
Abstract
Introduction
Most renal arteriovenous fistulae occur after renal biopsies but can also result from trauma, surgery, percutaneous interventions, tumors, or erosion of an aneurysm directly into a vein. 1 Isolated renal arteriovenous fistulae due to trauma are rare, accounting for a reported 2–13% of all renal arteriovenous fistulae. 2 Fistulae between the renal artery and inferior vena cava are a rare complication following nephrectomy. A well-documented risk factor for renal arteriovenous fistulae following nephrectomy is mass ligation of the renal pedicle.3-5
The presentation of renal arteriovenous fistulae range from asymptomatic to high-output heart failure. Renal arteriovenous fistulae are likely to have high flow rates given their proximity to the aorta, thus often will not close spontaneously. Current treatment options for renal arteriovenous fistulae include transcatheter embolization and open ligation of the fistula. This case report describes an adult trauma patient who developed a renal artery to inferior vena cava fistula after a right nephrectomy that was successfully treated with transcatheter embolization. This report adds to the literature on a rare complication following traumatic nephrectomy. Here we review the risk factors, presentation, diagnosis, and treatment of this rare complication.
Case Report
A 20-year-old man presented to the emergency department of a level I trauma center with multiple gunshot wounds to his back. The patient was tachycardic on arrival and received one unit of packed red blood cells in the emergency department. The patient had neurologic deficits below L1 including impaired motor and sensory function distal to his knees. Emergency laparotomy was performed, which was significant for a right zone II retroperitoneal hematoma, right kidney laceration, and segment VII liver laceration. The liver laceration was oversewn, a