
Abstract
Background
Recent studies report a limited window in which carotid endarterectomy (CEA) provides the greatest benefit for symptomatic carotid stenosis. Given the time-sensitive nature of CEA for symptomatic stenosis, it is important to understand whether patient outcomes are adversely affected by undergoing CEA over the weekend. Currently, it is unclear whether CEA is impacted by the “weekend effect” phenomenon.
Introduction
Three landmark studies have independently demonstrated that carotid endarterectomy (CEA) dramatically reduces the recurrent stroke risk in symptomatic patients with moderate-to-severe carotid stenosis.1-3 In the North American Symptomatic Carotid Endarterectomy Trial study, CEA significantly reduced 5-year risk of stroke or death in symptomatic patients with carotid stenosis (> 50%). 3 The European Carotid Surgery Trial mirrored this finding, with reduced 3-year risk of stroke or death in symptomatic patients undergoing CEA for carotid stenosis (> 80%). 2 These prospective trials have since been validated in a number of other studies. While recent advances in medical therapy may have lowered stroke risk in patients with symptomatic carotid stenosis, 4 the Society of Vascular Surgery (SVS) clinical practice guidelines still recommend CEA for symptomatic patients with carotid stenosis (5099%) as first-line treatment. 5
Interestingly, patients who suffer an ischemic neurologic event secondary to symptomatic carotid stenosis have a limited window in which they obtain the greatest benefit from CEA.6,7 Rothwell et al. 6 found that the benefit from surgery was greatest within 2 weeks after the ischemic event, with a significant decrease afterwards. Avgerinos et al. 8 found that CEA performed within 2 to 5 days after a neurologic event did not increase postoperative complications. More recently, Tanious et al. 7 reported an increased periprocedural risk within 48 h of an index stroke event.
Given the time-sensitive nature of CEA for symptomatic stenosis, it is important to understand whether patient outcomes are adversely affected by undergoing CEA over the weekend. The “weekend effect” has been previously described in other vascular diseases and procedures, with higher weekend mortality rates reported in ruptured aortic aneurysms,9,10 aortic dissection, 9 and lower extremity revascularization procedures. 11 Currently, it is unclear whether CEA is similarly impacted by the “weekend effect” phenomenon. In the present study, we investigated the “weekend effect” in CEA for symptomatic carotid stenosis. These results would help inform whether surgical revascularization should or should not be withheld on account of a weekend procedure.
Methods
The Research Patient Data Registry (RPDR) was retrospectively queried for all patients with symptomatic carotid stenosis who underwent CEA, from multiple institutions in the Mass General Brigham hospital system. International Classification of Diseases, ninth edition (ICD-9) codes were used to identify diagnosis and procedures. A total of 288 patients with symptomatic carotid stenosis underwent CEA during the study period from 2015 to 2020. The median follow-up period was 3 years.
Patients were divided into 2 cohorts based on day of surgery. The weekday group included CEAs performed on Monday to Friday, and the weekend group included CEAs performed on Saturday and Sunday. There was no overlap between groups. Specifically, no patients had a procedure that extended from Friday into Saturday or Sunday into Monday. No patients required bilateral CEA procedures for symptomatic carotid stenosis during the study period.
The RPDR was queried for patient demographic information, including age (years), race/ethnic group, gender, and medical comorbidities. Electronic medical records were reviewed to obtain information on perioperative data, including operating room (OR) time and estimated blood loss (EBL). Operative reports were reviewed for intraoperative complications and to verify EBL. Hospital discharge summaries were reviewed for details of hospital stay, including hospital length of stay (LOS), perioperative complications, and discharge destination. Death summaries (where applicable) and other medical records were reviewed for 30-day mortality rates. Discharge destinations included discharge home (with or without visiting nurse services), inpatient rehabilitation, or hospice/death. Perioperative complications included neck hematoma, wound infection, postoperative myocardial infarction (MI), cerebrovascular accident (CVA), cerebral hyperperfusion syndrome (CHS), and cranial nerve injury (CNI).
