
Abstract
Introduction
While there exists copious short-term data regarding renal function following infra-renal endovascular abdominal aortic aneurysm repair (EVAR), long-term analysis is sparse. This is a single institution retrospective review of predictors of renal function decline 5 years after elective EVAR.
Methods
All EVAR between 2007 and 2015 were queried. Patients in whom renal function was documented 5 years postoperatively were included in analysis. Exclusion criteria were ruptured aneurysm, mortality before 56 months, lack of follow-up, ESRD status, and concomitant renal intervention. The primary outcome investigated was a 20% or greater drop in glomerular filtration rate (GFR) 5 years postoperatively. The following variables at the time of surgery were investigated as potential predictors: age, gender, hypertension, hyperlipidemia, diabetes, CAD or prior MI, COPD, prior stroke, baseline eGFR under 60 mL/min/1.73 m2, supra-renal fixation, infra-renal fixation, neck diameter, neck length, and number of contrast CT.
Results
354 EVAR were identified of which 143 met inclusion criteria (211 excluded). Univariate analysis revealed female gender (OR 2.7), hypertension (OR 9.4), baseline renal insufficiency (OR 3.8), larger neck diameter, and supra-renal fixation (OR 2.32) all predictive (P < .05) of GFR drop at 5 years. Multivariate binary logistic regression analysis found female gender (multivariate OR 3.9, P = .023) and baseline renal insufficiency (multivariate OR 3.0, P = .029) as significant predictors of greater than 20% GFR drop at 5 years. Only 2 patients of the 143 progressed to dialysis requirement at 5 years.
Conclusions
Females and patients with baseline renal insufficiency are more vulnerable to significant decline in renal function 5 years following EVAR. Consistent with analogous literature, supra-renal fixation appears moderately deleterious toward renal function with no clinical significance in those with baseline normal renal function. The potential benefit of avoidance of supra-renal fixation in female patients with baseline renal insufficiency is worth further investigation in a more robust multi-center study.
Introduction
While there exists copious short-term data regarding predictors of renal function decline following infra-renal endovascular abdominal aortic aneurysm repair (EVAR), long-term analysis is sparse.1-5 This is a single institution retrospective review of predictors of renal function decline 5 years after elective EVAR.
There are no prior studies with universal 5 year follow-up post-EVAR which investigate gender, age, infra-renal neck length and diameter, hypertension, prior stroke, chronic obstructive pulmonary disease (COPD), diabetes, and the number of CT scan with iodinated contrast as potential predictors of decline in renal function.
EVAR can be performed utilizing stent grafts with either infra-renal (iEVAR) or supra-renal fixation (sEVAR). Whether supra-renal fixation has a deleterious effect on renal function is an area of debate. There is abundance of comparative data regarding renal function outcome at 30 days and 1 year renal post-iEVAR and sEVAR. The overall trend in these short-term analyses leans toward a modest decline in renal function with sEVAR relative to iEVAR.6-13 However, the clinical significance of this trend has not been found to be impactful regarding new onset of dialysis requirement.6-8 Mid-term (2–3 year) analysis post-EVAR trends more significantly toward a finding of declining renal function following sEVAR vs iEVAR. 13 Only 2 prior studies have investigated type of fixation as a potential predictor of decline in GFR 5 years after EVAR.1,2
Methods
All EVAR performed at Loyola University Medical Center between 2007 and 2015 were queried. Institutional Review Board authorization was obtained for this retrospective review. Patients in whom renal function was documented 5 years postoperatively were included in analysis. Exclusion criteria were ruptured aneurysm, mortality before 54 months, lack of follow-up, baseline end stage renal disease (ESRD) status, and concomitant renal artery intervention. The primary outcome investigated was a 20% or greater drop in glomerular filtration rate (GFR) 5 years after surgery. GFR level was considered to be at the 5 year interval if it was obtained between 54 and 66 months postoperatively. The value closest in time to 60 months was utilized when multiple data points were present.
