
Abstract
Bronchial artery (BA) pseudoaneurysm is an uncommon vascular complication of tuberculosis (TB), and early diagnosis is crucial due to risk of rupture and life-threatening hemorrhage. Immediate intervention is warranted in massive hemoptysis due to high mortality. Various causes of massive hemoptysis are TB, bronchiectasis, aspergilloma, lung abscess, lung cancer, necrotizing pneumonia, and cystic fibrosis. Active pulmonary TB as well as chronic pulmonary TB can manifest with massive hemoptysis. Hemoptysis in active TB occurs due to ulceration in bronchiolar wall, eroding the wall of the adjacent BA or pulmonary artery, and in chronic TB due to hypertrophied bronchial arteries, or bronchiectasis, or aspergilloma. Herein, we report a case of pulmonary TB causing intrapulmonary BA pseudoaneurysm in a young male patient who presented with acute massive hemoptysis. The BA pseudoaneurysm as well as other hypertrophied bronchial arteries were embolized using polyvinyl alcohol (PVA) particles.
Keywords
Introduction
Bronchial artery (BA) pseudoaneurysm is a rare vascular complication. Early diagnosis and management are crucial because of life-threatening hemorrhage and increased mortality. Bronchial arteries are the main source of blood supply to the bronchi and bronchioles. It provides nourishment to the bronchus and bronchioles by forming arterial networks on the wall and in the submucosa. The vasa vasorum of the adjacent pulmonary arteries are also supplied by the bronchial arteries. BA pseudoaneurysms can occur in active pulmonary tuberculosis (TB) due to erosion of the wall of BA or focal vessel wall weakening by ulceration or inflammation. We report a case of pulmonary TB causing intrapulmonary BA pseudoaneurysm in a young male patient successfully treated with embolization using polyvinyl alcohol (PVA) particles.
Case Report
A 28-year-old male patient who was diagnosed with pulmonary TB two years back, defaulted on anti-tubercular treatment. Now, the patient presented to our emergency department with complaints of massive hemoptysis of 4 days’ duration. The patient experienced 4 episodes of hemoptysis with a maximum of 300 mL in the episode on the day of admission. On examination, the patient was conscious, oriented with pulse rate of 141 bpm, blood pressure of 113/75 mmHg, respiratory rate of 26/min, and SpO2 of 83%. His hemoglobin was 12.7 g/dL.
