivariate logistic regression analysis was conducted for in-hospital mortality rates in patients who underwent TEVAR regardless of the procedure’s indication and with ruptured thoracic aneurysm as the only indication. The first model was adjusted for smoking, diabetes mellitus, hypertension, chronic kidney disease, chronic pulmonary disease, and cerebrovascular disease, whereas the second one was adjusted for hypertension, diabetes, chronic kidney disease, and coronary artery disease. The selection of the variables included in the multivariate model was based on their significance in the univariate analysis or their clinical relevance. SPSS version 25.0 (IBM Corp, Armonk, NY) and JMP version 14.0 (SAS Institute Inc, Cary, NC) were used for all statistical analyses. P-values were considered statistically significant if P < .05 (two-tailed).
Results
A total of 4108 patients in the NIS database underwent a TEVAR from 2012 to 2017; 3432 (83.5%) were younger than 80 years of age (median age: 64-years; IQR, 54-72), and 676 (16.5%) were aged 80 and older (median: 83; IQR, 80-86). Older patients were more likely to be female (50.7% vs. 37.9% in the younger group; P < .001).
Demographics and Patient Comorbidities n = 4108.
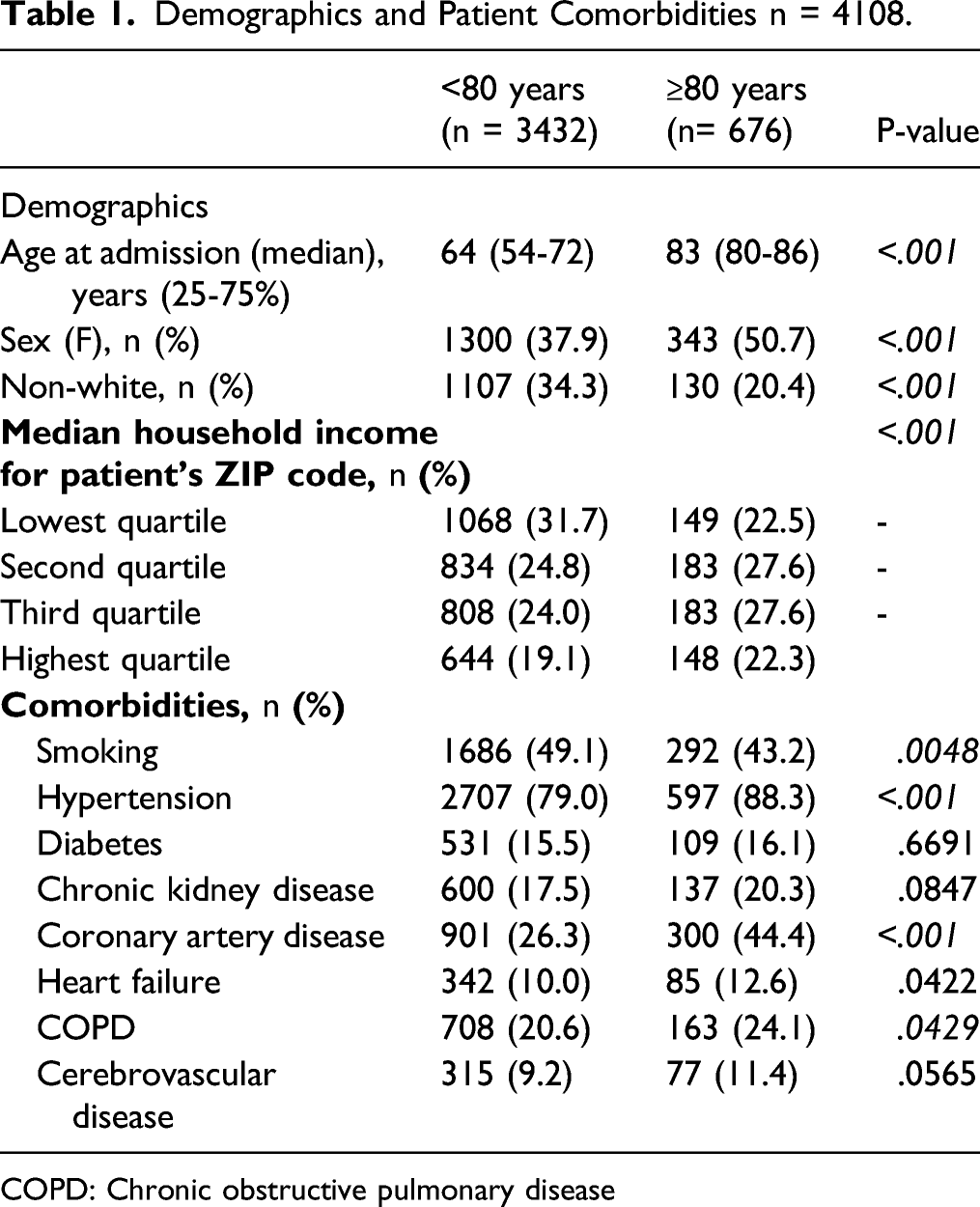
COPD: Chronic obstructive pulmonary disease
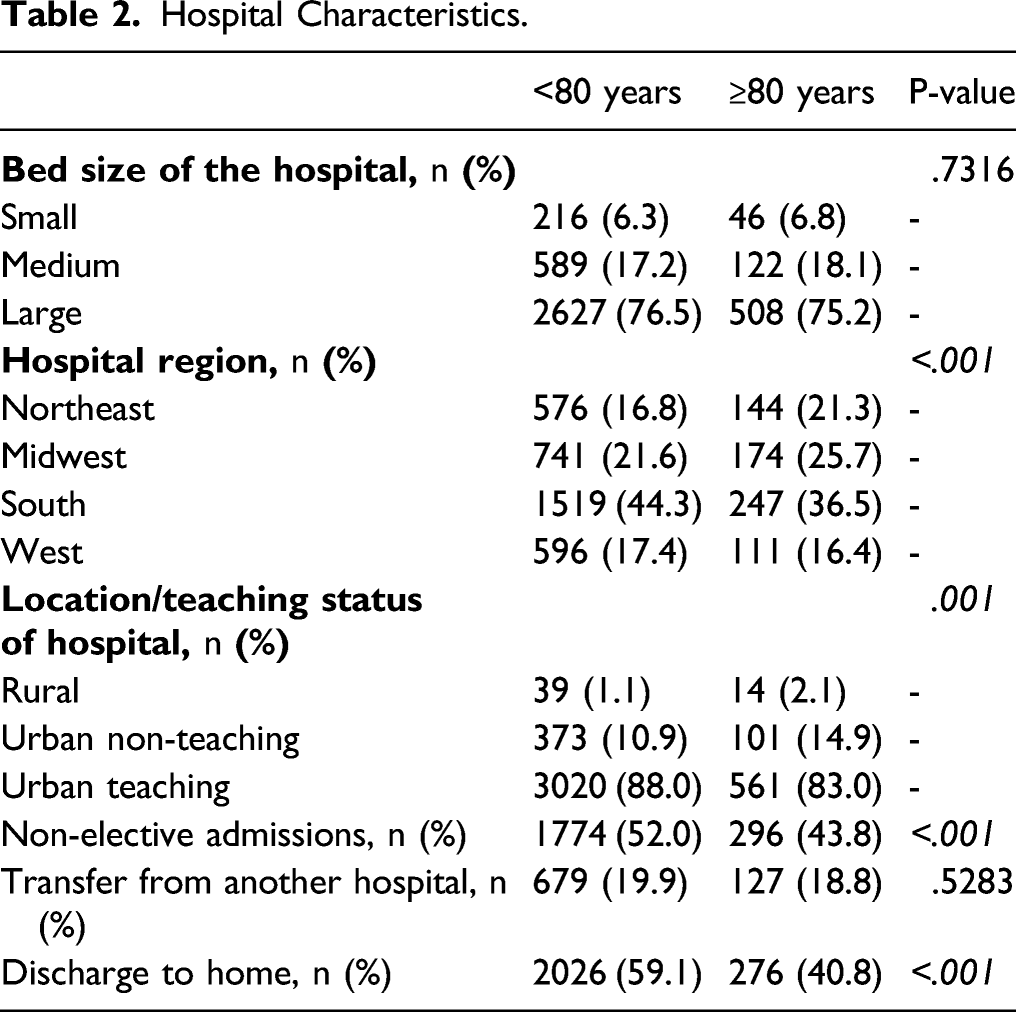
Hospital Characteristics.