The following variables at the time of surgery were investigated as potential predictors of 20% or greater drop in GFR at 5 years: age, gender, hypertension, hyperlipidemia, diabetes, CAD or prior myocardial infarction (MI), COPD, prior stroke, baseline GFR under 60 mL/min/1.73 m2, supra-renal fixation, infra-renal fixation, infra-renal neck diameter in millimeters (mm) measured at a level 5 mm beneath the lowest of the 2 main renal arteries, infra-renal neck length (mm), and number of documented CT scans with iodinated intravenous contrast in the 5 year postoperative period performed at our institution.
In terms of our routine practice, we follow Society of Vascular Surgery recommended indications for AAA repair at a diameter of 5.5 cm in men and 5 cm in women. 14 Consideration of repair at smaller diameters is made for symptomatic aneurysms, saccular morphology, and rapid aneurysm growth. Iso-osmotic hydration is used for patients with GFR under 50 before and after administration of iodinated contrast. Our laboratory reported all GFR with a value of 60 or higher as 60 mL/min/1.73 m2 before 2016, and thus this was the highest value obtainable for baseline GFR in this study. Post-EVAR long-term surveillance is recommended to all patients with a provider-dependent combination of duplex ultrasound and CT angiogram (CTA). Imaging is typically obtained between 1 and 3 months postoperatively, at 6 months, 1 year, and annually thereafter with more frequent imaging when endoleak or aneurysm sac growth is detected. In the past 15 years, we have had a shift to increased use of duplex imaging and fewer CTA exams to minimize long-term contrast and radiation exposure. Procedures were performed by vascular surgery (90%) and a combination of invasive cardiology and cardiothoracic surgery (10%).
Statistical analysis was carried out using IBM SPSS software, version 26. Univariate analysis was conducted with Chi-Square or Fisher Exact statistic for categorical