
Abstract
The development of aneurysms of thoracoabdominal aorta (TAAA) in a post-transplant patient is a rare clinical situation and requires special attention. Endovascular treatment is the most suitable option for these patients due to numerous comorbidities. Particular emphasis should be placed on the ejection fraction as one of the main criteria for qualifying for surgery. The treatment itself remains a major challenge relating to anatomical constrains; however, it is possible in select patients in experienced centers.
Keywords
Introduction
The increase in the number of heart transplantation (HT) procedures, as well as aging patient population undergoing transplant, has contributed to the increased incidence of aortic aneurysms in transplant recipients. 1 Treating complex aneurysms in a patient after HT is a therapeutic challenge despite advancement of aortic aneurysm surgery techniques in the last few decades.2,3 In this paper, we present a case of a symptomatic aneurysm of the thoracoabdominal aorta (TAAA)
Consent was obtained from the patient to publish these images and clinical history.
Case Report
A 65-year-old man presented to the emergency department (ED) with a sudden increase in abdominal pain which had been present for the past 2 weeks. Due to ischemic heart disease and post-infarction cardiomyopathy, the patient had undergone HT surgery 19 years before, followed by multiple percutaneous coronary interventions of the left circumflex artery 13 years later and of the anterior descending artery 15 and 18 years later. Additionally, the patient had a history of diabetes mellitus, chronic renal failure stage 4, hypertension, hyperlipidemia, and he was a long-time smoker. Upon admission to the ED, the patient was hemodynamically stable and had a Glasgow coma score of 15. Special attention was paid to cardiac function indices with the left ventricular ejection fraction (LVEF) of 65% confirmed by echocardiography (ECHO) and recent signs of myocardial infarction excluded by electrocardiogram (ECG). An urgent computed tomography angiography (CTA) examination of the aorta showed a TAAA measuring 62 x 64 mm, type IV Crawford Classification (Figure 1), below the origin of the superior mesenteric artery (SMA) and another aneurysm at the level of the renal arteries measuring 36 mm in diameter. (Figures 2A–C) In comparison to the previous CTA scan, the newest revealed a 20-mm growth of the abdominal aorta in the past 14 months. A decision was made to treat this patient with a two-stage endovascular repair. The first surgery was conducted 13 days after hospital admission due to the fact that the patient required a multispecialist approach, including cardiovascular and cardiosurgical specialists, a transplant physician, and a renal specialist consultation. The first stage of the branched endovascular aortic repair (BEVAR) involved placement of the proximal part of the “off-the-shelf” Zenith t-Branch Cook polyester stent-graft into the descending aorta with branches expanded into the visceral arteries (Figure 3). This was done via the right common femoral artery (RCFA) through percutaneous access. The distal bifurcated part of the stent-graft was introduced via the same access, with the right iliac limb landed in the right common iliac artery (RCIA) to achieve limb extension and with the left branch open in the aortic lumen. This approach allowed temporary aneurysm sac perfusion (TASP) to prevent spinal cord ischemia.
4
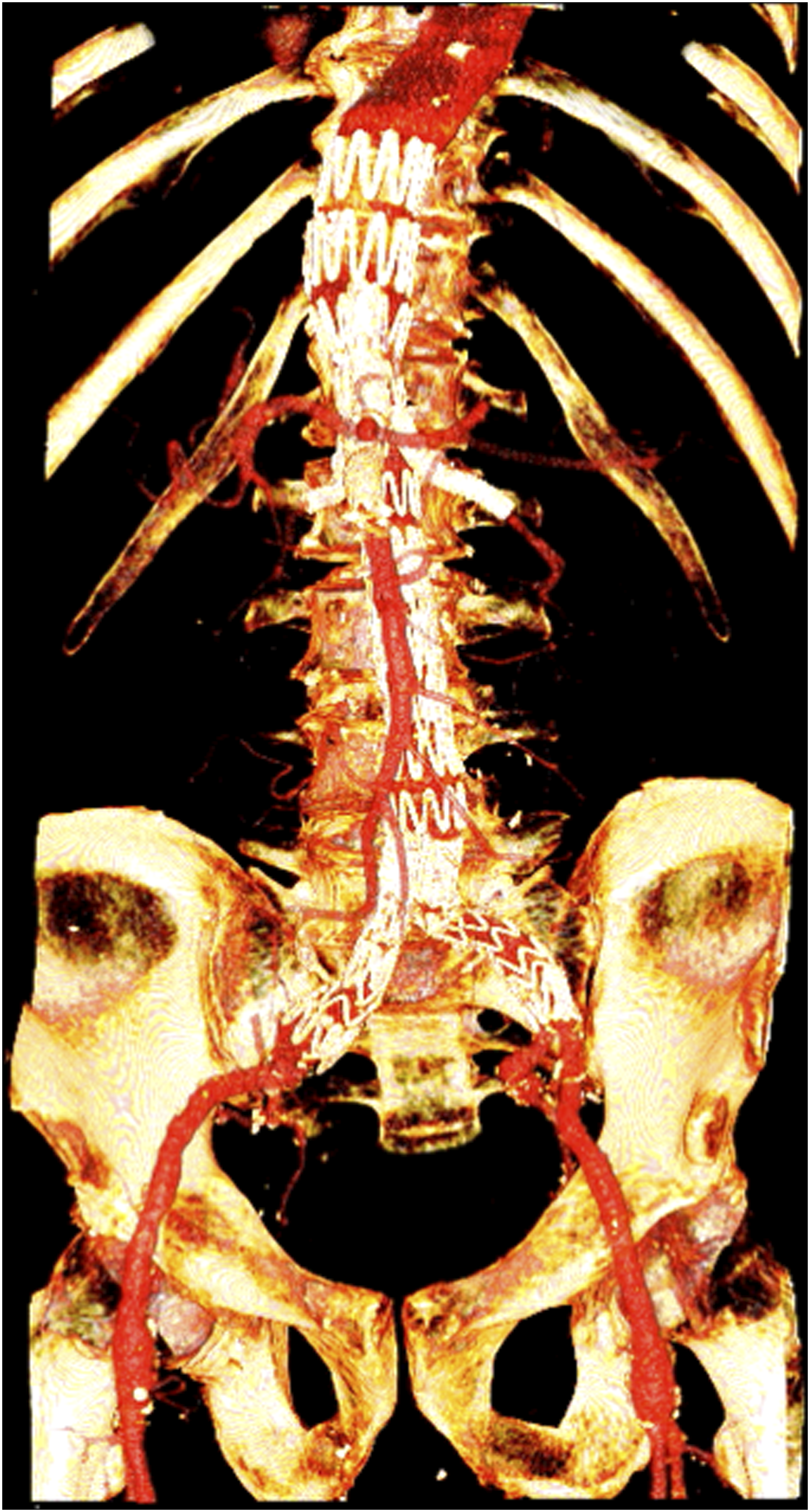
During this procedure, additional covered stent-grafts were also introduced into the right renal artery (RRA) and left renal artery (LRA), the SMA, and the visceral trunk via the left axillary artery (LAA). A post-procedure angiogram was successful, and the patient was discharged on the fifth day after the operation in good general condition, without complications. The second stage was carried out 42 days later and consisted of the introduction of the Zenith Cook stent-graft to the left common iliac artery (LCIA), thus completing the BEVAR procedure (Figure 4). Standard thoracic endovascular aortic repair (TEVAR) deployment approach was used. This