Chest radiograph and CT angiography (CTA) were done and showed a thick-walled cavity in right upper lobe and consolidation in right middle and lower lobes, suggestive of active TB (Figures 1A and 1B). The background lung showed fibrobronchiectasis of post-infective sequelae. Differential diagnosis of chronic pulmonary aspergillosis was also considered; however, laboratory parameters such as Aspergillus-specific IgE were not corroborative. Bilateral lung parenchyma also showed diffuse ground-glass opacities in the dependent portions, suggestive of aspiration changes. Necrotic conglomerated nodes were also seen in the right hilum with soft tissue in the lumen of right middle lobe and lower lobe bronchi, likely blood clots (Figures 1C and 1D). In addition, necrotizing consolidation was seen in peribronchial regions adjacent to right middle lobe and proximal right lower lobe bronchi with loss of definition of the bronchial walls (Figure 1E). Maximum intensity projection reconstruction images showed dilated and tortuous right common intercostal–bronchial artery trunk (ICBAT) and tortuous common bronchial artery (Figure 1F). Fiber-optic bronchoscopy (FOB) was also done and showed blood clots in the right middle lobe and lower lobe bronchi (Figure 1G). Multimodality imaging in a 28-year-old male patient with massive hemoptysis. (A) Chest radiograph showing thick-walled cavity in the right upper zone and consolidation in right middle and lower zone with prominent right hila. (B) Lung window showing thick-walled cavities in the right upper lobe. (C) Multiple centrilobular nodules and patchy areas of consolidation in right middle and lower lobe with soft tissue content (arrow) in the lumen of right middle lobe bronchus (likely nodobronchial fistula). (D) Axial mediastinal window showing enlarged right hilar lymph node (arrow). (E) Axial image shows an ill-defined area of consolidation in the right hilar region with loss of definition of RLL bronchus (arrow) and intraluminal bronchial soft tissue. (F) Coronal maximum intensity projection image showing the dilated and tortuous right intercostobronchial artery (arrow). (G) Bronchoscopy image showing a blood clot in the lumen of right middle lobe bronchus (arrow).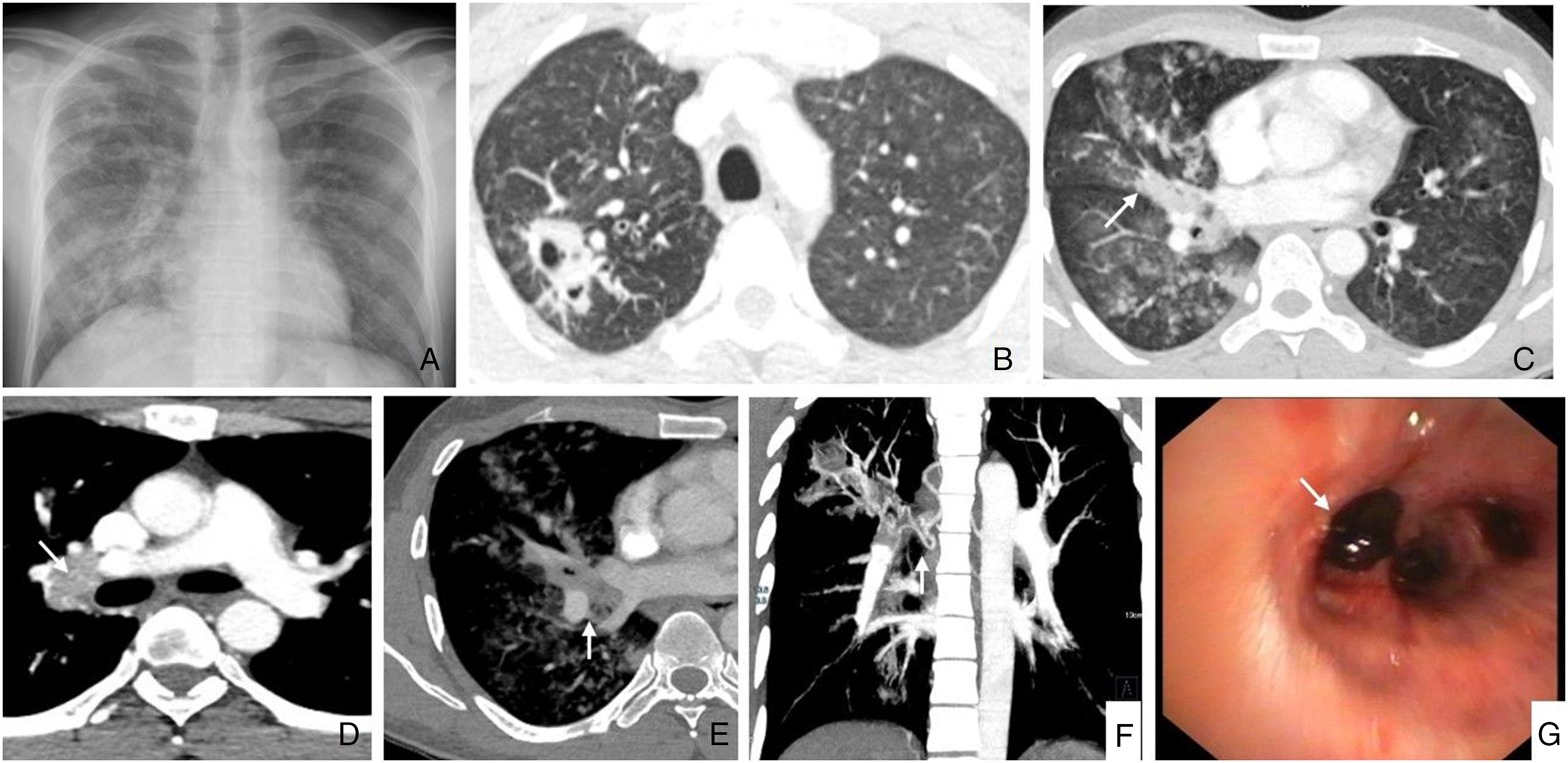
