
Abstract
Objective
After a nondenial prior authorization program evaluates orders for peripheral artery revascularization (PAR), ordering physicians sometimes withdraw their orders based upon program recommendations. Some patients with withdrawn orders receive PAR if claudication does not resolve. To characterize patient outcomes under this program, we evaluated whether associations existed between the withdrawal of patients’ initial PAR orders and the presence of claims for PAR and claims mentioning intermittent claudication (IC) in the following 16 weeks.
Methods
Orders for PAR placed from 1/1/19 to 9/30/19 for patients with Medicare Advantage health plans were extracted from a national healthcare organization’s database. Claims data from 0 to 16 weeks following the order were reviewed to determine if patients had downstream PAR claims, or if they had emergency department or hospital claims mentioning IC. Chi-square tests were used to assess the association between order withdrawal and downstream PAR, as well as claims mentioning IC. Multivariate logistic regressions were run to assess the same, controlling for patient age, sex, urbanicity, local median income, state obesity rate, type of PAR, ordering physician specialty, and whether PAR was ordered in a hospital setting.
Results
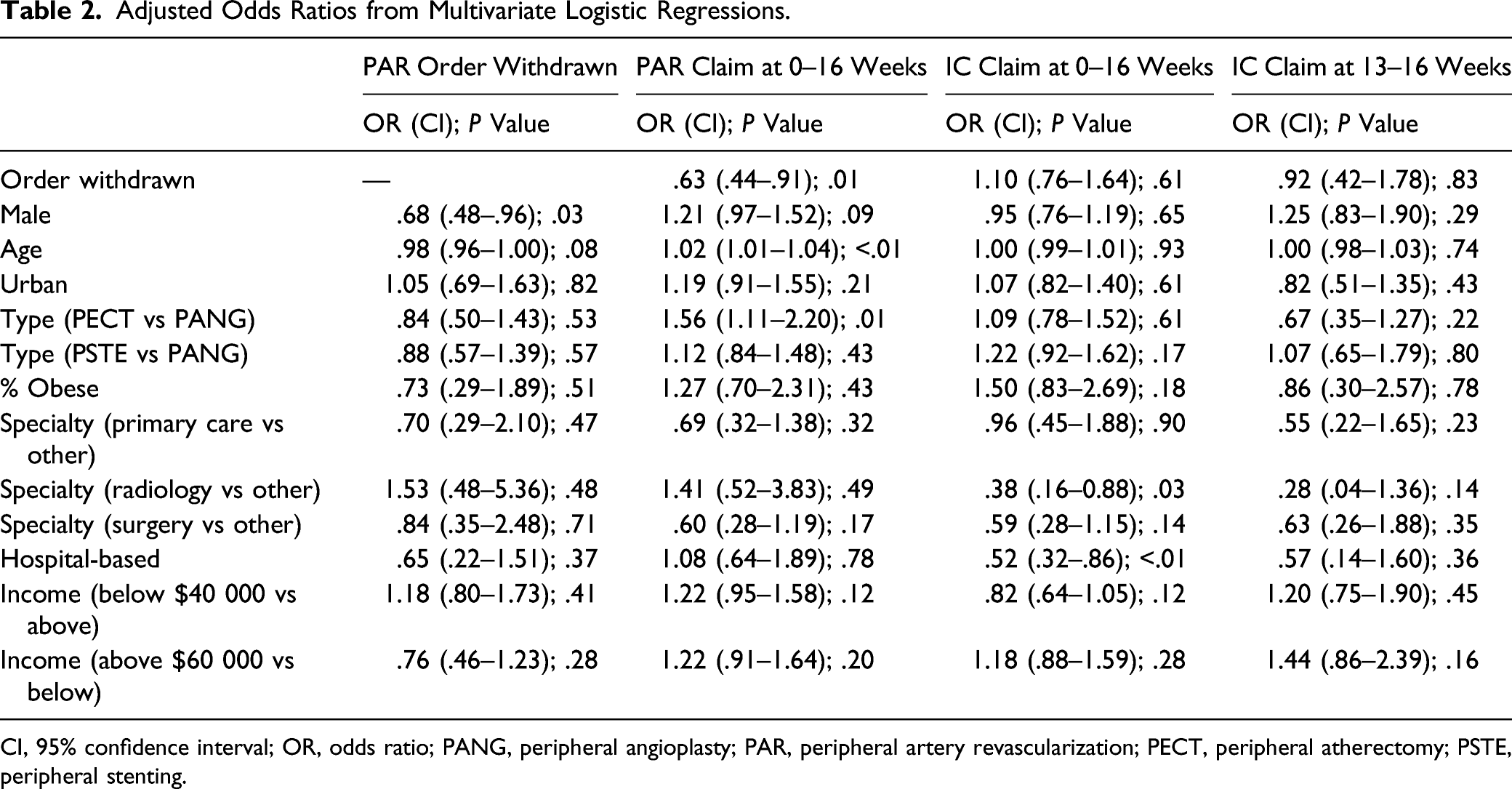
Of 1588 orders meeting inclusion criteria, 71.9% (1038/1444) of authorized orders and 61.1% (88/144) of withdrawn orders were followed by PAR within 16 weeks, a significant difference (P < .01). Relatedly, 69.8% (1008/1444) of authorized orders and 70.8% (102/144) of withdrawn orders were followed by IC claims, an insignificant difference. Multivariate logistic regressions showed patients with withdrawn PAR orders had significantly lower adjusted odds of PAR (OR: 0.63; 95% CI: 0.44–0.91), but an insignificant difference in their adjusted odds of IC (OR: 1.10; CI: 0.76–1.64).
Conclusions
Although patients with withdrawn PAR orders were significantly less likely to receive PAR in the subsequent 16 weeks, no association was found between withdrawn PAR orders and subsequent claims mentioning IC.
Keywords
Introduction
Peripheral artery disease (PAD) is common in older individuals and impacts more than 20% of people over the age of 80. 1 PAD can cause intermittent claudication (IC), which may limit patients’ physical activity and significantly reduce their quality of life.2,3 When patients experience intermittent claudication (IC), physicians may utilize surgical, medical, and exercise-based treatment to resolve the symptoms. Several studies have shown that exercise-first and revascularization-first approaches are similarly effective in improving the quality of life and functional performance of patients with PAD.4-6