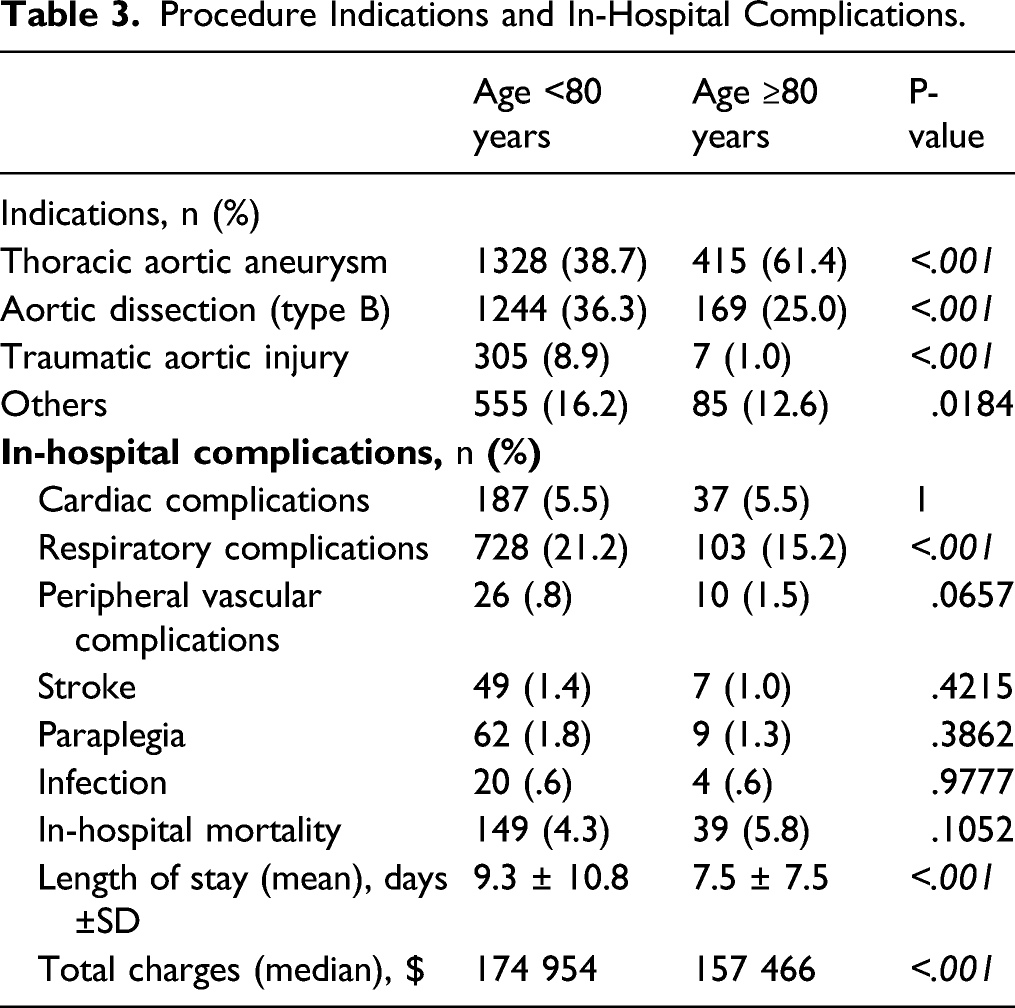
The primary indication for TEVAR reported in both the groups were intact thoracic aortic aneurysm, TBAD and TAI; TBAD and TAI had a higher prevalence in the younger group (36.3% vs. 25.0% and 8.9% vs. 1.0%, respectively; P <.001 for both). Intact thoracic aortic aneurysm had a higher prevalence in the older group (61.4% vs. 38.7%; P <.001). Other indications for TEVAR included re-intervention and aortoenteric fistula.
Interestingly, the younger population had a prolonged hospital length of stay (9.3 ± 10.8 vs. 7.5 ± 7.5; P <.001) and higher total hospital charges (P = <.001).
Procedure Indications and In-Hospital Complications.
In the cohort of patients who underwent TEVAR for ruptured thoracic aortic aneurysm, which were not included in the main statistical analysis, we found that older patients were at a higher risk of in-hospital death compared to the younger group (27.1% vs. 17.4%, respectively; P = .0497).