Primary outcomes were postoperative stroke and 30-day mortality rates. Secondary outcomes included non-stroke/death complications and indicators of increased hospital resource utilization, including OR time and hospital LOS. Categorical variables are described as integers (n) and percentages (%). Continuous variables are described as median and interquartile ratio (IQR). Univariate analysis was used to compare weekday and weekend groups. Multivariate logistic regression analysis was used to determine risk factors for postoperative stroke and 30-day mortality after CEA. Statistical analyses were performed utilizing MedCalc version 19.6 (MedCalc Software Limited, Mariakerke, Belgium). P-values of less than .05 were considered statistically significant. This study was approved by the Mass General Brigham Institutional Review Board (IRB #2020P003168).
Results
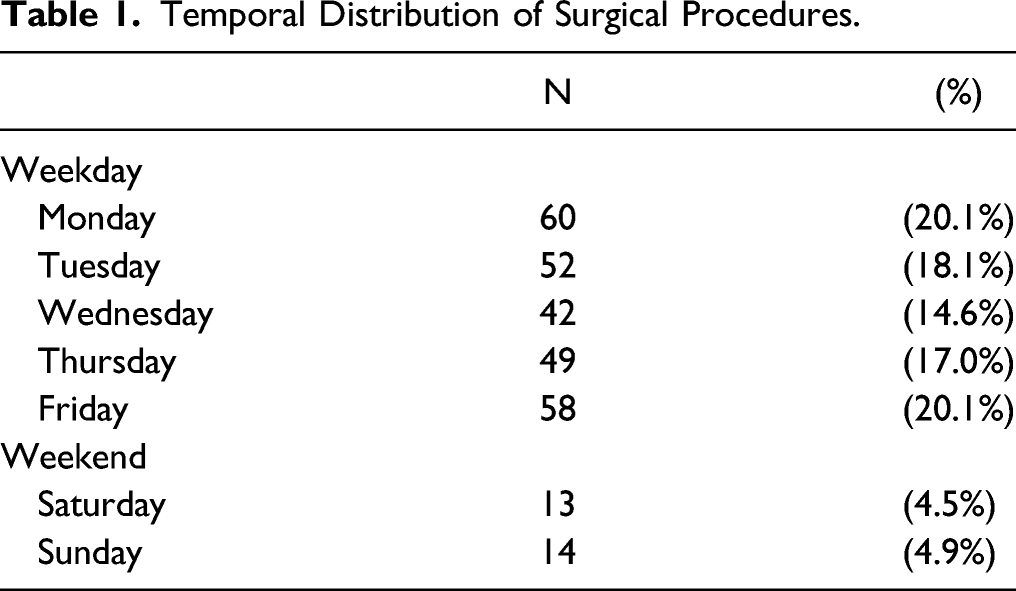
Temporal Distribution of Surgical Procedures.
Patient Demographics.
