
Abstract
Keywords
Introduction
In patients with peripheral arterial disease (PAD) in the lower limbs, multiple treatments may be required because of the distribution of lesions in multiple areas, re-stenosis, or occlusion even after treatment. The merits of endovascular treatment (EVT) for PAD include relative ease of reoperation, low perioperative mortality, and short hospital stay. 1 The advantages of using the common femoral artery (CFA) as an access route for EVT for PAD include safety in terms of hemostasis, accessibility to target lesions (especially for lesions below the knee), the availability of treatment devices, and the potential for catheterization without contacting the cerebral and main visceral arterial branch.2,3
Endarterectomy (EA), developed in the 1940s, is a common treatment for atherosclerotic lesions that develop in the CFA; it also yields satisfactory results in hybrid operations in which EVT for lesions outside of the CFA is performed simultaneously. 4 Conversely, EVT for CFA has been performed following recent advances in EVT. However, as stent placement in the CFA can result in complications, it may be difficult to use the CFA as an access route for subsequent necessary interventions. 4
In contrast, using the CFA as an access route for cardiac catheterization should be avoided after operating a lesion in the inguinal region because of several complications. 5 We sometimes experience difficulty with sheath insertion in our practice when the CFA is used as an access route after EA because of subcutaneous tissue scarring or difficulties maintaining hemostasis. However, we are not aware of reports on the safety of using the CFA as an access route or on the ease of sheath insertion and time course after EA.
We conducted a retrospective study on the ease of sheath insertion, the rate of successful insertions, and the achievement of hemostasis. Furthermore, regarding the ease of sheath insertion, we evaluated the number of days that elapsed from EA to EVT and the difference in the repair method of the CFA during EA, namely, simple closure or autologous patch repair. We aimed to evaluate the safety of the CFA as an access route for EVT after EA.
Material and Methods
EA was performed in 147 consecutive CFAs of 125 patients in our institution from January 2013 to December 2020. Of these, we included 19 consecutive patients (21 limbs, 40 cases) in whom the CFA repaired with EA was subsequently used as an access route for EVT for PAD. Interventions for PAD after EA were performed in patients with > 75% vessel restenosis and/or new stenosis, determined with computed tomography angiography or ultrasound tests performed at the time of exacerbation of symptoms or at regular visits. In all cases, the interventional method (open surgery or EVT), target region of treatment, and access site for EVT were decided during a preoperational vascular-surgery conference. The approval for the study was obtained from the ethical committee of the Tokyo Medical and Dental University (reference number M2020-126). Written informed consent for the retrospective study was obtained from patients at the time of each EA or EVT.
In our institution, the contralateral CFA is normally used as an access point for EVT after EA. However, there are exceptions such as cases in which EA was performed for both CFAs, proximal anastomosis of femoropopliteal bypass in the contralateral CFA, difficulties due to the tight aortic bifurcation, lesions located in the lower thigh on the same side, and complicated lesions in the area of the superficial femoral arterypopliteal artery.
Surgical Operation
EA was performed under general anesthesia in all cases. A vertical skin incision for EA was made in 16 limbs and an oblique incision in 5 limbs. The EA sites were the CFA alone in eight limbs, the area from the CFA to the superficial femoral artery in seven, the area from the CFA to the profunda femoris artery in four, and the areas from the CFA to both the superficial femoral artery and the profunda femoris artery in two. We performed EA with a longitudinal incision in the anterior surface of the artery, and removed the thickened intima and inner media, leaving behind the outer part of the media and the adventitia. For CFA repair, simple closure was performed in 9 limbs, and patching with autologous vessels such as the great saphenous vein was performed in 12 limbs. Therefore, all patients’ CFA were repaired with autologous tissue. We performed simple closure when the diameter of the CFA was ≥ 10 mm and autologous patch repair when the diameter of the CFA was <10 mm. Hybrid operations, in which EVT was added to EA, were performed in 18 limbs.