drain was left along the right retroperitoneum, and an Abthera wound vac was applied. The right retroperitoneal hematoma was not explored. Post-operatively, the patient remained hemodynamically stable; however, he was taken back to the operating room within 7 hours of the original operation because the drain left along the right retroperitoneum was draining bright red blood. Upon return to the operating room, the right zone II retroperitoneal hematoma was explored, which proved difficult. Significant blood loss was encountered upon exploration of the hematoma. A right nephrectomy was performed by mass ligation of the right renal hilum, and an injury to the posterior aspect of the inferior vena cava was repaired primarily. An Abthera wound vac was placed and the patient was transferred back to the ICU. During this second surgery, the patient received 8 units of packed red blood cells, 8 units of fresh frozen plasma, and 1 unit of platelets.
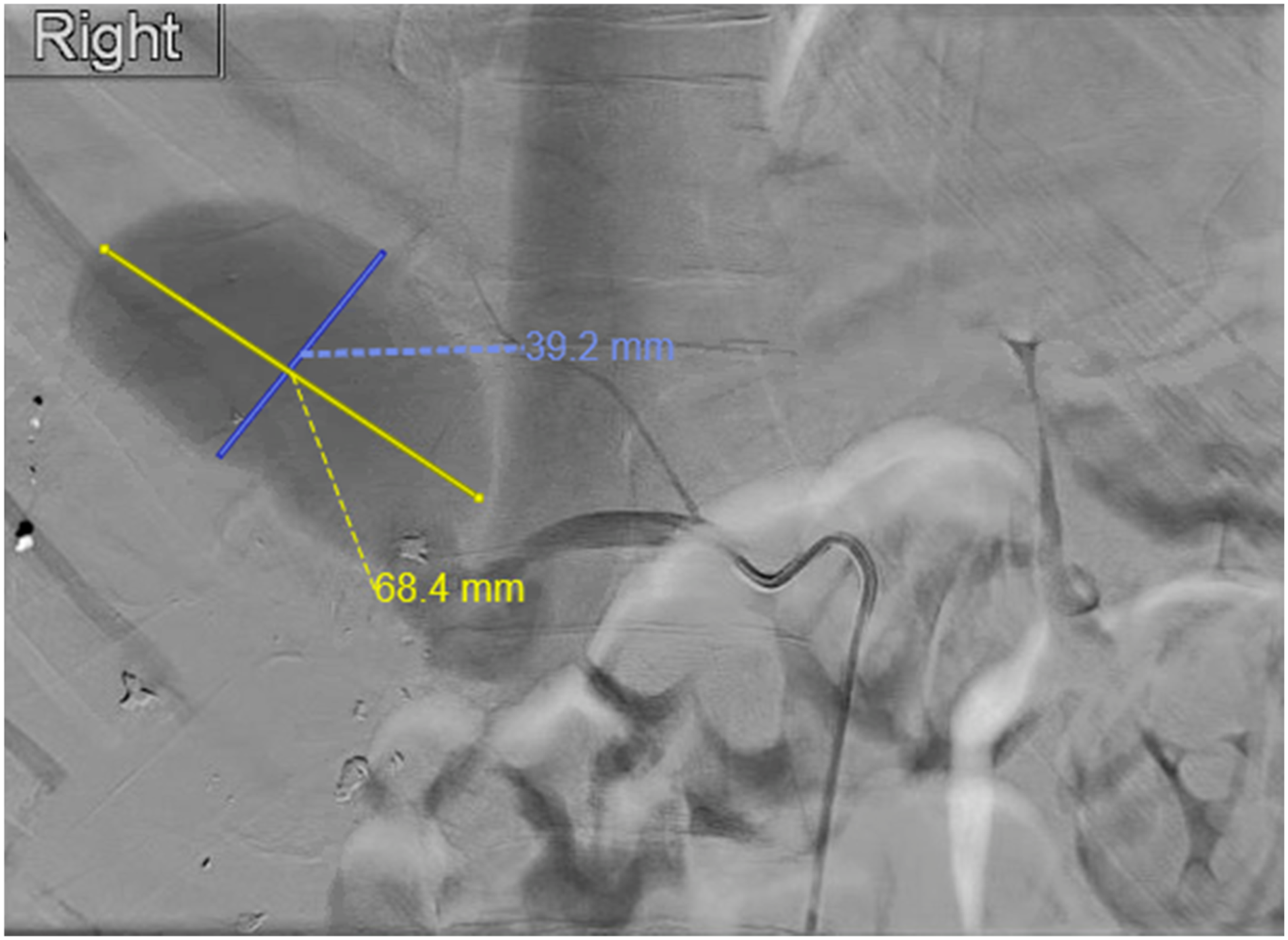
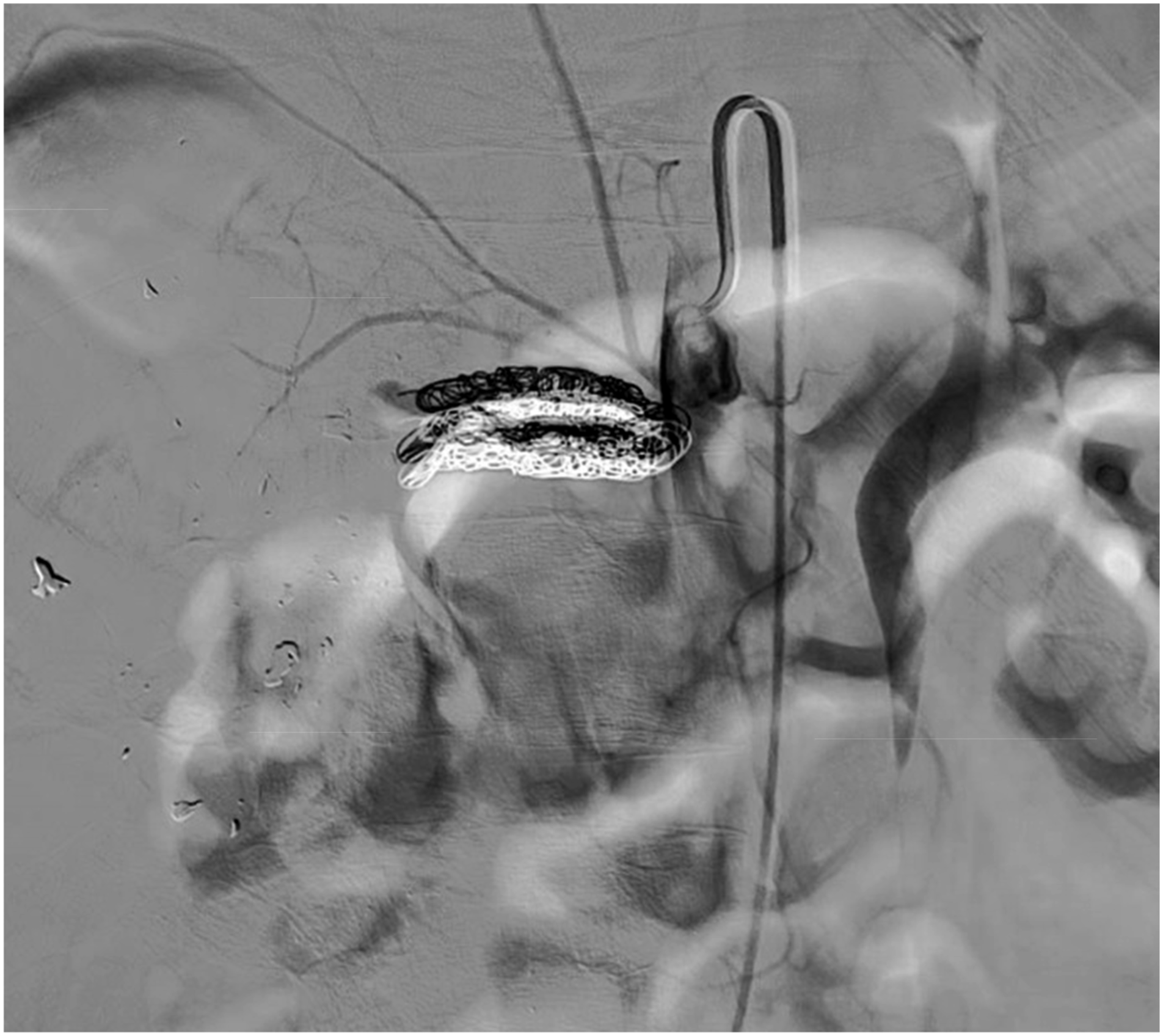
The following day, the patient returned to the operating room where a kocher maneuver was performed to examine the vena cava. No bleeding was noted around the vena cava or the renal artery during this operation and the abdomen was closed. The patient was extubated the following morning and transferred out of the ICU. The post-operative course was complicated persistent leukocytosis, and tachycardia. On post-operative day 9, cross-sectional imaging studies documented the presence of a complex pseudoaneurysm arising from the right renal artery stump (Figure 1). The patient underwent digital subtraction angiography, which revealed a complex vascular injury including a pseudoaneurysm originating from two main branches of the right renal artery and a fistulous communication to the inferior vena cava (Figure 2). The fistula was managed with selective