Figure 2 shows the overall and in-group in-hospital mortality rates over the duration of the study. In both groups, mortality rates did not change significantly from 2012 to 2017 (<80 group, 5.70 to 3.81; P = .1729 vs. ≥ 80 group, 5.49 to 6.78; P = .5480). In the older age group, from 2012 onward, the inpatient deaths were largely stable until 2015 where the mortality increased 1.4 to 1.5-fold in the last two years. On the contrary, the mortality rates in the younger patients decreased over the study period. A graph demonstrating the in-hospital mortality rates among octogenarians (dashed) and non-octogenarians (dotted) throughout the study period.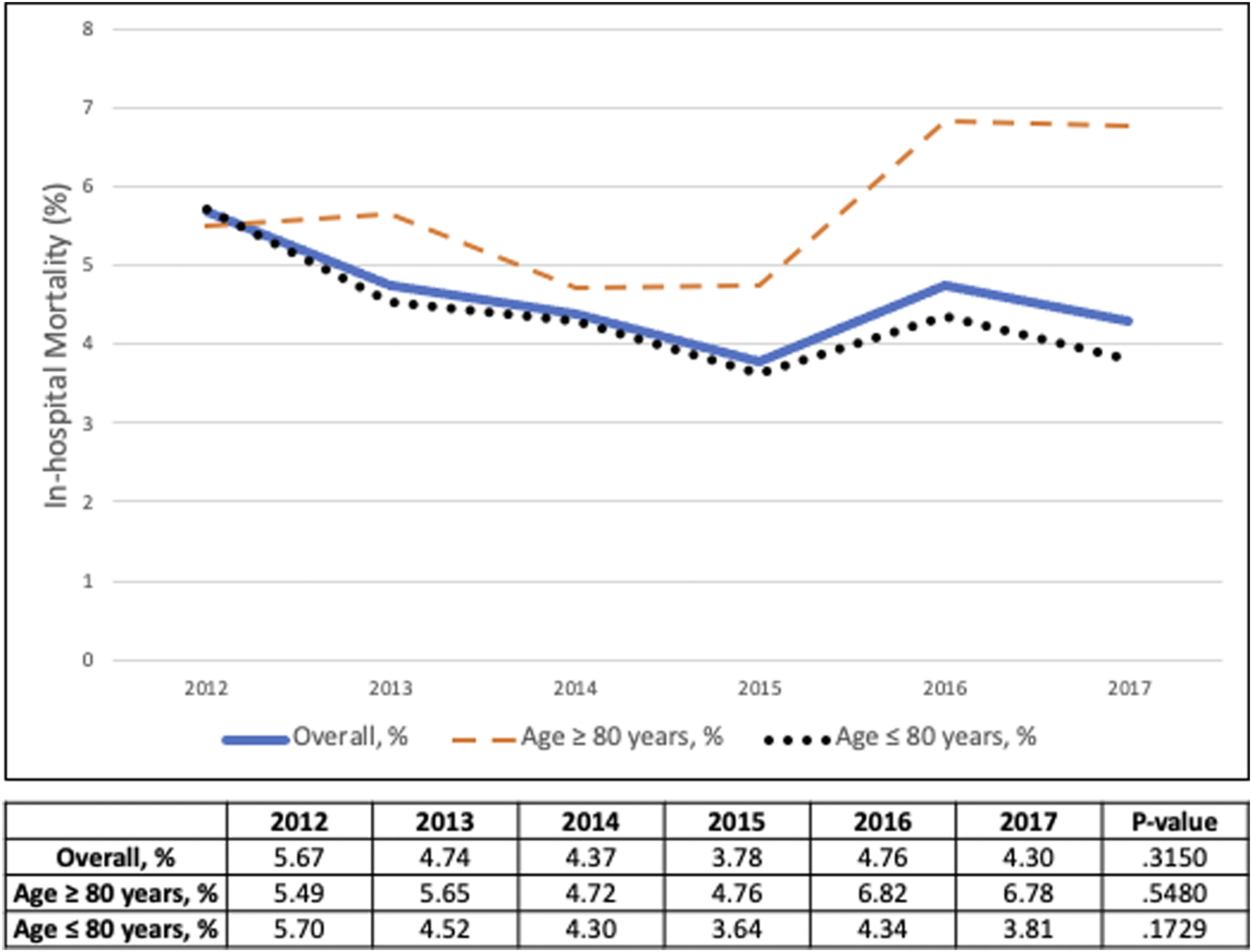
Multivariable Logistic Regression For in-Hospital Death in Patients Who Underwent TEVAR (Main Cohort).