As exercise and medical management are noninvasive, they are potentially beneficial initial approaches to managing IC that lack the potential for complications posed by surgery. Patients may engage in supervised exercise therapy in a hospital or outpatient setting, may pursue home-based exercise therapy with an observed component (e.g., a pedometer), or may be given walking advice and not observed. 7 While supervised exercise therapy programs have the potential to offer patients more support than other approaches to exercise-based treatment, some research shows they have lower rates of adherence than home-based programs due to the need to leave the home to participate. 8 Supervised exercise therapy programs last up to 12 weeks, and thus, a substantial time commitment is required. 9
Despite the potential benefits of exercise-based and medical management of PAD, and the decades of evidence supporting them, these approaches are underused.10,11 Healthcare organizations can impact the pathways patients follow in addressing PAD through prior authorization. The purpose of this analysis is to describe the outcomes that patients experience after having their order for PAR reviewed and potentially withdrawn through nondenial prior authorization. It seeks to characterize whether patients whose orders for PAR were withdrawn through nondenial prior authorization were significantly more likely to experience downstream IC than patients whose orders were authorized. In doing so, the analysis provides a snapshot of the outcomes experienced by patients.
While there has been prior research examining the effectiveness of nonsurgical first-line treatment approaches for resolving intermittent claudication, little is known about the outcomes experienced by patients pursuing nonsurgical treatment following the input of a nondenial prior authorization program. As patients receiving arterial vascular surgeries can have surgical site infections at rates reported to range from 0.9% to 22%, many patients may be able to avoid infection by forgoing surgery. 12 If nondenial prior authorization can encourage physicians to withdraw PAR orders when other approaches may be safely attempted, it may be possible to reduce PAR utilization without increasing patients’ experiences of downstream IC.