Endovascular Treatment
The use of oral antiplatelet drugs and anticoagulants was continued even on the day of the procedure in all cases. EVT was performed under local anesthesia in the operating room in all cases. Fluoroscopy was used to identify the location of the femoral head, followed by ultrasound-guided puncture of the CFA at a 45° angle to the skin in all cases. In all cases, we punctured the anterior surface of the CFA under ultrasound guidance, which was achieved by placing the ultrasound probe parallel to the artery and visualizing the artery and the puncturing needle in the longitudinal direction on one screen. The ultrasound probe was placed parallel to the artery for maximum visualization of its anteroposterior diameter.
Early EVT was defined as EVT performed within 6 months after EA. Difficult sheath insertions were defined as those in which additional devices were used to insert a sheath with the scheduled diameter; normal sheath insertions were defined as those in which no additional devices were necessary. Additional devices included a sheath with a smaller diameter used for dilation (bougie) or a half-stiff or stiff Radifocus™ guidewire (.035 inch; Terumo, Tokyo, Japan) to straighten the insertion route (cases in which only the inner tube of the sheath with the scheduled diameter was used for bougie were grouped with cases of normal sheath insertions). For cases with a difficult sheath insertion, cases in which a sheath with the scheduled diameter could not be inserted were defined as failed sheath insertions. Where the time from EA to EVT was less than 1 year, the period was divided into two 6-month periods; when the time from EA to EVT was 1 year or longer, the period was divided into years.
Intravenous injection of heparin was administered at a dose of 50 U/kg body weight, and an additional 1000 U was injected every hour during the operation. To achieve hemostasis, either an ExoSeal™ vascular closure device (Cordis, Warren, NJ, USA) or manual compression was chosen according to the surgeons' preference, with 10 min of routine compression in the former and 15 min in the latter. Hemostasis was confirmed using ultrasound after compression.
The patients were required to stay in a supine position for the first 3 h, stay in bed for the night, and allowed to walk the following day. In all cases, examination of the inguinal region was performed in the morning on the following day and at the outpatient visit within 1 month after discharge. Follow-up was performed every 36 months on an outpatient basis.
Statistics
All statistical analyses were performed using IBM SPSS Statistics for Windows (version 20.0, IBM Corp., Armonk, NY, USA). Data were presented as median values (25th–75th percentiles). Fisher’s exact test was used to compare the difficulty of sheath insertion between simple closure after EA and autologous patch repair. A P value < .05 was defined as a statistically significant difference.
Results
Patient Characteristics.
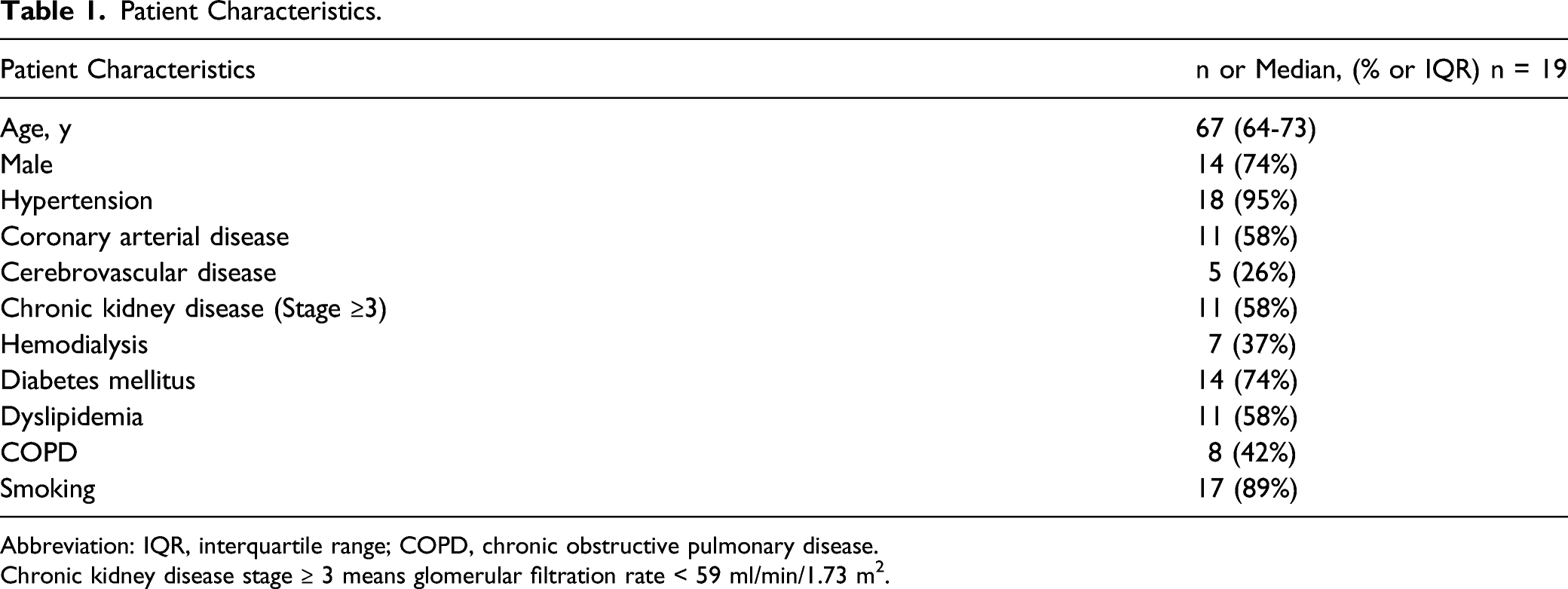