embolization of each renal artery branch (Figure 3) using AZUR hydrogel microcoils (Terumo Medical, Somerset, NJ). The delivery platform used was .018” via a microcatheter. There was no sheath placed in the renal artery, the system as stabilized with an angiographic catheter. A total of five coils were used, two 6 mm diameter coils in the upper renal artery, and three 8 mm diameter coils in the lower renal artery. The length of each coil was 20 cm. Completion angiogram showed successful occlusion of the vascular injury (Figure 4). Post-operatively, the patient was anticoagulated with prophylactic low dose lovenox (40 mg BID subcutaneous injection). The patient had an uneventful recovery after angiography with resolution of palpitations and a normal heart rate. His leukocytosis slowly resolved, and he was subsequently discharged to inpatient rehab five days after embolization. Computed Tomography of abdomen with intravenous contrast showing enhancement of the aorta and the inferior vena cava with fistulous connection at the level of the renal artery. Digital subtraction angiogram demonstrating a complex pseudoaneurysm (measuring 6.8 cm in greatest diameter) arising from the right renal artery communicating with the inferior vena cava. Digital subtraction angiogram demonstrating an accessory renal artery feeding the pseudoaneurysm after the main renal artery had already been embolized. Completion digital subtraction angiogram demonstrating successful closure of the renal arteriovenous fistula by embolizing two branches of the right renal artery.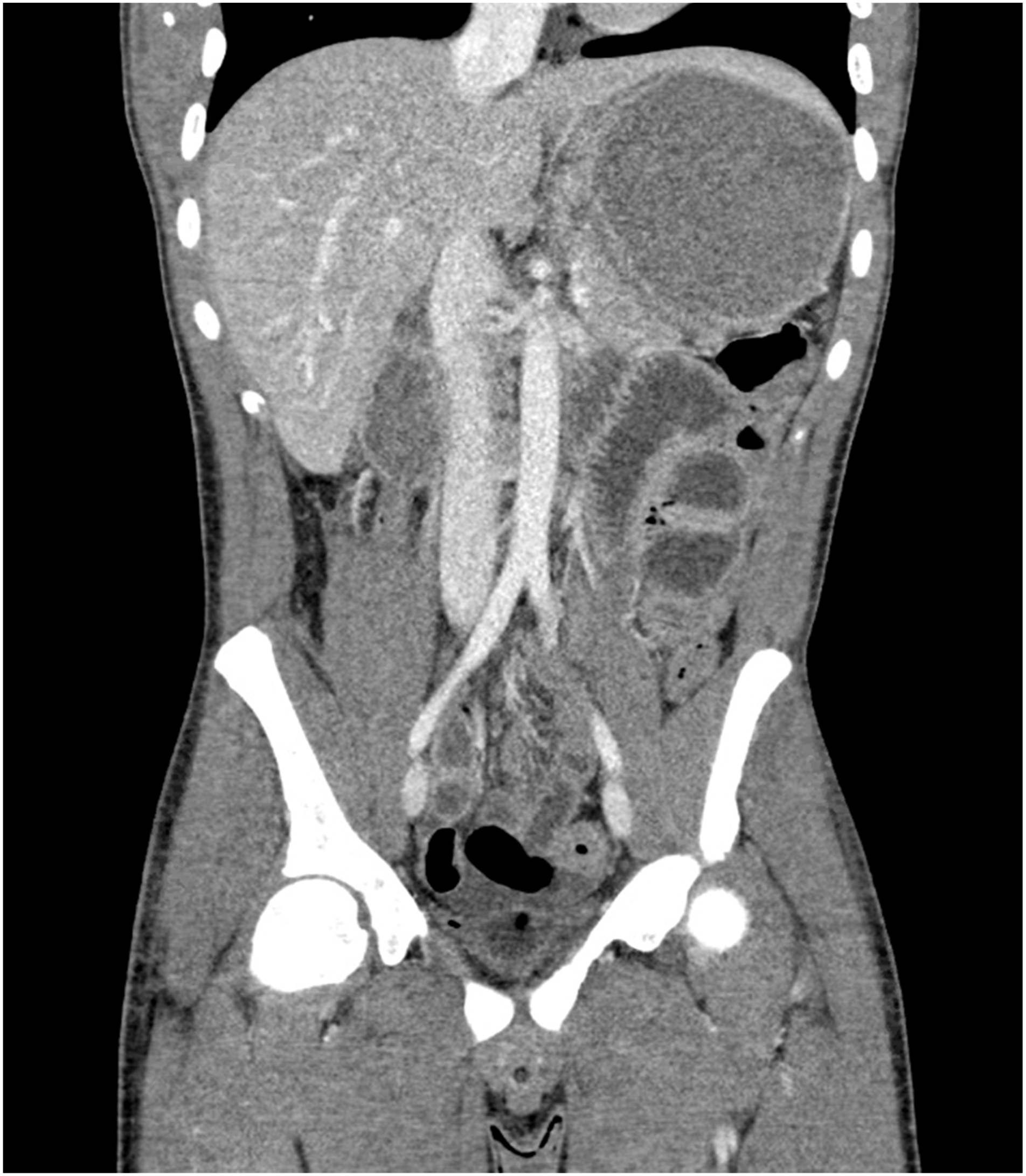

Discussion