Bronchial artery embolization was planned in view of acute massive hemoptysis. The right ICBAT and common bronchial artery angiogram were obtained. These showed the tortuous and hypertrophied bronchial component of right ICBAT. In addition, a small pseudoaneurysm arising from the distal part of the right branch of the common BA was also identified (Figures 2A and 2B). The pseudoaneurysm measured approximately 4.5 × 3.7 mm and was intrapulmonary in location, 3.8 cm from the right hilum and 9.5 cm from the ostium of common BA. The pseudoaneurysm was not associated with the cavity, but location correlated with the ill-defined area of consolidation in the right hilar region on CT. Engorged BAs were embolized using PVA particles (355–500 μ). Post-embolization contrast run showed elimination of blush and non-opacification of the pseudoaneurysm (Figures 2C-2E). On follow-up, the patient was restarted on anti-tubercular treatment and there was no hemoptysis after the procedure for a follow-up period of one month. Digital subtraction angiography in a 28-year-old male patient with massive hemoptysis. (A) Common bronchial trunk angiogram showing right and left branches with a tortuous right branch and a small pseudoaneurysm (arrow) arising from the distal part of the right branch. Embolization was done using PVA particles. (B) Magnified image clearly showing the pseudoaneurysm (arrow). (C) Post-embolization contrast run showing neither opacification of right and left branch of common bronchial trunk nor the aneurysm. (D) Right intercostobronchial artery angiogram showing hypertrophied and tortuous right bronchial component. Embolization was done using polyvinyl alcohol particles. (E) Post-embolization contrast run showing non-opacified right bronchial component of intercostobronchial artery.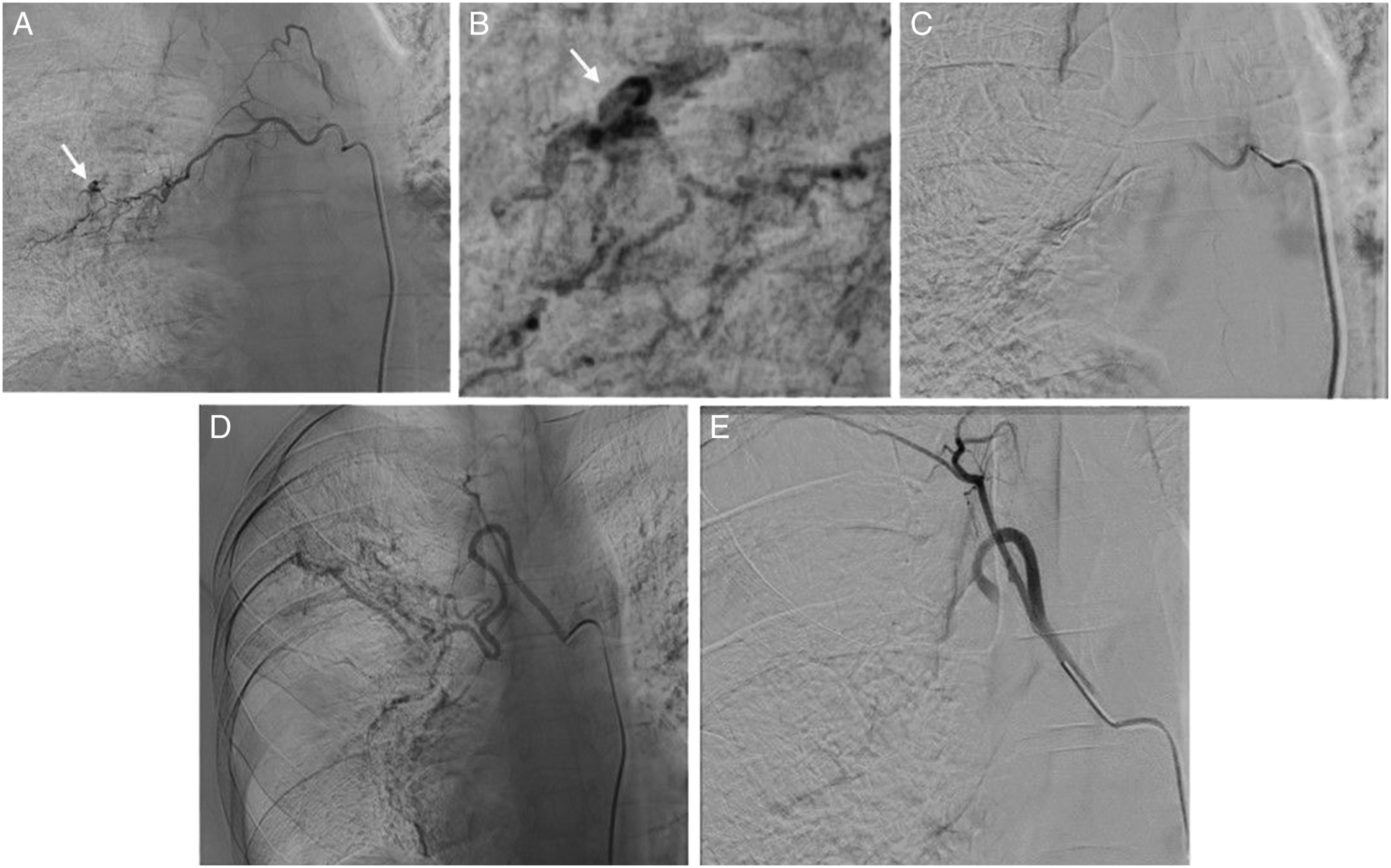
Discussion
Pulmonary TB is the most common cause of hemoptysis in TB endemic regions. Hemoptysis in TB occurs both due to active disease and sequelae (bronchiectasis or fungal ball). Vascular causes such as hypertrophied bronchial arteries (BAs), Rasmussen aneurysm, and rarely BA aneurysm may manifest with massive hemoptysis.