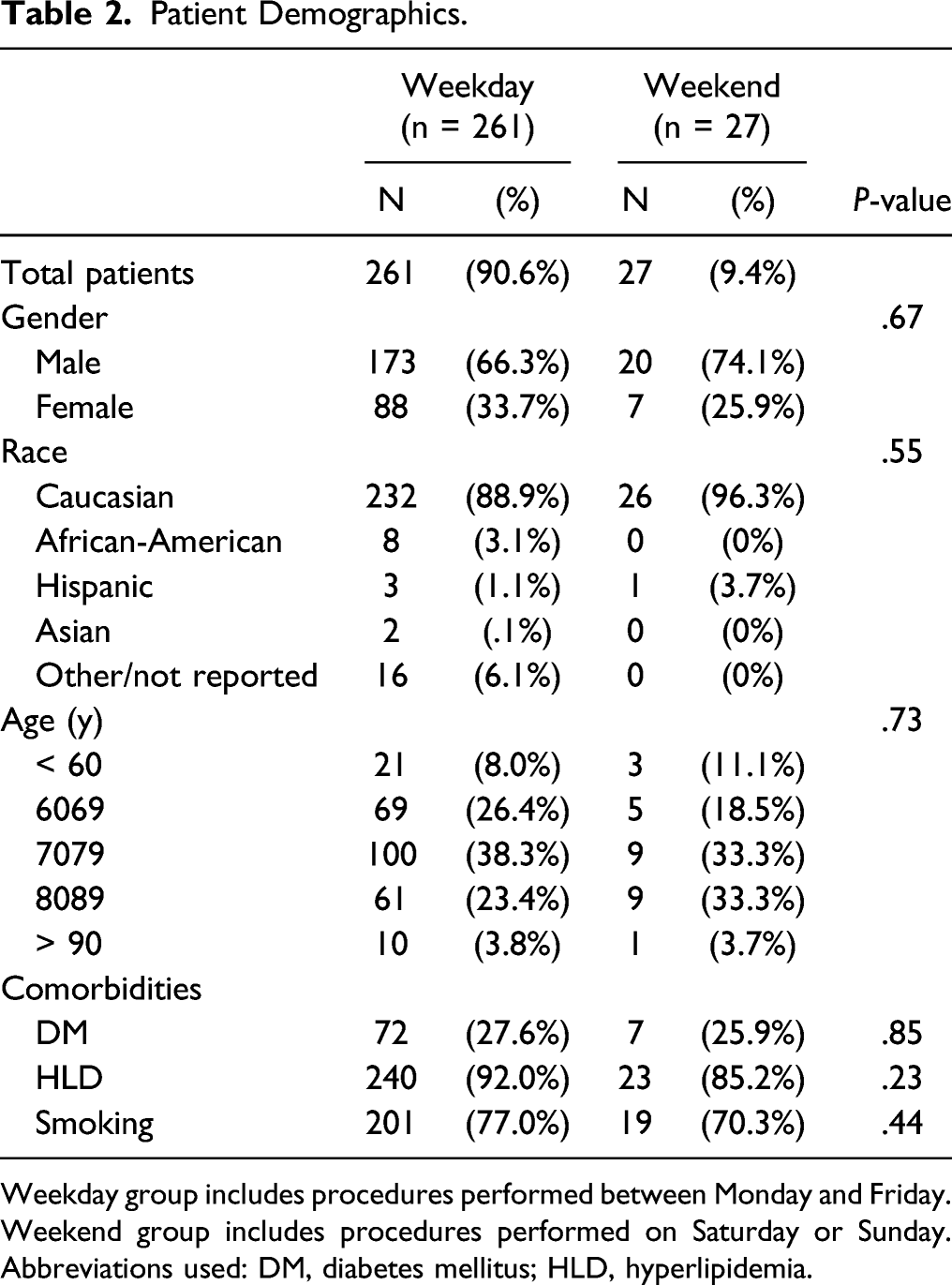
Weekday group includes procedures performed between Monday and Friday. Weekend group includes procedures performed on Saturday or Sunday. Abbreviations used: DM, diabetes mellitus; HLD, hyperlipidemia.
Operative Details.