involved placing a 12F arterial port into the left subclavian artery (LSA) and additional ports in the left common femoral artery (LCFA) and RCFA. Via the LCFA, a pigtail catheter was introduced into the aorta. The main part of the graft was implanted through the RCFA and advanced over the wire. The stent was expanded by inflating a balloon on the level of renal arteries. Additional stents were introduced via the LSA port into the visceral arteries. An intra-operative digital subtraction angiography (DSA) scan showed no leakage. The patient was discharged on the second day after surgery without complication. Preoperative CTA with volume-rendering reconstructions. Enlarged lumen of the contrast flow and the course of the aortic branches. CTA images of the thoracoabdominal aorta aneurysm prior to surgery. (A) Axial section, (B) sagittal section, and (C) coronal section. Perioperative digital subtraction angiogram of the aorta. The main element of the branched stent-graft was introduced by RCFA. It was expanded in the aorta. Ending with the right branch in RCIA, the left branch remained open in the aortic lumen for temporary influx into the lumbar arteries. Postoperative CTA with volume-rendering reconstructions.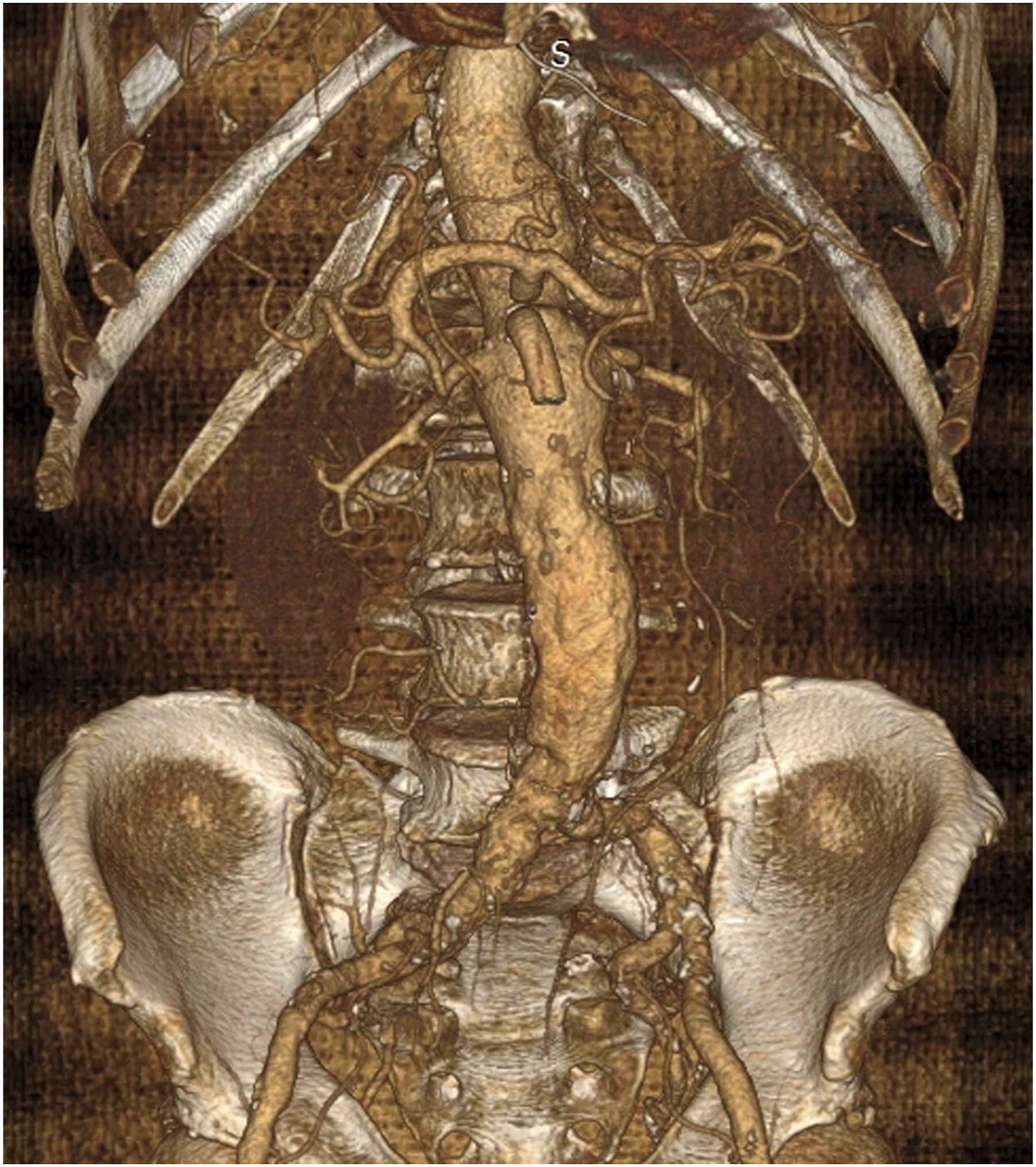


Follow-up CTA 5 months later revealed a small endo-leak at the level and below the RRA stent. This was treated with an additional covered stent-graft to the RRA with percutaneous access via the LAA with a good hemodynamic result. Computed tomography angiography performed 6 months later demonstrated no endo-leaks. On follow-up 19 months after the procedure, the patient remained well; daily activity did not cause shortness of breath, pain, or palpitations; and there were no postoperative complications. Echocardiography showed normal LVEF of 66%. During the ultrasound examination, no endo-leaks were detected. During the follow-up period, the patient underwent a transient ischemic attack 7 months post-surgery and he had an operation of an inguinal hernia, after which he returned to baseline level of fitness.