variables and student t-test for comparison of means. Two-tailed P value of less than .05 was considered statistically significant. Binary logistic regression analysis was used to investigate multivariate predictors of greater than 20% drop in GFR at the 5-year postoperative interval. All of the variables were included in the multivariate analysis.
Results
Patient Demographics and Characteristics.
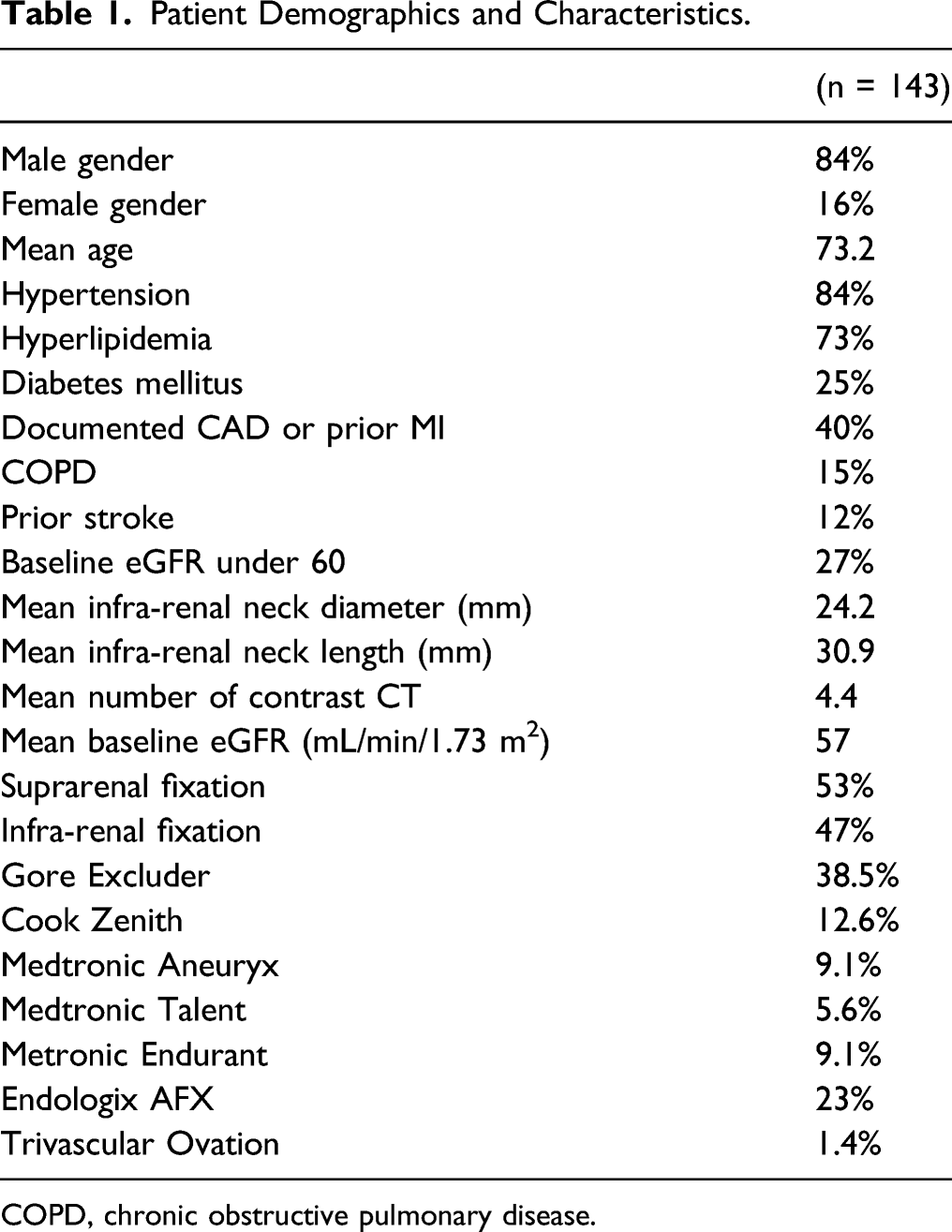
COPD, chronic obstructive pulmonary disease.
Predictors of Greater Than 20% Drop in GFR 5 Years After EVAR.
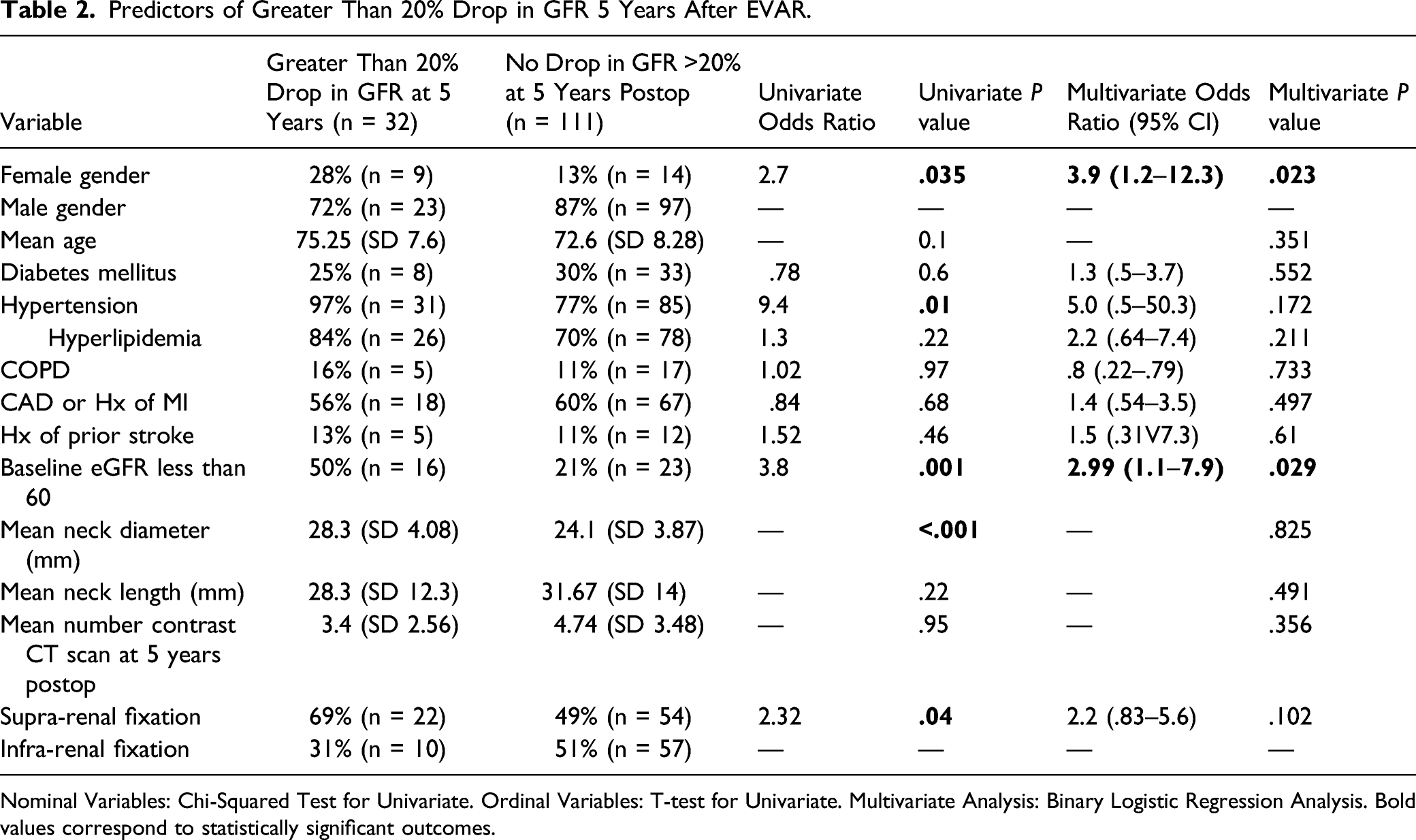
Nominal Variables: Chi-Squared Test for Univariate. Ordinal Variables: T-test for Univariate. Multivariate Analysis: Binary Logistic Regression Analysis. Bold values correspond to statistically significant outcomes.
Female Gender in Conjunction with Supra-renal Fixation.

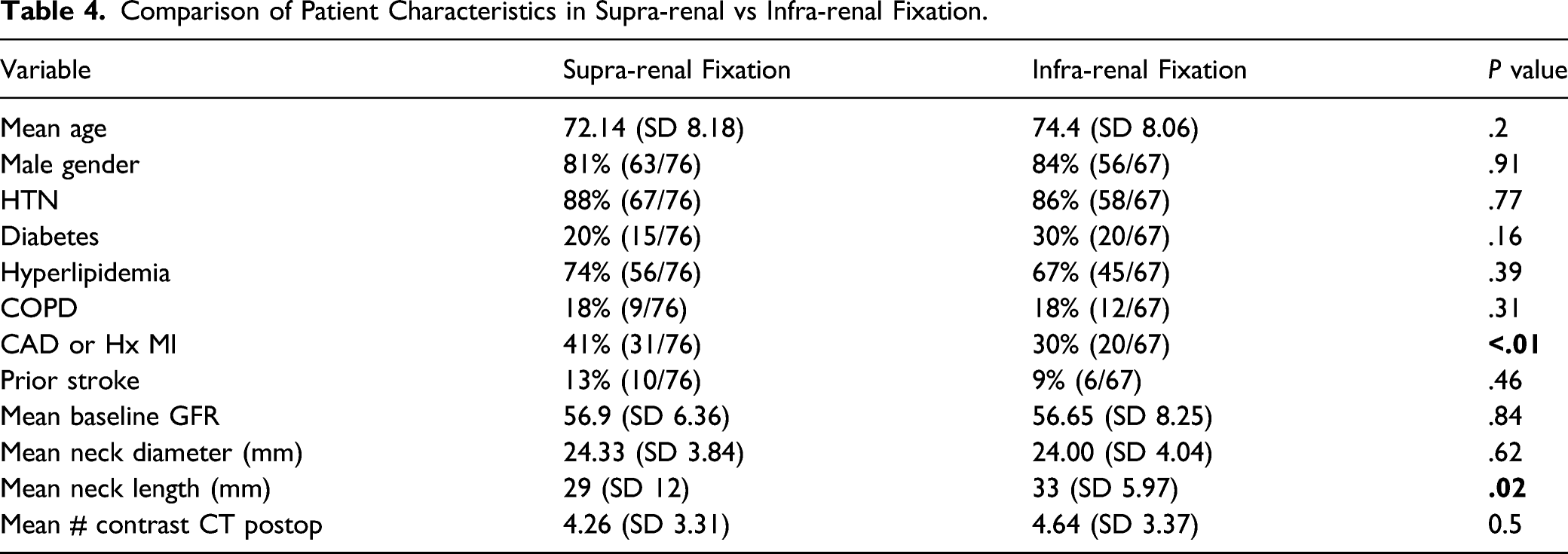
Comparison of Patient Characteristics in Supra-renal vs Infra-renal Fixation.