Description of the Nondenial Prior Authorization Program
The national healthcare organization that is the focus of this analysis requires physicians to obtain authorization to perform peripheral artery revascularization (PAR) and other procedures. Orders for PAR are reviewed by a nondenial prior authorization program that combines rule-based evaluation of clinical appropriateness with peer-to-peer discussion. During these peer-to-peer conversations, ordering physicians may discuss whether there are alternatives to immediately pursuing PAR, such as having the patient attempt to resolve claudication through exercise or medication. The discussions are educative in nature and do not directly lead to denials, even if there is disagreement between the ordering physician and peer physician. These phone-based discussions provide the ordering physician with the opportunity for the ordering physician to discuss the patient’s clinical presentation with a peer physician, to learn about the latest evidence, and to engage in a non-adversarial conversation about the best course of action for the patient. Based upon the information shared, the ordering physician may decide to withdraw their order for PAR. All orders that are not withdrawn are either authorized (sometimes with a change in the type of PAR that will be performed) or referred to the health plan for review. If the patient’s IC does not resolve with the initial nonsurgical approach, the physician may order PAR for the patient afterward.
Methods
Study Design
This retrospective, observational study consisted of a patient-level analysis of orders for PAR, as well as claims for PAR and claims for emergency department-based and hospital-based care. This study was reviewed by the Advarra institutional review board (Pro00046556) and received an exemption from oversight and waiver of informed consent on September 11, 2020, in accordance with the Department of Health and Human Services regulations found at 45 CFR 46.104(d)(4). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Data Source and Sample Population
Orders for PAR for patients aged 18 to 89 years, with Medicare Advantage health plans, placed between January 1st, 2019, and September 30th, 2019, were extracted from the database of a nondenial prior authorization company. Orders for PAR were for peripheral angioplasty, peripheral atherectomy, and peripheral stenting. The patients’ claims for PAR, emergency department-based care, and hospital-based care, filed between 0 and 16 weeks after each PAR order, were used for the study’s analysis. Health plan enrollment data pertaining to these patients for this period were obtained as well. Orders were excluded if they pertained to patients that were not continuously enrolled in their health plan for the 16 weeks following the order, with no claudication (as indicated on the order), with acute limb ischemia (as indicated on the order), if the order was not the patient’s first in the sample, if the patient had multiple PAR orders on the day, if the disposition of the order for PAR was unknown because it was referred to the organization sponsoring the health plan for review, if the patient had a PAR claim filed in the 16 weeks prior to the order, or if the patient did not have an angiography claim (Current Procedural Terminology code 36245, 36246, 36247, 75630, 75710, or 75716) between 16 weeks before the order and 16 weeks after the order. Only patients that had angiography shortly before or after their PAR order were included, as angiography is necessary to determine a patient’s candidacy for PAR.
The control variables in the analysis were the patient’s age, sex (as reported in administrative data), the type of PAR ordered, the ordering physician’s specialty, and whether the ordering site was a hospital. Additional control variables were constructed by mapping patients’ ZIP codes to publicly available data. The urbanicities of patients’ home ZIP codes were determined using a table developed by the Centers for Medicare & Medicaid Services. 13 The American Community Survey’s 1-year estimate of income in 2018 inflation-adjusted dollars was used to determine the median incomes of patients’ home ZIP codes. 14 Two binary variables were then constructed, denoting if the median income within each patient's home ZIP codes was below $40,000 or above $60,000 per year. Using 2019 data from the Behavioral Risk Factor Surveillance Survey, the prevalence of obesity in the patient’s home state was determined. 15
Measurement
The outcomes examined were whether the patient had a claim for PAR (defined as a claim with a Current Procedural Terminology code in the range 37224–37231) within 0–16 weeks of the initial order, whether the patient had an emergency department-based or hospital-based claim mentioning IC (defined as a claim with an International Classification of Diseases, version 10, code in the range I70.211–I70.219) within 0–16 weeks of the initial order, or whether the patient had an emergency department-based or hospital-based claim mentioning IC within 13–16 weeks of the initial order. The period 13–16 weeks after the initial order was examined, as prior research has established that 12-week exercise training programs can be beneficial to patients with symptomatic PAD. Thus, this period captures outcomes for patients a month after they have potentially completed a full course of exercise.8,16
Analysis
Descriptive statistics were calculated for each of the variables. Statistics for orders that were authorized were compared with statistics for orders that were withdrawn, and the significance of the differences in the statistics for the 2 types of orders was evaluated. Chi-square tests were used when proportions were compared, and t-tests were used when magnitudes were compared. Chi-square tests were then used to assess the presence of a univariate association between order withdrawal and 3 outcomes: PAR claims at 0–16 weeks, claims mentioning IC at 0–16 weeks, and claims mentioning IC at 13–16 weeks. An adjusted analysis using multivariate logistic regression was used to assess whether there was an association between each of the control variables and if the initial PAR order was withdrawn. Multivariate logistic regression was also used to assess whether there was an association between the withdrawal of the initial PAR order and PAR claims at 0–16 weeks, claims mentioning IC at 0–16 weeks, and claims mentioning IC at 13–16 weeks, after adjusting for the control variables. Results from the multivariate logistic regressions were reported as odds ratios (OR) with 95% confidence intervals (CI).