Abbreviation: IQR, interquartile range; COPD, chronic obstructive pulmonary disease.
Chronic kidney disease stage ≥ 3 means glomerular filtration rate < 59 ml/min/1.73 m2.
Characteristics of Endovascular Treatment After Endarterectomy.
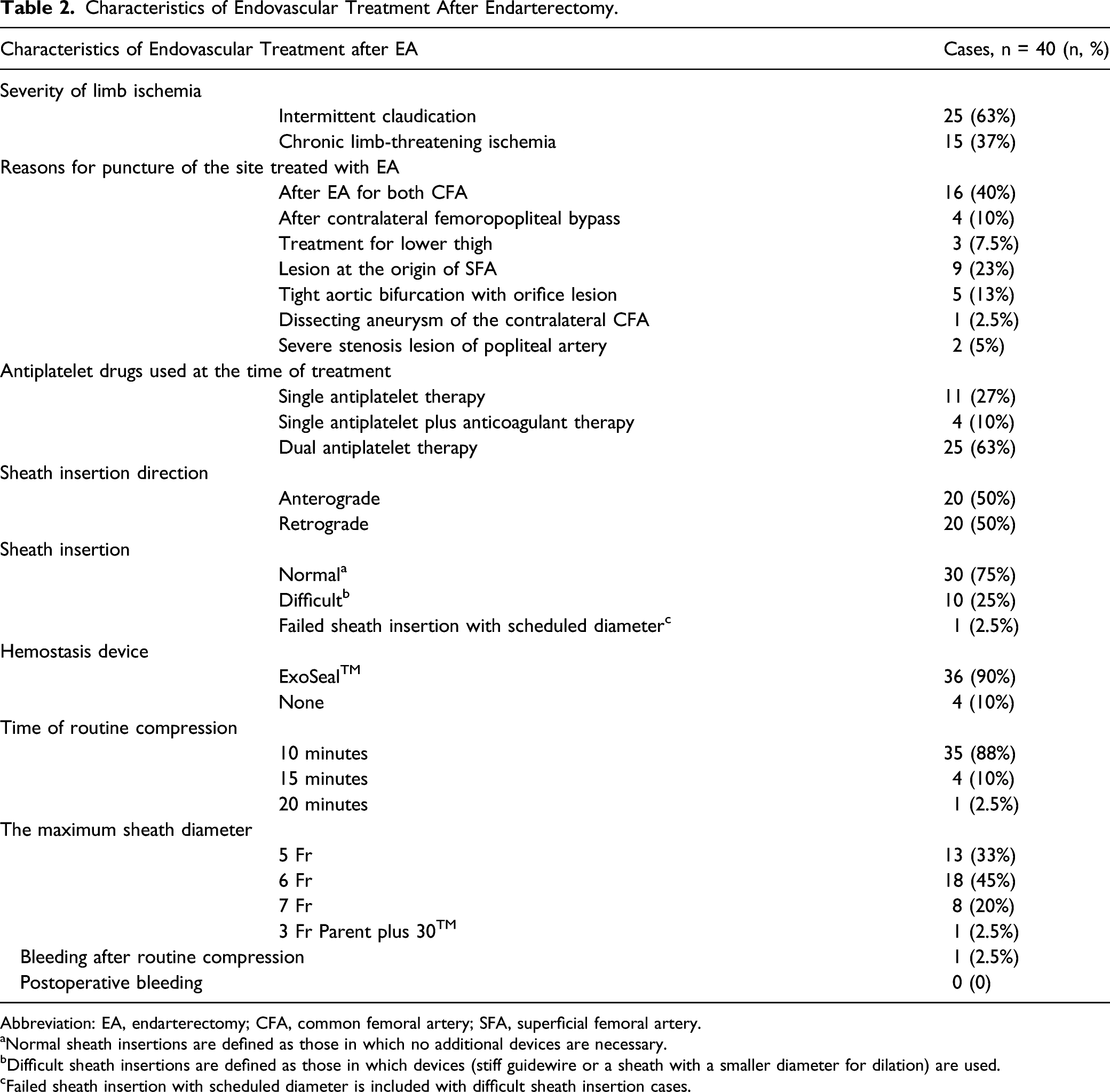
Abbreviation: EA, endarterectomy; CFA, common femoral artery; SFA, superficial femoral artery.
aNormal sheath insertions are defined as those in which no additional devices are necessary.
bDifficult sheath insertions are defined as those in which devices (stiff guidewire or a sheath with a smaller diameter for dilation) are used.
cFailed sheath insertion with scheduled diameter is included with difficult sheath insertion cases.
The median time from EA to any EVT was 1106 (6061355 (2575%)) days (includes all 40 cases). The four shortest times from EA to EVT were 28, 117, 161, and 168 days, constituting the early EVT groups. In these cases with short intervals, EVT was performed due to rapid aggravation of symptoms. All four cases were normal sheath insertions in which hemostasis was achieved; however, as a puncture had to be performed shortly after EA, these procedures were performed with extra care.
There were 10 difficult sheath insertions, of which one was a failed sheath insertion. There was no significant difference (P = .24) in time from EA to EVT between the 30 cases of normal sheath insertion (1202 (7101409 (2575%)) days) and the 10 cases of difficult sheath insertions (923 (4221068) days).