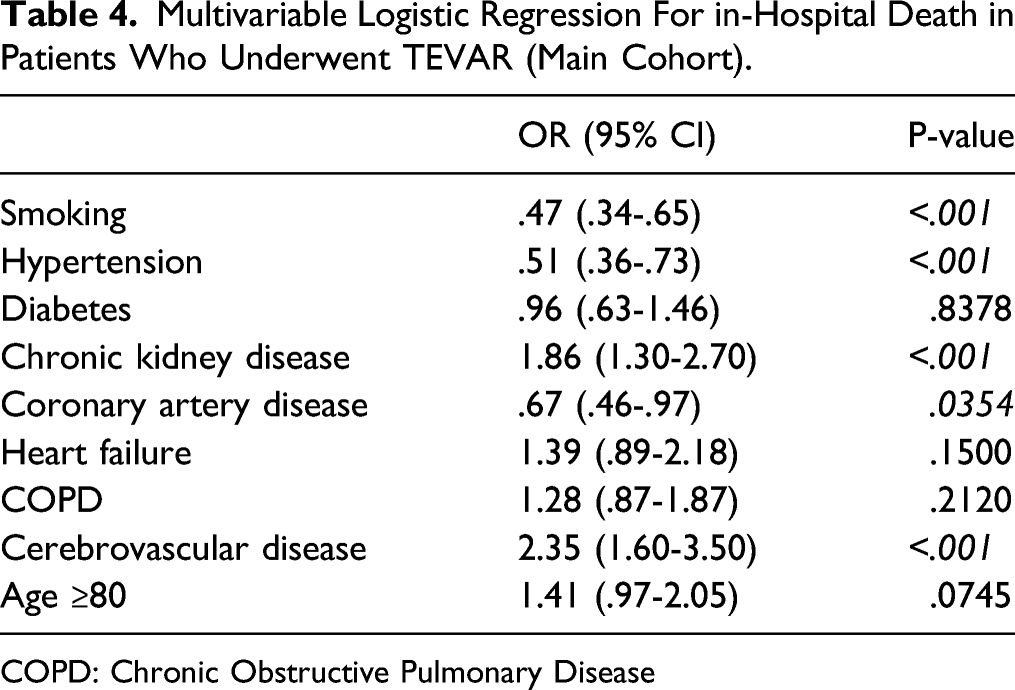
COPD: Chronic Obstructive Pulmonary Disease
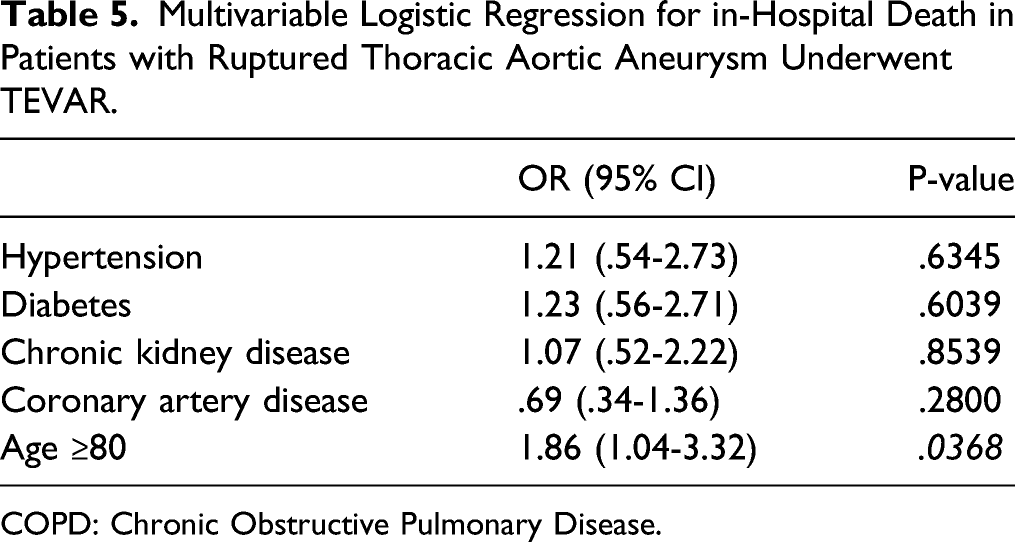
Multivariable Logistic Regression for in-Hospital Death in Patients with Ruptured Thoracic Aortic Aneurysm Underwent TEVAR.