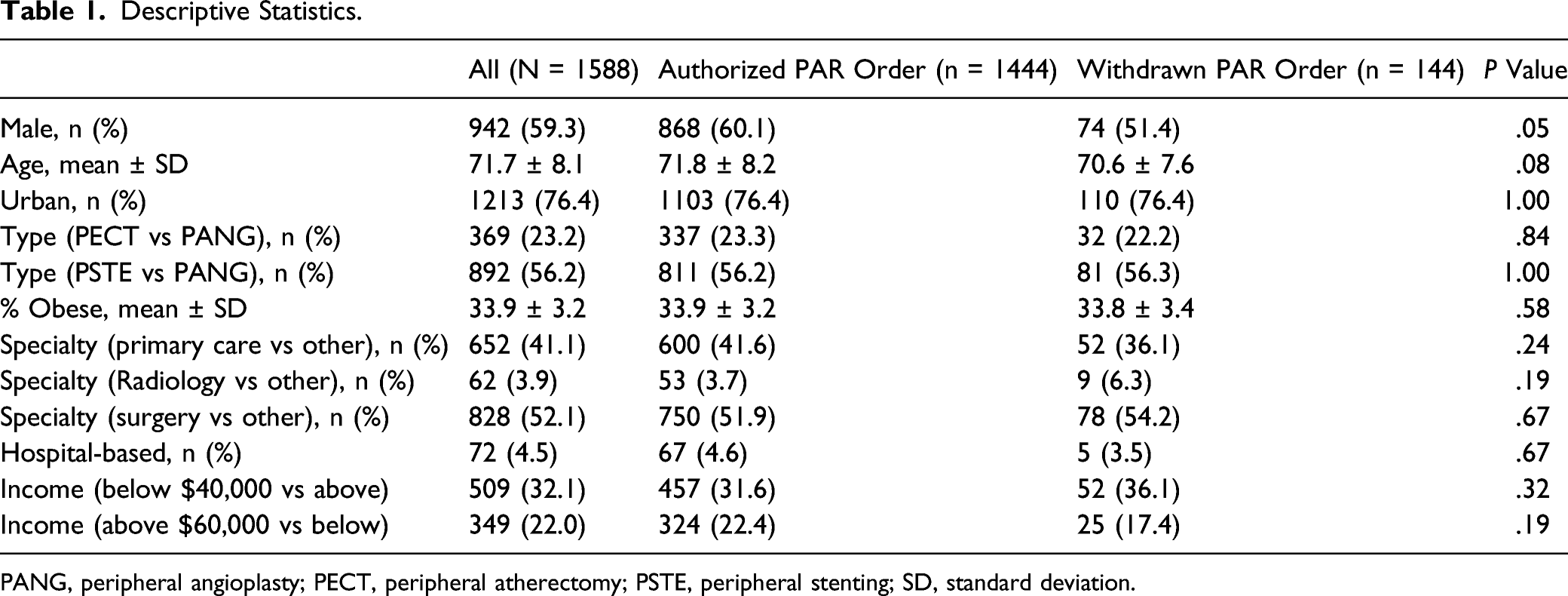
Results
Of the 10389 orders meeting the initial inclusion criteria, 1588 remained after exclusion criteria were applied (Figure 1). The primary reason orders were excluded was that they pertained to patients with acute limb ischemia (n = 3970). These patients were excluded as they were not good candidates for nonsurgical treatment. There were no statistically significant differences between the descriptive statistics of the orders that were authorized vs those that were withdrawn (Table 1). The difference in the percentage of the patients included in the groups that were male differed slightly, but not enough to meet the criteria for significance (P = .052). Overall, 59.3% of the patients included in the study were male and had a mean age of 71.7 years. Most (76.4%) lived in urban areas. Most orders (56.2%) were for peripheral stenting, the second largest percentage were for peripheral atherectomy (23.2%), and the remainder were for peripheral angioplasty. Obesity was common in patients’ home states, with a mean rate of 33.9%. Most orders