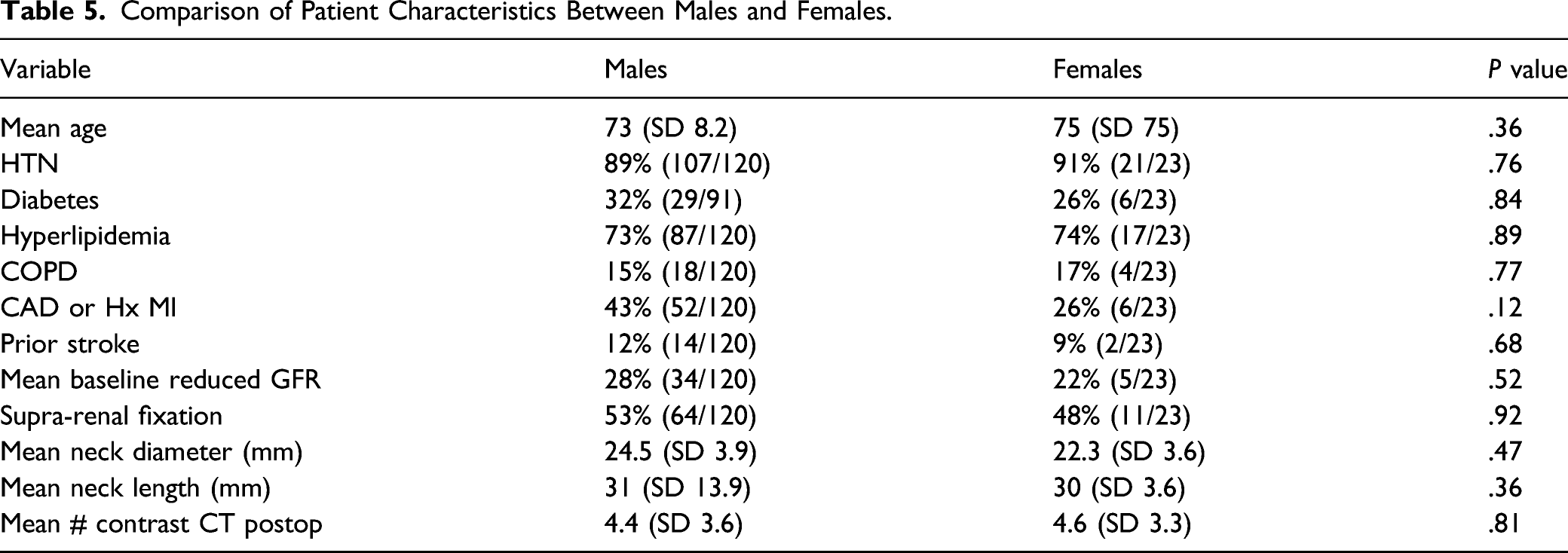
Comparison of Patient Characteristics Between Males and Females.
Only 2 of the 143 patients in this study progressed to ESRD at 5 years after EVAR. The first patient was a 79-year-old female with a baseline GFR of 46, past medical history of hypertension, and a device with supra-renal fixation. The second patient was an 82-year-old male with hypertension, a baseline GFR of 40, and an infra-renal fixation device.
Discussion
This is the first study which investigates gender, aneurysm neck features, and hypertension as predictors of renal function decline 5 years after EVAR. Prior studies of renal function 5 years after EVAR have been done strictly in comparison to open repair, limited to comparison of supra- and infra-renal fixation, or had intra-study multi-year variations between surgery and outcome.1-5 Analyzing long-term outcomes is critical to making informed treatment recommendations.
Female gender was the leading statistically significant multivariate predictor of long-term renal function decline in our single institution cohort (OR 3.9, P = .023). Five years after EVAR, we saw a greater than 20% drop in GFR in 39% of females relative to just 19% of males (OR 2.7, P = .035). Within the female patient group, 57% of those with supra-renal fixation developed renal decline as opposed to just 18% in those with infra-renal fixation (OR 3.2, P = .08).