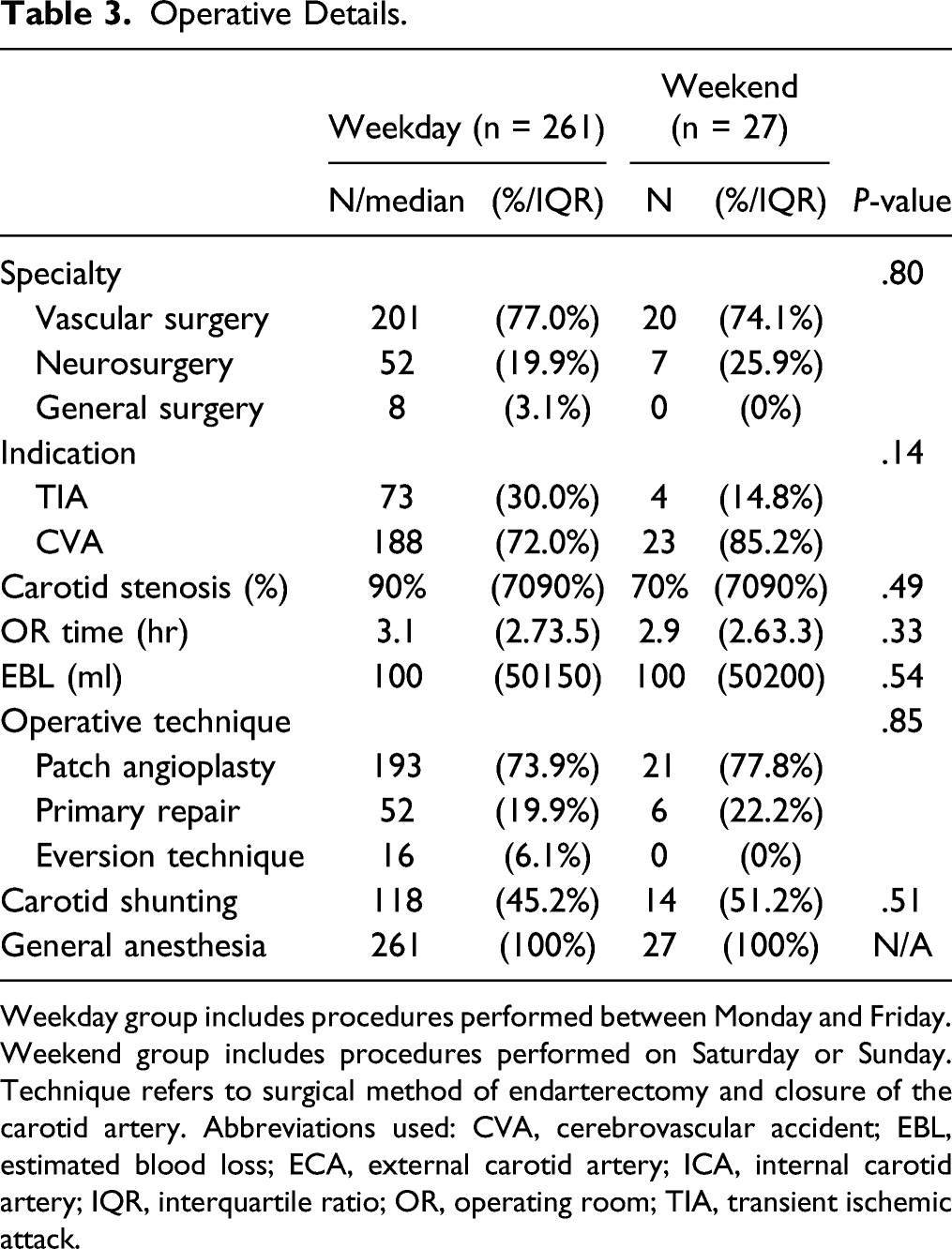
Weekday group includes procedures performed between Monday and Friday. Weekend group includes procedures performed on Saturday or Sunday. Technique refers to surgical method of endarterectomy and closure of the carotid artery. Abbreviations used: CVA, cerebrovascular accident; EBL, estimated blood loss; ECA, external carotid artery; ICA, internal carotid artery; IQR, interquartile ratio; OR, operating room; TIA, transient ischemic attack.
Hospital Outcomes and Complications.
