
Abstract
Iodized oil-based lymphangiography (LAG) is a well-established diagnostic exam during the workup of postoperative lymphatic leaks. Computed tomography (CT) has been shown to be a useful complement to optimize treatment planning and can easily be performed after conventional LAG. The treatment options for lymphatic leaks include conservative dietary modification, sclerotherapy, embolization, and surgery. We present a case of a 48-year-old man who developed a symptomatic left retroperitoneal lymphatic fluid collection after left nephrectomy, complicated by postoperative retroperitoneal abscess. Retroperitoneal duct leak was confirmed via ultrasound-guided intranodal LAG and post-LAG CT. This leak was successfully managed with N-butyl cyanoacrylate glue embolization of the leaking lymphatics via fluoroscopic-guided catheterization of the leak via percutaneous access through the lymphatic fluid collection.
Introduction
Lymphatic leaks are an uncommon complication after thoracoabdominal surgery and have been reported after urologic, thoracic, vascular, gastrointestinal, gynecologic, hepatobiliary, and transplant surgeries. High-volume lymphatic leaks may result in the loss of significant protein, lipid, water, and electrolytes and are associated with increased postoperative mortality due to malnutrition, immune compromise, and sepsis.1-3 Lymphatic leaks are a challenging condition with wide-ranging treatment options. These options include (1) conservative management with medium chain fatty acid dietary restriction, fluid replacement, and somatostatin analogue medication; (2) radiological intervention with percutaneous drainage, sclerotherapy, or embolization; or (3) surgical treatment.1-3 Lymphangiography (LAG), either pedal or intranodal, is the traditional method utilized to localize the site of lymphatic leak prior to either surgery or endovascular intervention.1,2,4-6 In this report, we present the successful treatment of a retroperitoneal lymphatic leak after nephrectomy via percutaneous translymphocele catheter embolization under fluoroscopy.
Case Report
A 48-year-old man underwent left nephrectomy at an outside hospital for renal cell carcinoma (Figure 1A). Two weeks post-surgery he presented in sepsis with fever, hypotension, tachycardia, leukocytosis (white blood cell count: 34.1 × 10^9/L), and lactic acidosis (lactate: 3.4 mmol/L). CT in the emergency department identified left renal fossa abscess (Figure 1B). Small-volume ascites and pleural effusions were also present. The patient was fluid resuscitated, started on IV antibiotics, and underwent percutaneous 10.2 French drain placement by