COPD: Chronic Obstructive Pulmonary Disease.
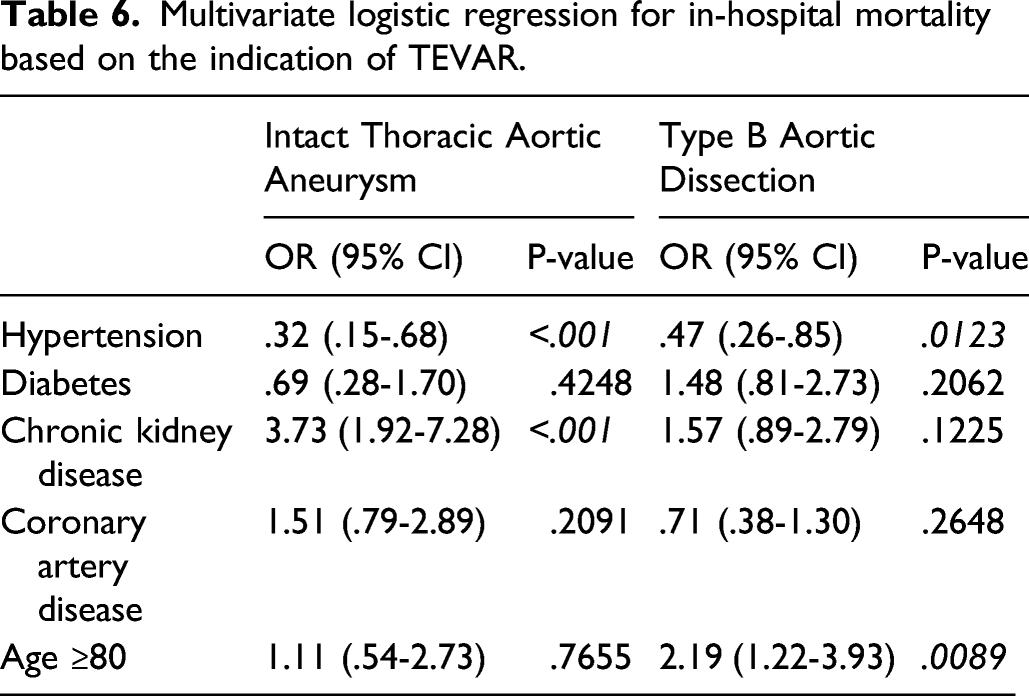
Multivariate logistic regression for in-hospital mortality based on the indication of TEVAR.
Discussion
In this study, a retrospective cohort analysis was performed to assess the clinical outcomes of octogenarians compared to non-octogenarians undergoing TEVAR. As the geriatric population continues to grow, more octogenarians are expected to undergo TEVAR as primary management for thoracic aortic pathology.
There are distinct demographic differences between the two groups, including higher rates of hypertension, coronary artery disease (CAD), and chronic obstructive pulmonary disease (COPD) among the octogenarians. With age, two phenomena occur: physiological decline and an increase in the prevalence of disease. 17 A survey of elderly members of a health maintenance organization (HMO) found an average of 8.7 chronic diseases per person.18,19 Patients with multiple comorbidities have poorer physical functioning, a higher morbidity, and increased mortality. 18 As a result, the elderly are perceived, and not incorrectly, as a sicker population. Therefore, it is critical to establish the safety profile of TEVAR in this population.