In lungs with post-tubercular sequelae, chronic inflammation leads to recruitment of new systemic vessels (BAs or non-bronchial systemic arteries) in the affected segments of the lungs. These vessels are at systemic pressures and prone to rupture and hence are the major reason for hemoptysis. 1 Rarely calcified nodes are also often found as the culprit when they erode into the bronchial tree. This is seen as calcified masses in the airway known as broncholithiasis and can also present with hemoptysis. 2
In active TB, hemoptysis occurs due to ulceration in bronchiolar wall, eroding the wall of the adjacent BA or pulmonary artery. Pulmonary artery pseudoaneurysms known as Rasmussen aneurysms are much more common than the BA variety and develop in walls of cavities. Our index case presented with massive hemoptysis and BA angiogram showed an intrapulmonary BA pseudoaneurysm arising from the right branch of the common BA. Adjoining this aneurysm was an ill-defined area of necrotizing consolidation with loss of definition of the right lower lobe bronchus, intraluminal bronchial soft tissue, and right hilar lymph node.
Overall, BA aneurysms are detected in less than 1% of patients who undergo selective BA angiography.3,4 They can be congenital or acquired. The congenital type is associated with pulmonary sequestration and pulmonary artery agenesis. 5 Bronchiectasis and TB are the common acquired causes. In cases of TB presenting with massive hemoptysis, the BA aneurysms are reported in upto 7% of the cases.6,7 The other underlying conditions could be cystic fibrosis and hereditary hemorrhagic telangiectasia. 8
CTA/FOB may not demonstrate the BA pseudoaneurysm. One of the case reports described a small intrapulmonary aneurysm well visualized on CTA. 6 In the other case, the aneurysm was not detected on CT and only seen on the FOB. 7 In our index case, the BA pseudoaneurysm was not visualized in CT and only visualized on BA angiogram.
BA aneurysms are classified into two types—mediastinal and intrapulmonary based on its anatomical location.9,10 The diagnosis of mediastinal BA aneurysms are easy on CTA when compared to the intrapulmonary type because of large size and juxta-aortic location. The former presents like a mediastinal mass causing compression of the adjacent structures or rupture into the pleural cavity, mediastinum, or into the esophagus. 5 The intrapulmonary type usually presents with massive or intermittent hemoptysis due to rupture. Surgical or endovascular management should be considered in both types regardless of size because of risk of life-threatening hemorrhage and increased mortality. Endovascular management is preferred nowadays in hemodynamically stable patients or in selected hemodynamically unstable patients who are poor surgical candidates due to its advantages of decreased hospital stay and post-operative morbidity. Various endovascular management options are available for each type. Size of the aneurysm, number of feeding arteries, and outflow vessels should be assessed in angiography for appropriate management planning. Juxta-aortic mediastinal aneurysm is usually treated with an aortic stent graft/detachable coils.9,10 Coil placement may be particularly challenging in cases of multiple thin tortuous feeding vessels and a short segment of vessel between aneurysm and aorta.9,11
Detachable coils are preferred in the intrapulmonary BA aneurysm with a large caliber feeding artery. When the feeding artery caliber is small or super-selective catheterization is unsuccessful, other embolic agents like gelatin sponge, N-butyl-2-cyanoacrylate (NBCA) glue, and PVA particles are resorted to.5,12 Each embolic agent has their own advantages and limitations. Gelatin sponge is cost effective and causes less tissue necrosis but it has a high rate of recanalization and recurrence. N-butyl-2-cyanoacrylate glue can cause rapid complete vessel occlusion but is more prone to extensive tissue necrosis and non-target embolization. 12 In our case, PVA particles were used through a microcatheter due to the small caliber of the feeding artery. Advantages of using PVA particles include availability in a variety of sizes, characteristics of a permanent occluding agent, and lesser risk of non-target embolization compared to NBCA glue. Clumping within the microcatheter leading to more proximal occlusion or catheter blockage and more recanalization rates than NBCA are some of the disadvantages of PVA. 13
Our index case presented with intrapulmonary type of BA pseudoaneurysm fed through the common BA; however, the microcatheter could not be super-selectively negotiated beyond the first curve because of its small caliber (.4 mm in diameter). Hence, we used PVA particles (355–500 μ) for embolizing the aneurysm as well as other hypertrophied BA, and the procedure was technically and clinically successful.
Conclusion
Small intrapulmonary BA pseudoaneurysms are difficult to identify on CTA and in BA angiogram; however, meticulous search is warranted in patients who present with massive hemoptysis. Endovascular embolization using PVA particles successfully treated the intrapulmonary BA pseudoaneurysm in the index case and may be used as an alternative to coil embolization when there is a small-caliber feeding artery or difficulty in super-selective catheterization of the feeding artery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.