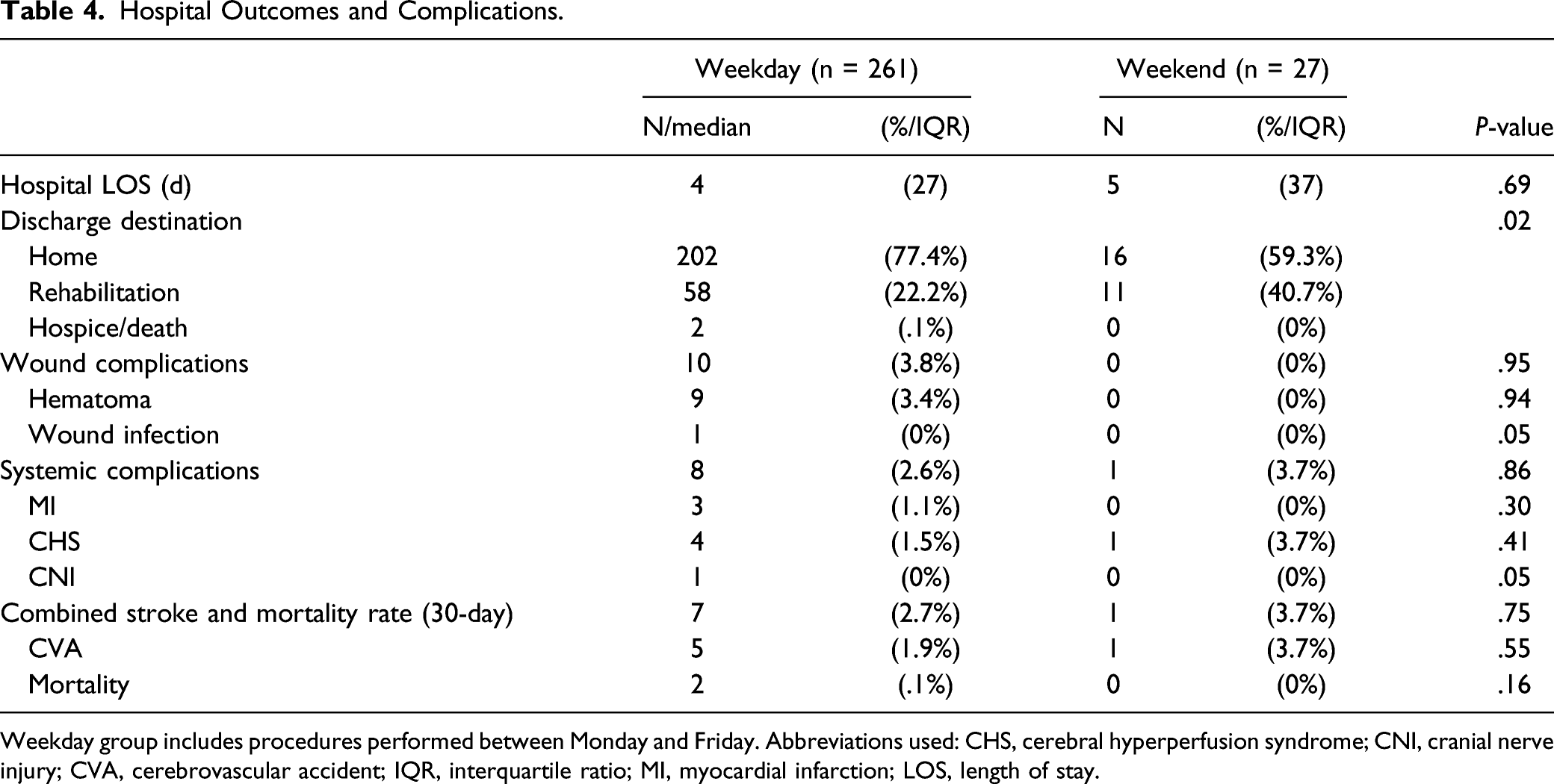
Weekday group includes procedures performed between Monday and Friday. Abbreviations used: CHS, cerebral hyperperfusion syndrome; CNI, cranial nerve injury; CVA, cerebrovascular accident; IQR, interquartile ratio; MI, myocardial infarction; LOS, length of stay.
Risk Factors for Postoperative Stroke and 30-Day Mortality After CEA.