radiology. The patient’s clinical condition rapidly improved; however, drain output which was initially purulent appearing became milky in appearance with output ranging from 1 to 1.5 L per day with the patient developing pre-syncopal symptoms. Repeat CT 1 week post drain placement (Figure 1C) demonstrated persistent fluid collection despite drain placement with near complete resolution of ascites and pleural effusions. Fluid studies were sent from the drain which identified an elevated triglyceride level (1419 mg/dL) compatible with chylous retroperitoneal lymphatic leak. Due to volume, protein, lipid, and electrolyte loss, inpatient nutrient and fluid repletion were required with PICC line placement. The patient’s serum albumin nadir was 1.3 g/dL. The patient was initially managed with octreotide and medium-chain fatty acid diet. However, the patient could not tolerate octreotide due to adverse reaction (oral facial numbness and taste alteration). The patient was transitioned to parenteral nutrition. Drain output did not significantly diminish (∼0.9-1.5 L per day) with conservative management. Contrast-enhanced axial CT images: (A) demonstrating large left renal carcinoma 1 month prior to nephrectomy, (B) demonstrating left retroperitoneal fluid collection with air compatible with abscess/infected lymphocele 2 weeks post-nephrectomy, and (C) demonstrating persistent fluid collection despite left retroperitoneal pigtail drain placement.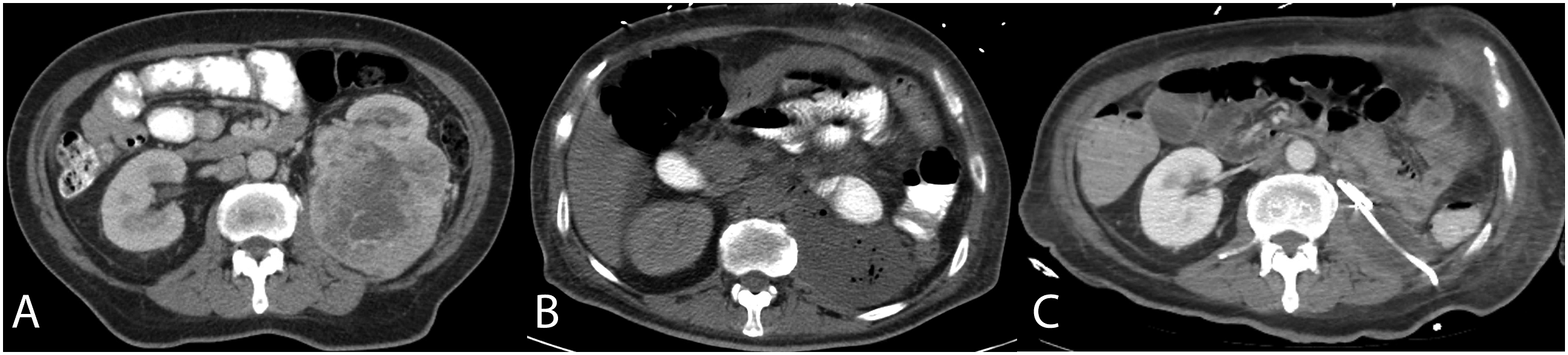
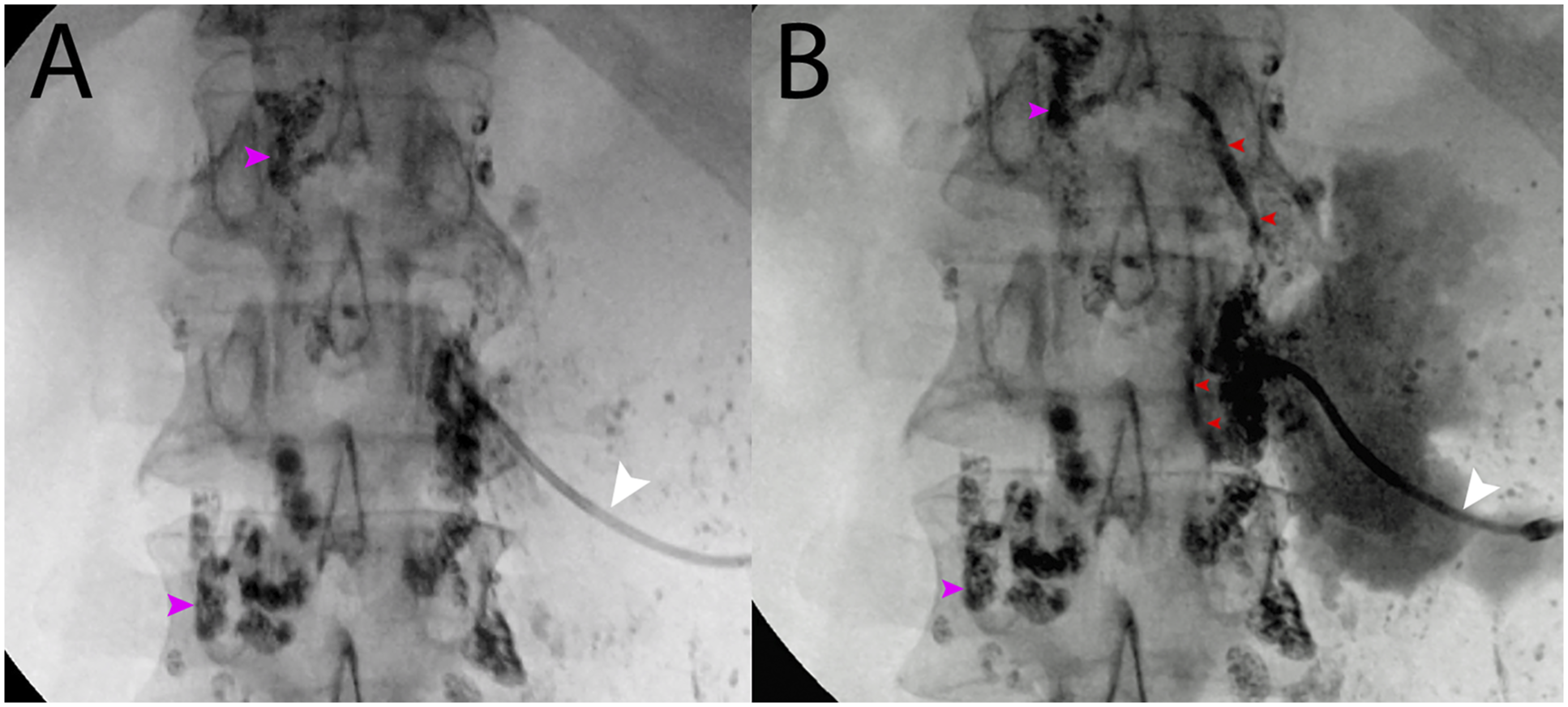
The patient underwent ultrasound-guided intranodal LAG to characterize the leak on post-nephrectomy day 33/post-drain placement day 16. LAG demonstrated retroperitoneal lymphatic leak at the level of L2 (Figure 2A), and post-LAG CT was also performed elucidating the site of injury (Figures 2B-2C). Due to relative ease of procedure and low risk of side effects, the decision was made to attempt sclerotherapy. On day 35, 50 mL 98% ethanol was instilled in the retroperitoneal lymphatic cavity via the existing drain and allowed to dwell for 1 hour while the patient changed positions. The ethanol was subsequently aspirated. Only a mild decrease in drain output was noted over the next 6 days (640-850 mL per day). As initial sclerotherapy had not sufficiently decreased output and the patient still required parenteral nutrition and fluid management, percutaneous translymphocele embolization was performed under fluoroscopy (Figure 3). In interventional radiology, the indwelling drain was exchanged under fluoroscopy for a 6 Fr vascular sheath. Through the vascular sheath, a 5F KMP catheter was utilized to