Renal arteriovenous fistulae are a rare complication after total nephrectomy. This case illustrates the development of a complex vascular injury after a right nephrectomy. The vascular injury consisted of a large pseudoaneurysm and a high flow fistula from right renal artery to the inferior vena cava. The clinical presentation was tachycardia, palpitations, and leukocytosis. A literature review published in 1997 reported 72 cases, with the first being reported in 1934.6,7 The most recently published literature review reported another twenty-one cases between 1997 and 2019. 4 The reported incidence of renal artery arteriovenous fistula accompanying pseudoaneurysm is less than 1%. 8 This case report adds to the published literature on this rare entity.
The pathophysiology of acquired renal arteriovenous fistulae after nephrectomy is not well understood. A documented risk factor for renal arteriovenous fistulae includes mass ligation of the renal pedicle instead of individual ligation of the renal artery and renal vein. In the case of nephrectomy performed for trauma, the surgeon often does not have the luxury to cleanly dissect the renal artery and vein individually due to significant blood loss. Renal arteriovenous fistulae following trauma preferentially affect the right side. 9 This right-sided predominance is likely due to the longer renal artery on the right, which could promote the formation of an aneurysm at the blind end with subsequent erosion into the vena cava, forming a fistula.
The time from nephrectomy to presentation of renal arteriovenous fistulae can vary from hours to decades later. 10 Presenting signs in the postoperative period can include persistent tachycardia with palpitations and persistent anemia. If the flow rate across the fistula is high, as seen in aortocaval fistula, there is an increase in cardiac output to compensate for the left to right shunt. This process results in high-output heart failure if left untreated, which accounts for the clinical manifestations in many late presenting cases.3,10