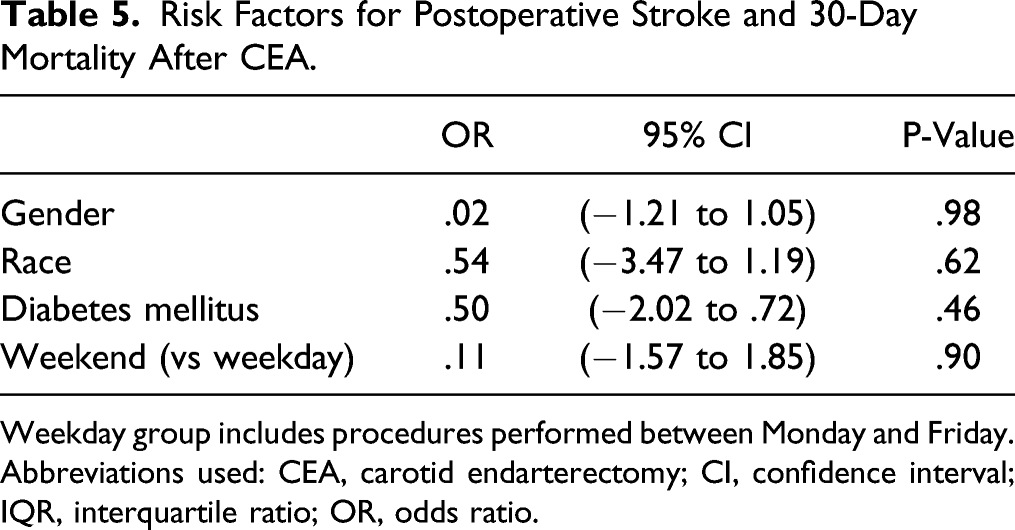
Weekday group includes procedures performed between Monday and Friday. Abbreviations used: CEA, carotid endarterectomy; CI, confidence interval; IQR, interquartile ratio; OR, odds ratio.
Discussion
In this retrospective analysis, we investigated the “weekend effect” phenomenon in CEA for symptomatic stenosis. There were no differences in patient outcomes, including postoperative stroke and death, between weekday and weekend surgery. After adjusting for patient factors, weekend surgery was not identified as a risk factor for postoperative complications. These findings suggest that CEA is not impacted by the “weekend effect,” and surgical revascularization should not be withheld on account of a weekend procedure.
The “weekend effect” is a well-described phenomenon in modern healthcare. Nearly 200 studies have been published regarding this phenomenon across both surgical and nonsurgical specialties. In one of the largest studies among surgical patients, in 2011, Ricciardi et al. 12 investigated discharge data from nearly 30 million patients utilizing the Nationwide Inpatient Sample database. The authors discovered a significantly higher mortality rate for patients admitted for nonelective indications during weekends (2.7%) compared with weekday admission (2.3%, P < .001). After adjusting for patient factors, the “weekend effect” persisted, with an odds ratio (OR) of 1.10 (95% confidence interval [CI]: 1.101.11) for mortality during weekends. Subsequently, in 2016, Ricciardi et al. 13 examined the role of patient safety indicator (PSI) events on weekend vs weekday admission. Among 28 million patient admissions, the PSI rate was 1.5% for both weekend and weekday groups. Interestingly, patients who suffered a PSI event had a 7% higher risk of mortality on weekends compared with weekday admissions. Moreover, weekend patients had higher complication rates, including postoperative wound dehiscence, hip fractures, and surgical inpatient death. Similar studies have been performed in many different countries, with the majority coming to the same conclusion—patient mortality is higher on the weekend.