were placed by a physician with a surgical specialty (52.1%), although orders from primary care physicians were also common (41.1%). A minority of orders (4.5%) pertained to care in a hospital-based setting. Participant Selection Diagram. Descriptive Statistics. PANG, peripheral angioplasty; PECT, peripheral atherectomy; PSTE, peripheral stenting; SD, standard deviation.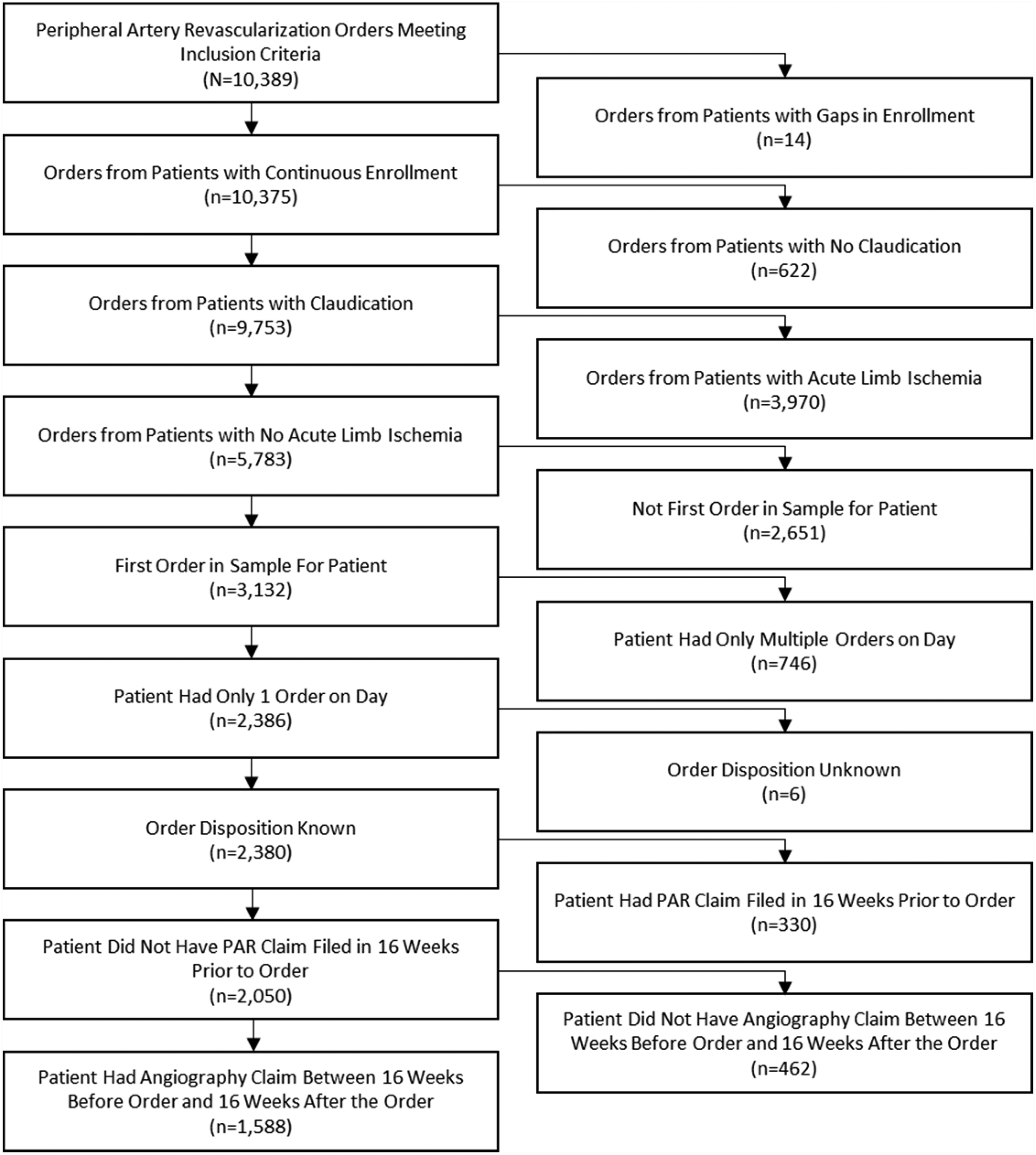
Within the set of orders meeting selection criteria, 71.9% (1038/1444) of authorized orders and 61.1% (88/144) of withdrawn orders were followed by PAR within 16 weeks, a significant difference (P < .01). There was an insignificant difference (P = .87) in the rate at which initial authorized vs withdrawn PAR orders were followed by IC claims at 0 to 16 weeks; 69.8% (1008/1444) of authorized orders and 70.8% (102/144) of withdrawn orders. There was likewise an insignificant difference (P = .92) in the rate at which initial authorized vs withdrawn PAR orders were followed by IC claims at 13–16 weeks; 6.9% (99/1444) of authorized orders and 6.3% (9/144) of withdrawn orders.