Cross-sectional imaging studies are key to the diagnosis of renal arteriovenous fistulae. 11 Digital subtraction angiography is considered the diagnostic gold standard and management of the complications is possible in the same session. Given the high flow rate across renal arteriovenous fistula, treatment is mandatory to either treat or prevent the development of high-output heart failure. Treatment options consist of endovascular therapy and operative surgical repair.
There has been a shift toward endovascular management of renal arteriovenous fistulae.10,12,13 Endovascular repair offers a less morbid treatment option in the high-surgical risk patient. Transcatheter embolization can be used to treat many different arteriovenous fistulae throughout the body and was successfully used to treat a renal arteriovenous fistula in our patient. Operative repair of a renal arteriovenous fistula following nephrectomy would include selective renal artery and renal vein ligation. This operation may require suprarenal aortic clamping to avoid injury to the renal artery or enlarged veins. Care must be taken to identify any accessory renal arteries that may feed the fistula, as seen in our patient who had two dominant branches feeding into the vena cava. This again highlights the value of endovascular therapy, which allows for clear identification of all vessels feeding the fistula, and completion angiogram can document closure of the fistula prior to leaving the operating theater.
Conclusion
Renal arteriovenous fistula following nephrectomy remains a rare entity. This case report adds to the literature another case managed by angioembolization using microcoils. This fistula formed secondary to mass ligation of the renal pedicle with concomitant inferior vena cava injury. This case also highlights the importance of exploring retroperitoneal hematoma’s secondary to penetrating trauma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient provided written consent for the publication of this case report.