The “weekend effect” is also prevalent in vascular surgery. Higher weekend mortality rates have been reported for ruptured aortic aneurysms,9,10 aortic dissection, 9 and lower extremity revascularization procedures. 11 In 2018, O’Donnell et al. 14 first reported a significant “weekend effect” on patient outcomes after CEA. Utilizing the SVS Vascular Quality Initiative (VQI) database, a total of 86,123 patients were identified who underwent CEA from 2003 to 2018. Among these patients, 53% were asymptomatic and 47% were symptomatic. Among asymptomatic patients, weekend CEA was associated with higher odds of postoperative stroke/death (OR = 2.3 (95% CI: 1.14.8)) and prolonged hospital LOS (OR = 3.6 (95% CI: 2.74.7)). Among symptomatic patients, postoperative stroke/death odds were greater in patients suffering from stroke (OR = 2.2 (95% CI: 1.52.3)) but not from transient ischemic attack (TIA) (OR = 1.2 (95% CI: .62.1)). The authors concluded that weekend CEA should be avoided in asymptomatic patients, and any symptomatic patients presenting with stroke.
Our results differ from those of O’Donnell in that we did not observe any “weekend effect” in symptomatic patients. Two reasons may explain this discrepancy. First, our patient data was collected from a regional, multi-institutional database whereas O’Donnell utilized the SVS VQI database. The VQI registry a self-reported database (from both physicians and hospitals) and despite its many strengths, it remains vulnerable to selection bias. 15 Second, in contrast to the heterogeneous mix of hospital and surgeon volumes in the VQI, our institutional experience has benefited from a protocolized, team-based approach for patients presenting with symptomatic carotid stenosis.
At our institution, where the majority of CEAs were performed, we have found that multidisciplinary management plays a key role in optimizing patient outcomes regardless ofweekday or weekend procedure. Vascular surgery, neurology, cardiology, physical therapy, speech language therapy, and visiting nurses are all integral to the care of patients with symptomatic carotid stenosis. At time of initial presentation, the neurology stroke team is involved early to determine whether the patient is a candidate for thrombolytic therapy. All patients undergo carotid duplex ultrasound as part of their stroke evaluation, as CT angiogram may inaccurately estimate the degree of stenosis. This requires coordination with the vascular technician and interpreting physician. All patients are started on full-dose aspirin on admission, and clopidogrel is strongly considered if there are no contraindications. Patients are maintained on this antiplatelet regimen until time of surgery. If carotid stenosis is considered to be the etiology of the patient’s neurologic deficit, then cardiology is also consulted for preoperative cardiac clearance. Depending on the patient’s clinical presentation, clearance may entail an echocardiogram or a stress test, which is decided on by the cardiology consultant. Once the patient has been cleared for surgery, the procedural details and risks are discussed with the patient prior to proceeding with the operation. A dedicated vascular team is present regardless of weekday or weekend procedure, and includes vascular anesthesiologists, vascular-trained scrub nurses, and a senior vascular trainee (fellow or resident). All procedures are performed during daytime hours, as this maximizes the involvement of ancillary staff members. In the postoperative phase, physical therapists and speech language therapists are involved when appropriate for recovery. Clopidogrel is discontinued if it was initiated for carotid disease, and patients are maintained on full-dose aspirin only. Finally, for patients discharged home, visiting nurse services are offered, and they are educated on symptoms concerning wound infection and CHS.
The results on this study must be taken in context of several limitations. First, symptomatic disease reflects a large spectrum of deficits, from transient monocular deficits to disabling hemiparesis. Our records do not report the severity of symptoms based on known scales, such as the modified Rankin score. Therefore, we were not able to stratify and risk-adjust patients based on the degree of their neurological disability. Second, the data presented are from a regional, multi-institutional database. While these results describe our recent outcomes with CEA, they may not be generalizable on a national level. Third, given the small size of our patient cohort, our study may not have detected small but important differences in outcomes. Fourth, the time of the neurological index event is not reliably reported within medical records. Therefore, we were not able measure the time interval from symptom-onset to surgical intervention.
Conclusion
In our multi-institutional experience, we found that weekend surgery does not adversely affect postoperative outcomes for CEA in the treatment of symptomatic carotid stenosis. These findings suggest that CEA may not be impacted by the “weekend effect,” as described for other surgical procedures. Urgent revascularization should not be withheld on account of a weekend procedure, in similar academic medical centers.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.