The number of normal and difficult sheath insertions in each period is indicated in Figure 1. The rate of difficult sheath insertions peaked between 6 months to 1 year after EA and gradually decreased after that. Among 15 cases in which EVT was performed between 6 months to 3 years after EA, there were 7 difficult sheath insertions, accounting for 47% of cases. In contrast, more than 3 years after EA, the rate of difficult sheath insertions decreased to 14%. Percentage of difficult sheath insertion cases in each period. Abbreviations: EVT: endovascular treatment, EA: endarterectomy. Normal sheath insertions are defined as those in which no additional devices are necessary. Difficult sheath insertions are defined as those in which additional devices (stiff guidewire or a sheath with a smaller diameter for dilation) are used.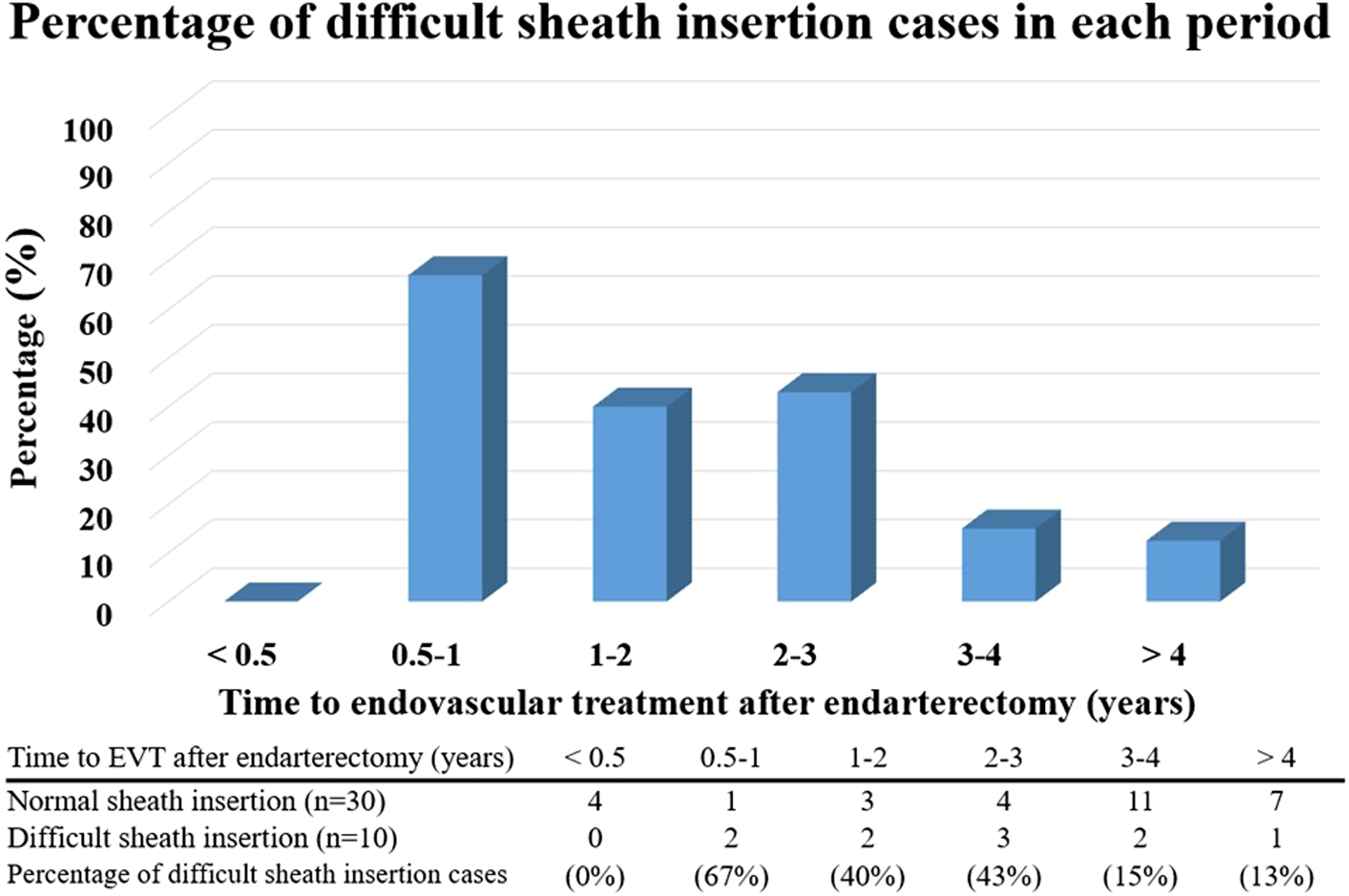
Of the nine limbs in which there were difficult sheath insertions (10 cases), the occurrence of multiple EVTs is as follows: twice for one limb, three times for two limbs, and five times for one limb. For three of these four limbs, the difficult sheath insertion was encountered only in the initial EVT; during subsequent EVTs, the resistance was lower, allowing normal sheath insertions. In the remaining limb, both the first and second sheath insertions were difficult.