Adjusted Odds Ratios from Multivariate Logistic Regressions.
CI, 95% confidence interval; OR, odds ratio; PANG, peripheral angioplasty; PAR, peripheral artery revascularization; PECT, peripheral atherectomy; PSTE, peripheral stenting.
Discussion
This study characterized the outcomes produced by a nondenial prior authorization program that in some cases, encouraged orders for PAR to be withdrawn. Even though some patients had their orders reinitiated, patients whose orders were withdrawn were still significantly less likely to have a PAR procedure performed within 16 weeks. There was no association between whether patients had their orders approved and whether they experienced IC, either during the 16-week period following their order, or at 13–16 weeks following their order—when they could have potentially completed an exercise regimen.
The findings of this study suggest that only the sex of the patient was significantly associated with whether an order for PAR was authorized or withdrawn during the nondenial prior authorization process. The adjusted model (Table 2) found that male patients were significantly less likely to have their PAR order withdrawn. None of the other factors examined were associated with withdrawal. Although age and type of revascularization ordered were not significantly associated with order withdrawal, this finding suggests that potentially there were physiological differences between patients with authorized vs withdrawn orders. As the criteria used by the nondenial prior authorization program for evaluating the appropriateness of PAR does not consider the patient’s sex, this finding is not a direct byproduct of the program’s ruleset.
Withdrawn PAR orders were significantly associated with reduced adjusted odds of a PAR claim within 0–16 weeks of the order. While 61.1% of patients with a withdrawn PAR order did ultimately receive a PAR procedure, this was a significantly lower frequency than was observed among patients whose PAR orders were authorized. Order reinitiation after withdrawal in the context of prior authorization has been previously reported, and varies in its extent, depending upon the nature of the procedure ordered.17,18
It was anticipated that some orders for PAR would be reinitiated, as not all patients would be able to resolve their claudication through exercise or medical management. Furthermore, all the patients with withdrawn orders had been previously deemed by their ordering physicians to need PAR. Thus, the patients in this population were likely in greater need of PAR than the general population of patients with PAD.
Order withdrawal was not significantly associated with increased odds of IC at 0–16 weeks or 13–16 weeks. The main consequence for patients with a withdrawn order but subsequent IC was likely delayed surgery due to the attempt at resolving the claudication through nonsurgical means, an approach endorsed by experts in both the United Kingdom and the United States. For instance, the peripheral arterial disease guideline of the United Kingdom–based National Institute for Health and Care Excellence recommends that all patients with IC be offered a supervised exercise program. 19 Meanwhile, the British Association of Sport and Exercise Sciences Expert Statement on Exercise Training for People with Intermittent Claudication due to Peripheral Arterial Disease states that “revascularisation or drug treatment options should only be considered if exercise training provides insufficient symptomatic relief.” 20 Finally, the 2016 American Heart Association/American College of Cardiology Guideline on the Management of Patients with Lower Extremity Peripheral Artery Disease likewise states that structured exercise therapy “is an important element of care for the patient with PAD.” 21 Thus, while some patients may experience delayed PAR because of a nonsurgical attempt to resolve PAD, this delay is consistent with professional guidelines.