probe the location of the leak identified on prior LAG at the margin of L2 (Figure 3A). Gentle small-volume dilute iodinated contrast injection confirmed communication between the catheter tip and retroperitoneal lymphatics at the level of L2. Renegade STC 18 microcatheter was advanced into the visualized lymphatics over Transend .014″ wire (Boston Scientific, Marlborough, MA). Ethiodized oil (Lipiodol, Guerbet, Princeton, NJ) and NBCA glue (Histoacryl Blue, B. Braun, Bethlehem, PA) were then injected until the embolic cast was demonstrated within lymphatics cranial and caudal to the leak catheterization site (Figure 3B). The catheters were removed, and the sheath was replaced with a new 10.2 French pigtail drain to monitor output. On post-procedure day 1, a marked drop in output to 35 mL was demonstrated. The patient’s oral diet was restarted. Output remained ∼25 mL per day and he was discharged 4 days later with subsequent drain removal at follow-up clinic visit in good condition. Conventional intranodal lymphangiogram (A) and immediate post-lymphangiogram coronal maximum intensity (B) and axial CT (C) images demonstrating left retroperitoneal leak at the level of L2 (orange arrowheads) extending to lymphatic fluid collection and drain. Note normal retroperitoneal lymphatic channels (white arrowheads). Pre-embolization fluoroscopic image (A) with 5 Fr diagnostic catheter (white arrowheads) cannulating lymphatic leak at the level of L2. Post-NBCA/lipiodol leak embolization fluoroscopic image (B) with glue cast within retroperitoneal lymphatics cranial and caudal to site of injury (red arrowheads). Note retained lipiodol from prior conventional lymphangiogram within retroperitoneal lymph nodes (purple arrowheads).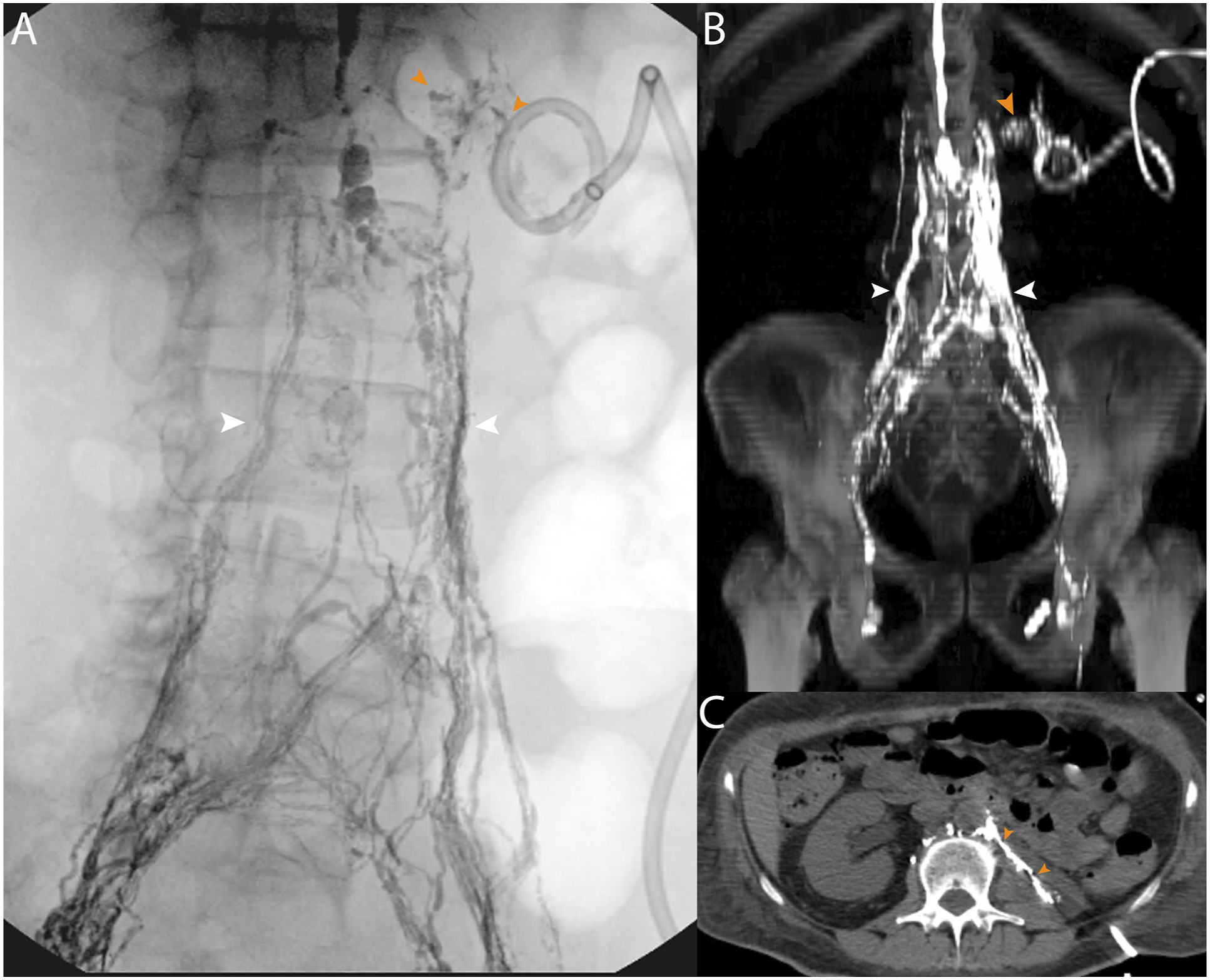
Discussion
Symptomatic retroperitoneal lymphoceles, chylous ascites, or lymphatic fistula are uncommon complications of surgical procedures. In patients with malignancy, however, untreated high-volume chylous fluid loss can lead to a reported mortality near 50% due to the loss of protein, electrolytes, and lymphocyte-rich fluid which increases the risk of infection and malnutrition.2,3 The diagnosis can be suspected upon aspiration of milky fluid from the affected region and confirmed by laboratory presence of chylomicrons or elevated triglycerides in collected fluid. 3 Lymphosctigraphy, conventional LAG with or without CT, or MR LAG may also be used to confirm the diagnosis and/or characterize the source of leak allowing for more informed treatment discussion between surgical and interventional endovascular services.