Other differences include more women and more Caucasians in the octogenarian group. The impact of gender on health outcomes can be determined by metabolic differences, differences in life span, as well as response to diseases. 18 Given men have higher mortality rates than women across the world, it would not be unexpected to see a higher rate of women in an older population. 18 In patients undergoing TEVAR, the indications also differ between the two groups. In non-octogenarians, TBAD (40.7%) and thoracic aortic aneurysm (38.3%) are the primary indications for TEVAR, whereas in octogenarians, the primary indication appears to be thoracic aortic aneurysm (61.4%). Previous studies have shown that elderly patients with TBAD have a greater risk of aneurysm expansion leading to rupture and higher rates of in-hospital mortality.20,21 Stable elderly patients were often managed medically as opposed to an invasive approach, possibly secondary to the perception of increased risk within the population. 22 Both of these factors, along with generally the lower incidence of TBAD, 23 likely have influenced the lower rate of TEVAR in octogenarians with TBAD.
The findings of this study show that octogenarians have similar in-hospital mortality to non-octogenarians (5.8% vs. 4.3%, P = .11) undergoing TEVAR. Conversely, when specifically evaluating TEVAR in ruptured thoracic aortic aneurysms, octogenarians display a higher mortality (27.1% vs. 17.4%, P = .0479), suggesting the higher impact of the advanced age on the mortality rates of patients who underwent endovascular repair for the ruptured thoracic aortic aneurysm compared to the intact one. In non-ruptured patients, there was no difference in cardiac complications, stroke, peripheral vascular complications, infections, paraplegia, or hospital costs. The octogenarian group did have a shorter length of stay (7.5 vs. 9.2 days, P < .001) and lower rate of respiratory complications, possibly secondary to a more selective criteria used to take them to surgery as shown by a lower number of emergent cases (43.8% vs. 51.6%).
Multivariable regression analysis revealed age was not a significant predictor of in-hospital mortality in non-ruptured patients. In contrast, smoking, hypertension, chronic kidney disease, CAD, and cerebrovascular disease were statistically significant predictors of death. This is an immensely significant finding as it indicates that octogenarians with non-ruptured aortic pathology amenable to TEVAR are likely acceptable candidates and age alone should not be a deterrent to proceeding with the procedure. However, in ruptured thoracic aortic aneurysms, age was not only a significant predictor of death, but it was also the only predictor of death. This finding signifies that screening elderly patients for TEVAR, especially by indication, may have an impact on outcomes, including in-hospital mortality. Hemodynamic instability from rupture compounded by high-risk comorbidities seen in octogenarians may be the reason why mortality is higher in this group. As a result, octogenarians with ruptured thoracic aneurysms may not be the best candidates, further supporting elective TEVAR in appropriately selected patients in this group.
To our knowledge, there have been no prospective studies evaluating differences in outcomes between octogenarians and non-octogenarians undergoing TEVAR and further study may help us understand the role of age in predicting outcomes. This study has shown that when appropriately selected, octogenarians have an acceptable rate of perioperative morbidity and mortality and should be considered for TEVAR.
This study has several limitations: the administrative nature of the NIS dataset could result in potential coding errors; also, this did not allow us to provide detailed clinical data regarding anatomical characteristics of aorta, TBAD classification (complicated vs. uncomplicated), and access information. Moreover, the transition from ICD-9 to ICD-10 in NIS dataset in October 2015 may result in another limitation through using two different ICD codes (ICD-9 and ICD-10) which would affect the consistency of capturing of included patients or their clinical outcomes throughout the years of study. Furthermore, there is no specific ICD code found to identify TBAD, which would lower the accuracy in capturing patients with this indication; also, we could not exclude patients underwent TEVAR for a primary procedure of aortoenteric fistula or re-intervention due to same reason. The lack of long-term data in this discharge abstract-level NIS dataset would limit our ability to investigate the procedure’s long-term outcomes.
Conclusions
Octogenarians have acceptable rates of perioperative morbidity and mortality compared to the younger group and should be considered for TEVAR. However, for those with ruptured thoracic aortic aneurysm, they were at higher risk for in-hospital mortality, than the younger patients. This may support the appropriateness of elective TEVAR in selected octogenarians.
Supplemental Material
sj-pdf-1-ves-10.1177_15385744211051502 – Supplemental Material for Outcomes of Thoracic Endovascular Aortic Repair in Octogenarians
Supplemental Material, sj-pdf-1-ves-10.1177_15385744211051502 for Outcomes of Thoracic Endovascular Aortic Repair in Octogenarians by Khaled I. Alnahhal, Qianyun He, Zhengyu Zhang, Chunli Qi, Lina Ding, Tingting Yuan, Yanhong Chen and Zhihua Li in Human & Experimental Toxicology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.