Difficulty of Sheath Insertion by CFA Repair Method.
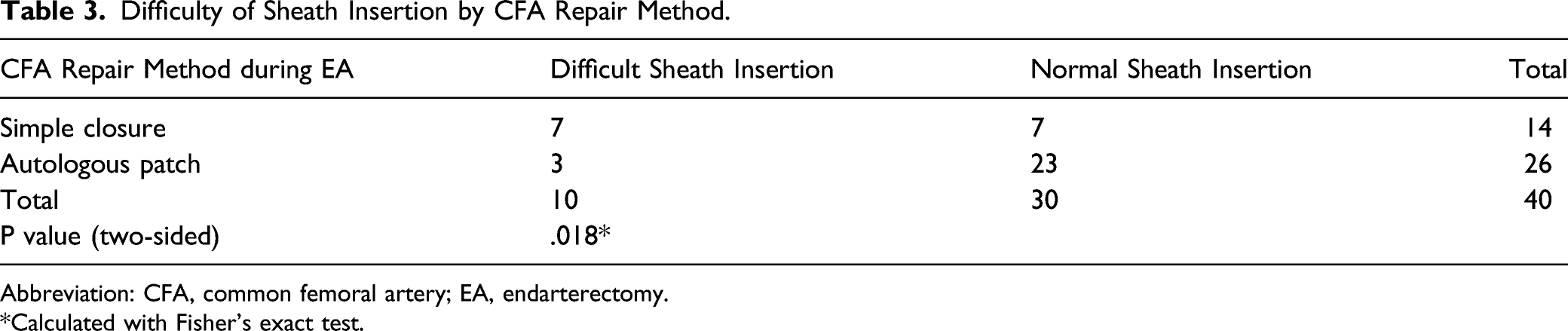
Abbreviation: CFA, common femoral artery; EA, endarterectomy.
*Calculated with Fisher’s exact test.
In the case of the failed sheath insertion, 1990 days had passed since the EA was repaired via simple closure of the CFA, and a treatment plan, in which the stent would be placed in the contralateral iliac and femoral arteries via a crossover approach from the CFA, was developed. However, retrograde insertion of 4-Fr and 5-Fr sheaths (Terumo, Tokyo, Japan), as well as of a 6-Fr guiding sheath (DestinationTM; Terumo, Tokyo, Japan), failed, and the treatment was completed only with balloon dilation of the iliac and superficial femoral arteries through a sheathless, 3-Fr guiding sheath (Parent Plus 30TM; Medikit Co., Ltd., Tokyo, Japan). After the guiding sheath was removed, manual compression was performed, and hemostasis was confirmed.
There was only one case in which hemostasis could not be achieved after routine compression, a case in which EVT was performed 1108 days after EA. The patient, in this case, received dual antiplatelet therapy with aspirin and clopidogrel. In this case, EVT was performed for occlusion of the femoropopliteal graft bypass in the contralateral limb. After we performed the endovascular procedure, the inserted 7-Fr sheath was removed using the ExoSeal hemostasis device. Since ultrasonographic evaluation after the 10-min compression revealed a hematoma around the site of the ExoSeal application, a further 10-min compression was performed using an echo probe, which resulted in hemostasis.
There were no cases of bleeding from the puncture site and no cases in which surgical intervention was required for a false aneurysm. None of the patients exhibited indications of infection, including redness, swelling, abscess at the puncture site, or a body temperature of 37.5°C or higher. The median follow-up period after each EVT in all cases was 786 (4891079 (2575%)) days. Drop-outs occurred in five cases, including three due to death (one case each of coronary artery disease, chronic renal failure, and unknown cause of death), one case in which the patient had experienced difficulty in visiting the hospital, and one case in which CFApopliteal artery bypass was performed for superficial femoral artery occlusion 310 days after EVT.