Professional societies endorse attempting to resolve PAD without PAR, as there are several quality benefits to doing so. Since patients can develop infections during surgery, reducing PAR utilization prevents some of these infections from occurring. 12 Furthermore, patients now face the potential for exposure to COVID-19 while in a clinical setting. Thus, reducing PAR utilization decreases the extent to which patients experience these negative outcomes.
Although the mechanisms by which patients with withdrawn orders resolved their IC were not examined, our findings suggest the means used by the patients with withdrawn orders and authorized orders may have had similar efficacy over the period examined. While some patients may have experienced delays in surgery because of the program, delaying surgery to pursue nonsurgical management is congruent with international guidelines.
Limitations
Since only data present in orders and claims were reviewed, there may have been unobserved clinical factors which could have influenced the outcomes of this study. Nonetheless, important issues related to the patients’ clinical presentations were documented during the ordering process. For instance, the orders noted whether patients had claudication and acute limb ischemia. While the orders for PAR that were authorized vs withdrawn differed on none of the patient and provider characteristics examined, other than sex, it is possible that the patients with withdrawn PAR orders were at lower risk for downstream IC at the time their orders for PAR were placed.
Patients whose orders were withdrawn by their physician so that exercise could be pursued may have been given walking advice, a home-based exercise program, formal supervised exercise therapy, or medical management. Given that the first 2 options do not produce claims data, the claims data available do not provide a clear picture of how patients attempted to nonsurgically resolve their IC. Since the extent to which patients exercised cannot be measured, it is not possible to determine whether their efforts to exercise were correlated with whether they ultimately had a PAR. Likewise, due to the nature of the data used, it was not possible to examine outcomes traditionally used in the study of PAD treatment, such as maximum walking distance, pain-free walking distance, or quality of life. 22
Additionally, the possibility exists that patients with withdrawn orders could have experienced lower rates of downstream IC during the 16-week period if their orders for PAR had been approved. Nonetheless, the UK and US guidelines on the management of PAD recommend attempting nonsurgical interventions and suggest that the benefits of avoiding surgery outweigh the potential downside of delayed surgery. In characterizing the rate of downstream IC, the study reassuringly does not find any evidence that patients with withdrawn orders experience IC at significantly higher rates.
The failure to find an association between prior authorization outcomes and downstream IC does not guarantee that an association does not exist. While the difference in the rate at which initially authorized vs withdrawn orders were followed by downstream IC was insignificant (P=0.87), patients with authorized orders had slightly lower downstream rates of IC. The study lacked the statistical power to yield a significant finding for the small effect size observed. Thus, it is possible that a study with a larger sample could have found a significant association between prior authorization outcomes and downstream IC if the effects observed were maintained as the sample size were increased.
Finally, the data analyzed pertained to patients with health plans from 1 national organization. Patients with non-Medicare Advantage health plans were not included in the analysis, and thus, the findings may not be generalizable to patients with commercial health plans. As the patients resided predominantly in the South, our findings may not be representative of the overall US population.
Conclusion
In a population of patients with Medicare Advantage health plans receiving orders for PAR in 2019, patients whose orders were authorized were no less likely to experience downstream IC than those patients whose orders were withdrawn. When patients’ initial orders for PAR were withdrawn rather than authorized by nondenial prior authorization, the patients were significantly less likely to receive PAR within the following 16 weeks, but had similar rates of IC both during the 16-week period and in the final 4 weeks of it. While many patients whose initial orders were withdrawn ultimately had PAR within the 16-week period, some were able to avoid it. This suggests that there may be a quality benefit to encouraging patients to manage their claudication via nonsurgical means before pursuing surgery. Nondenial prior authorization is one means of promoting the deferral of PAR.
Footnotes
Declaration of Conflicting Interests
AP, CL, CD, and AD report an employment or consulting relationship with HealthHelp/WNS at the time the study was written. EL, JL, and JS report employment by Humana Inc. AP additionally reports employment by Payer+Provider Syndicate and stock ownership of Amazon, Berkshire Hathaway, JPMorgan Chase, Payer+Provider Syndicate, Target, and Walmart.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: Funding for the development of this manuscript was provided by HealthHelp and Humana Inc., in the form of general compensation provided to the authors. The authors were compensated for participation in research activities as a part of their job responsibilities, rather than this particular study.
Authors’ Note
An abstract based upon this study has been presented at the 2021 New Cardiovascular Horizons Annual Conference.