The majority of lymphatic leaks heal with conservative management including medium-chain fatty acid diet, total parenteral nutrition, somatostatin analogue medication, and/or drain placement.2,3,7-9 In patients who fail these conservative options, such as our patient, treatment options remain varied without consensus of optimal management. 9 The most commonly utilized adjuvant strategy is sclerotherapy with agents including doxycycline, povidone iodine, or ethanol7-9 which was initially attempted albeit unsuccessfully in our case. Sclerotherapy is easy to perform via existing drainage catheters and may be beneficial if multiple leak sites are identified, limiting likely success of targeted embolization. However, it may be suboptimal in high-flow lymphatic leakage, or when a ruptured lymphocele communicates with the peritoneum, or there is direct intraperitoneal lymphorrhea. 10 Furthermore, sclerotherapy also may require multiple treatment sessions. 10
More recently, case reports and small case series have reported success utilizing percutaneous coil or glue embolization either via direct percutaneous needle targeting of the leaking lymphatic under CT or fluoroscopy at time of LAG. 11 The largest reported series of 8 patients undergoing percutaneous translymphocele embolization (the technique used in the index case) demonstrated a clinical success rate of 88%. The authors reported decreasing fluid output from leak sites with mean of 465 mL per day pre-embolization to 42 mL per day post embolization which allowed for drain removal in all but one patient. 10 Had embolization not successfully treated the leak in the index case, surgical intervention had been planned with possible fibrin glue, cautery, or surgical ligation to terminate the leak. As LAG and CT demonstrated the site of leak at the level of L2 posterior to aorta, the likelihood of surgical cure was improved.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Manuscript and images have not been previously published nor have they been submitted for review at another publication.
Chris Bent wrote and edited the manuscript and participated in the patient’s care.
This report conforms with human subjects research guidelines according to the World Medical Association Declaration of Helsinki. The manuscript conforms to the ICMJE Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals. The Riverside University Health System Institutional Review Board waives the requirement for review and informed consent in retrospective case reviews which do not include identifying patient information. Informed consent has been obtained from the patient for publication of the case report and accompanying images.