Gender difference in vascular surgery outcomes is a well-recognized phenomenon. Prior studies in gender comparison for aortic aneurysm have focused primarily on either perioperative outcomes or long-term mortality, but not long-term renal function. Al Adas et al 3 investigated predictors of GFR drop of 30% or greater at any time frame after EVAR (from immediately postoperative to several years) and noted men to have a hazard ratio of .5 relative to women. This did not achieve statistical significance, as the relative paucity of women was a source of wide confidence interval. In a robust meta-analysis of gender differences in outcomes after EVAR, Liu et al 15 noted increased 30-day mortality (OR 1.6) and acute renal insufficiency (OR 1.73) in females. Several large multi-institutional investigations have identified increased perioperative mortality in females following EVAR, but this has not translated to increased long-term mortality.16-19
There are several potential explanations for increased rate of renal decline in females relative to males after EVAR, particularly with supra-renal fixation. Females present for AAA repair at a slightly advanced mean age relative to men.20,21 Less renal parenchyma volume creates a higher contrast to nephron ratio when postoperative CT angiograms are performed creating an increased theoretical risk of contrast nephropathy. Female patients on average have smaller caliber renal arteries which are more vulnerable to meaningful trauma from guidewires or supra-renal stent graft struts.
Supra-renal fixation was noted to have an odds ratio of 2.3 relative to infra-renal fixation for long-term GFR drop over 20%. This achieved univariate significance and approached multivariate significance. Renal infarcts, renal artery stenosis, and renal artery occlusion are all noted to occur following 2–5% of EVAR. These phenomena occur more than twice as frequently when devices with supra-renal fixation are utilized.6,8 Stent grafts with supra-renal fixation have been noted to cross 1 renal artery orifice in 40% of cases, both renal arteries in 9%, and neither renal artery orifice in 51% of sEVAR. 22 This has the potential to induce turbulent renal artery flow which may be disruptive or serve as an embolic nidus. The smaller the renal artery, the more significant the potential consequences may be. However, this has not been associated with an increased short- or mid-term rate of malignant hypertension or new onset dialysis requirement across all genders.3,6,8-12 However, long-term gender specific outcome investigation is lacking. This study adds to the literature by extending the timeline of renal function analysis after EVAR. The deleterious effect of supra-renal fixation in some patients did not manifest in malignant hypertension or dialysis requirement in our patients. Nevertheless, it does serve as warning that for patients with advanced renal insufficiency (GFR under 25, for example), there may be an increased risk of reaching ESRD with supra-renal fixation. More robust multicenter long-term investigation would be worthwhile.
Comparison of patient characteristics undergoing sEVAR vs iEVAR in our study was made (Table 4). We did not identify any meaningful selection bias between sEVAR and iEVAR in our analysis. sEVAR was performed in patients with shorter mean neck than iEVAR. However, the mean neck length for sEVAR was 29 mm which is well in excess of standard stent graft instructions for use recommendations. Further, neck length was not predictive of renal decline in univariate or multivariate analysis.
Baseline renal insufficiency was the second factor that reached multivariate statistical significance in predicting long-term renal function decline after EVAR in our study (OR 3.8, P = .001, multivariate P = .029). Patients with pre-existing renal dysfunction are more prone to long-term continued decline for several reasons. Foremost, the intrinsic pathology which induced renal insufficiency is still present (examples—HTN, DM, and atherosclerosis) and has the potential to continue to damage nephrons. Patients with renal insufficiency are significantly more vulnerable to iodinated contrast induced toxicity than patients with normal renal function.23,24 EVAR and CT angiogram surveillance both expose these patients to contrast. Indeed, the amount of contrast medium used during EVAR and the first year of surveillance has been associated with renal function decline 12 months after EVAR. 11 We did investigate the number of CT scans in the first postoperative 5 years as a potential predictor of renal decline but did not find an increased risk. In fact, the cohort with over 20% long-term GFR drop underwent fewer CT scans with contrast than those without drop in renal function. This is likely due to avoidance of CT scan in favor of duplex ultrasound in patients with abnormal renal function. Not having access to imaging records at outside hospitals also limits this analysis as patients may have had contrast exposures of which we are not aware.