Discussion
Thoracoabdominal aorta is more common in ischemic-indicated HT recipients and is by far the most prevalent in male patients. 5 Review of the literature has found only 5 cases localized in the TAAA in patients after HT. Of the reported cases, only one has been operated with success; 3 patients died from rupture and 1 did not require surgery.5,6 The incidence of aortic aneurysms in heart transplant patients ranges from 1% to 6.2% depending on the examination. 5 The prevalence of aortic aneurysms in males over 65 is estimated at 4–7%. 7 There are numerous reports linking HT with an accelerated rate of aortic expansion and ultimately an increased risk of abdominal and thoracic aortic aneurysms at a younger age compared to the general population.8,9 Some authors attribute this phenomenon to a sudden change in hemodynamic conditions resulting from an increase in the LVEF and to different anatomical conditions of the aortic outlet of the left ventricle.1,8 The difference in diameter between the donor’s aorta and the recipient’s aorta, as well as the different elastic properties of these tissues, additionally stresses the vessel wall due to an abnormally high pulse load.5,6 Risk of an unfavorable prognosis at the time of aneurysm rupture and a greater number of urgent surgical interventions was increased in patients after HT.5,6,8 At the same time, the advantage of earlier surgery of small, asymptomatic abdominal aortic aneurysms (40–55 mm) over a conservative strategy, including regular monitoring of the size of the aneurysm by imaging methods, was not demonstrated.10,11,12 Guidelines for small, asymptomatic abdominal aortic aneurysms in post-HT patients remain limited and require further investigation. 10 Immunosuppression and previous history of HT were not described as risk factors of rapid AAA growth. Guidelines did not recommend any modifications in elective AAA treatment strategies and in the frequency of surveillance scanning in post-HT patients. 13
Transplant patients often develop new or worsening hypertension, which is seen as a side effect of immunosuppressive therapy.1,14 Other complications of immunosuppressants include blood sugar management disorders (including diabetes), hyperlipidemia, and the intensified atherosclerotic processes, all of which were observed in our patient. The role of immunosupressive treatment on atherosclerosis remains unclear and requires further evaluation. The use of immunosuppressive drugs seems to be a significant risk factor for the development of abdominal aortic aneurysms as it was documented in the population of patients after kidney or liver transplantation. 1 The formation of aortic aneurysms due to the effect of glucocorticoids has been proven in animal models and in patients with COPD treated with corticosteroids.14,15 Additionally, there is a growing body of evidence to suggest that immunosuppression contributes to an increase in the rate of graft infections. 13 Despite that, due to insufficient evidence, reduction of the dose of immunosuppressants to slow the widening of the aortic aneurysm is not recommended. 1
Due to the fact that this was a high-risk patient, a two-stage endovascular procedure with TASP was chosen. Leaving the left branch of the graph open allowed for a temporary inflow of blood to the iliac arteries. 16 Due to the presence of the aneurysm in the right internal iliac artery, the second stage was delayed (> 4 weeks) and was completed after 42 days. Such an approach was chosen due to reports showing that early reinterventions (< 4 weeks) are associated with the risk of complications in the form of renal and hepatic perfusion disorders. 4 The time span between stages was elongated due to cardiological, cardiosurgical consultations along with the transplant physician assessment, which were necessary in the process of qualifying the patient for the second stage of the surgery. Preserved LVEF in this patient was a key qualifier for the procedure. Follow-up ECHO at 8 and 15 months post-procedure demonstrated this to be maintained; thus, it can be concluded that the procedure did not adversely affect the patient’s cardiac function. Based on our experience, post-procedure follow-up should involve CTA at 1, 6, and 12 months, and every year thereafter. 12
Cardiological long-term management should be aimed at maintaining the fraction. This includes optimizing prevention and treatment against cardiac rejection, preventing complications and prophylaxis (diet and lifestyle). Optimal immunosuppression treatment is of paramount importance. The combination therapy with the lowest effective dose should be used in order to minimize the risk of side effects. Hypertension, diabetes, and dyslipidemia are quite common in these patients. Aggressive therapy for each of them is recommended. Heart transplant recipients are at high risk of developing severe flu and pneumonia. 17 They should be vaccinated against influenza and pneumonia. There are also no contraindications against SARS-CoV-2 vaccines. 18 Non-pharmacological management should include abstinence from tobacco, minimal alcohol intake and avoiding close contact with people with respiratory tract infections. Regular physical activity of at least 150 minutes a week of moderate-intensity exercise. 17
Conclusions
Based on the postoperative results and the control carried out 19 months after the procedure, we conclude that the two-stage endovascular procedure with TASP may be a useful therapeutic option for selected HT recipients. The endovascular option in these patients will contribute to extending life expectancy while avoiding major comorbidities associated with open repair.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.