Discussion
In this study, the safety and success rate of CFA access for EVT after EA were evaluated. There were no cases in which surgical procedures were required after operation due to complications associated with CFA access; however, there were 10 cases of difficult sheath insertions, including one failed sheath insertion. The rate of difficult sheath insertions peaked between 6 months and 1 year after EA and gradually decreased after that.
In cases with difficult sheath insertions, scar tissue between the vessel and skin is considered a major contributor. When the sheath was inserted through the hard scar tissue, the tissue was caught in the gap between the margin of the sheath and the inner tube. Therefore, the .035-inch wire was changed to a half-stiff wire to straighten the insertion route, 6 and the diameter of the sheath was gradually increased to ensure successful insertion. We did not perform a nick-and-tunnel approach, 5 in which a small nick is creased and subcutaneous tissue is removed with forceps, because of the risks of damage caused by the lack of a border between the scar tissue and vascular tissue and the difficulty in subsequent hemostasis. In the case with failed sheath insertion, neither a 4-Fr nor a 5-Fr sheath could be inserted, and we had to revert to a sheathless, 3-Fr guiding sheath. This guiding sheath has an outer diameter of 5.3 Fr (1.76 mm) and an inner diameter of 4 Fr (1.50 mm), with a smaller gap between the two. In addition, the guiding sheath has a hydrophilic coating. These characteristics may have been of assistance in getting the sheath to penetrate the hard scar tissue.
The difficulty with sheath insertion changed over time in our study, as demonstrated in Figure 1. This may be explained by the dynamics of scar tissue formation. Scar tissue is formed in the final healing process of tissue defects, such as surgical wounds. It is composed of the same protein (collagen) as the tissue that it replaces, but the fiber composition is different; instead of the random, basketweave formation of collagen fibers in normal tissue, collagen cross-links form a pronounced alignment in a single direction in fibrotic tissue. This, in addition to a lack of elastic fibers, contributes to the stiffness of scar tissue. 7 These processes of extracellular matrix remodeling are the most active in the first 6 months after tissue damage, strengthening the scar tissue, but become gradually less active thereafter. 8 Considering these underlying conditions, we believe that successful sheath insertion in cases of early EVT can be achieved since the maximum strength of the scar tissue has not been achieved. This would also explain why the rate of difficult sheath insertions peaked 6 months to 1 year after EA and gradually decreased thereafter.
During EVT after EA, there may be a risk of damage to the suture site made at the time of EA, caused by the needles or sheaths used in the insertion procedure. Hemostasis after vascular surgery is achieved with suture threads and surrounding tissues. 9 In cases in which vascular anastomosis is performed, suture threads play important roles in early hemostasis after surgery. For such purposes, polypropylene yarn, such as ProleneTM (Ethicon, Bridgewater, NJ, USA), a non-absorbable suture, is generally used. However, in cardiovascular surgery in pediatric patients, absorbable sutures have been used for vascular anastomosis. In one study of PAD treated using vascular anastomosis, neither postoperative bleeding nor false aneurysm occurred after using polydioxanone, an absorbable suture. 9 The tensile strength of polydioxanone diminishes by 42% in 4 weeks and by 86% in 8 weeks, 10 and it cannot be identified with the naked eye 180 days after use. 11 Based on the above results, we suggest that a reasonable strategy is to perform EVT after the patient’s condition has been monitored for at least 6 months after EA. Therefore, we defined cases in which EVT was performed within 6 months after EA as early EVT. Hemostasis was achieved in all four cases of early EVT in our study, likely because of the extra care taken, knowing that the risk was higher. In this study, cases in which artificial blood vessel patches were used at the site of puncture in the CFA were not included. In cases in which artificial blood vessel patches are used, permanent suture threads should be used due to the risk of formation of false aneurysms caused by the rupture of artificial objects. Therefore, puncture near the suture line should be avoided.