Baseline hypertension showed a strong trend toward predicting long-term renal function decline (OR 9.4, univariate P = .001) but did not achieve multivariate significance (P = .17) despite having the highest multivariate odds ratio (5.0). Hypertension is a well-recognized source of chronic renal insufficiency and among the leading causes of ESRD.25,26 Of the patients who experienced a greater than 20% drop in GFR 5 years after EVAR, 97% had a pre-existing diagnosis of hypertension at the time of intervention. This creates a strong implication that the absence of hypertension is protective against long-term renal decline after EVAR.
Infra-renal neck diameter was a univariate predictor of long-term renal decline, but lacked multivariate significance. AAA diameter was not investigated as a predictor of decline in renal function in our study. As mentioned, neck diameter was included and larger neck diameters correlate with larger mean AAA diameters. Further, AAA diameter has been previously associated with accelerated long-term renal decline, likely secondary to more advanced co-morbidity and duration of tobacco use. 4
We did identify weaknesses in our study. Challenges of the retrospective chart review did not allow for thorough investigation of smoking status, secondary interventions, presence of accessory renal arteries, or the number of iodinated contrast CT scans at outside facilities as variables. While we did not find meaningful baseline patient characteristic differences between females and males or between sEVAR and iEVAR patients, any retrospective review of non-randomized patients has vulnerability to selection bias. Patients who progressed to ESRD but did not survive to 54 months were not included in our study. Therefore, if some of the deleterious effects of certain variables on renal function contributed to renal failure associated mortality, this was not identified. This is due to the initial study design being focused on the long-term effects of supra-renal fixation. Before 2016, our laboratory reported all GFR with a value of 60 or higher as 60 mL/min/1.73 m.2 If higher values of GFR were recorded, then more patients with a drop of 20% or greater may have been detected. Finally, the timing of laboratory analysis may affect GFR value and not reflect the baseline at which a patient is truly living. Factors such as dehydration at the time of testing may alter results and trigger a false positive. Congestive heart failure, a risk for declining renal function, was not included in our variables due to difficulty in obtaining echocardiogram information in our review. This would have been a prudent variable to include in analysis if consistent data had been readily accessible. Patients undergoing concomitant renal artery intervention were excluded from our study. The presence of renal artery stenosis on preoperative CT imaging was not included as a study variable, nor was the presence of accessory renal arteries. Finally, a significant number of patients were lost to follow-up.
Progression to ESRD is indeed rare after EVAR which further emphasizes the need for large database or multi-center investigation of the topic of 5 year and longer outcomes. Only 2 of the 143 patients in our study progressed to ESRD in the 5-year postoperative interval. A more robust study involving multiple institutions would be worthwhile to investigate for the same risk ratios for long-term renal decline after EVAR. If similar findings were achieved with a study number 5-10 times larger, then stronger clinical recommendations could be made. Given that over 80 percent of AAA interventions are performed on male patients, achieving powerful data on female AAA patients is challenging in single institution studies. Regarding the potential effect of our findings on clinical practice, female patients with baseline renal insufficiency are the most intriguing cohort. The potential benefit of avoidance of supra-renal fixation in female patients with baseline renal insufficiency is worth further investigation. Specifically, if larger studies confirmed a 58% rate of long-term renal function decline in females following sEVAR relative to 18% in females with iEVAR, then opting for iEVAR in females with GFR under 30 would be prudent.
Conclusions
Females and patients with baseline renal insufficiency are more vulnerable to significant decline in renal function 5 years following EVAR. Consistent with analogous literature, supra-renal fixation appears moderately deleterious toward renal function with no clinical significance in those with baseline normal renal function. The potential benefit of avoidance of supra-renal fixation in female patients with baseline renal insufficiency is worth further investigation in a more robust multi-center study.
Footnotes
Acknowledgment
We would like to thank James Sinacore, PhD, for his assistance with performance of multivariate regression analysis.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Carlos F. Bechara serves as a consultant to WL Gore Medical, Cook Medical, Endospan and holds equities in Mokita Medical.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Statement
Loyola University IRB approved this retrospective review of de-identified patient information. IRB reference – LU #214380.