In this study, during EA surgery, the CFA was anteriorly incised in the longitudinal direction and repaired with autologous tissue. Simple closure of the CFA yielded a higher proportion of difficult sheath insertions than did autologous patching. With simple closure, the suture line can be placed directly above the CFA, whereas, in patch repair, the patch is positioned directly over the incision and the suture line is formed on both sides. The postoperative arterial tissue healing can spread along the suture line, 9 which can result in scar formation.7,8 As we punctured the most anterior surface of the CFA under ultrasound guidance and inserted the sheath along the artery during EVT, we speculate that the scar had a greater effect on sheath insertion in simple closure cases, where the suture line is directly above the artery.
In this study, all EVTs were performed under ultrasound guidance, which probably contributed to the prevention and treatment of bleeding as it allowed the accurate puncture of the CFA, confirmation of hemostasis after routine compression, and compression hemostasis using a probe. It has been previously reported that punctures below the CFA bifurcation or above the inferior epigastric artery are related to bleeding complications 12 ; therefore, accurate puncture of the CFA is important from the viewpoint of hemostasis. In addition, ultrasound-guided compression is useful for the treatment of bleeding, including the false aneurysm. 13
This study had several limitations. First, we included a small number of cases from a single institution; therefore, additional investigation is necessary. Second, because this was a retrospective study, there were no clear criteria for using a new device for sheath insertion or a vascular closure device, and the choice was made based on the operator’s preference. In all cases, the interventional methods were decided during preoperational vascular surgery conferences; however, over the course of the study, treatment strategies changed, primarily because of the progression of EVT, which may have influenced the overall choice of treatment and resulted in a patient selection bias. Third, in this study, the time taken for sheath insertion was not measured; therefore, the difficulty of sheath insertion could not be evaluated with regard to this aspect. Furthermore, because we generally do not use artificial blood vessel patches for CFA because of the risk of infection or pseudoaneurysms, cases in which an artificial blood vessel patch was used in the anterior part of the CFA, a puncture site, were not included in this study. No biologic patches were used for CFA repair after EA during the period of this study in our institution, as bovine pericardial patches with sufficient durability for CFA repair after EA were not covered by medical insurance until 2020 in Japan.
Conclusion
In this study, sheath insertion was difficult (likely due to postoperative scarring) in 25% of cases in which EVT was performed using a vessel previously treated with EA as an access route. The rate of difficult sheath insertions peaked 6 months to 1 year after EA and gradually decreased thereafter. The rate of difficult insertions was 47% from 6 months to 3 years and 14% 3 years after EA. In addition, 50% of cases undergoing simple closure repair of the CFA exhibited difficult sheath insertions, whereas only 12% of cases undergoing autologous patch repair did. As this difference was statistically significant, autologous patch repair may be preferable for closure of the CFA after EA in future cases of EVT. However, even in cases of difficulty, scheduled diameter sheath insertion was achieved in 97.5% by gradually increasing the diameter of the sheath or using a stiff wire. No additional surgical procedures were required for complications, including bleeding at the puncture site. These results suggest that EVT using the CFA as an access route after EA is safe and that the timing of EVT after EA of more than 3 years after EA as well as the autologous patch method of CFA repair during EA surgery can play important roles reducing the difficulty of sheath insertion, possibly because of the dynamics of scar formation.
Footnotes
Acknowledgments
The authors are grateful to Dr. Yoshinori Inoue (Ambulatory Vascular Surgical Clinic Tokyo) for his kind support and insightful advice regarding this article.
Author’s Contributions
S.K. conceived and designed the study and performed the analysis. S.K and K.I. prepared the manuscript. All authors performed the research, discussed the results, and contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.