
Abstract
Background
Intercostal artery aneurysms (ICA) are rare vascular disease. A rupture of ICA is a possible mechanism of intramural aortic hematoma (IH). We report a case with IH and ICAs without clear etiology.
Keywords
Background
Intramural hematoma (IMH) is a life-threatening aortic pathology included under the term Acute Aortic Syndromes, together with aortic dissection and penetrating aortic ulcer (PAU). IMH is a contained aortic wall hematoma caused by bleeding within the media without initial intimal flap formation. 1
Computed tomography angiography (CTA) can identify high-risk patients with IMH prone to higher morbidity and mortality: Those having IMH with maximum ascending aortic diameter from 48 to 55 mm or descending aortic diameter >41 mm have higher rate of adverse events. Hematoma thickness >11 mm is also predictive of adverse events-independent of the maximum aortic diameter. 2
Differential diagnosis of ICA includes intramural blood pool (IBP) and an ulcer-like projection (ULP) both of them are associated with IH. IBP is defined as a focal contrast-enhancing collection within an intramural hematoma with a narrow or non-discernible communication with the aortic lumen. They are believed to represent blood pooling related to an aortic branch pseudoaneurysm or tear.
While ULP which is a complication of IMH characterized by a new focus of intimal disruption in an area of high shear stress with no underlying atherosclerotic disease.3-5
In the current case, we performed diagnostic selective angiography revealing true intercostal artery aneurysms as they have clear neck, arterial continuation, and appeared after TEVAR placement.
Several predisposing conditions of an intercostal artery aneurysms were described in the literature: Type 1 neurofibromatosis, coarctation of the aorta, Kawasaki Disease, Ehlers-Danlos Syndrome, tuberculosis, mycotic aneurysm, post-trauma or iatrogenic procedures, etc.6-9 Rupture of minor arteria branches, such as the intercostal or bronchial arteries, may represent one mechanism of intramural hemorrhage and subsequent aortic dissection of the distal aorta. 10 Successful embolization of intercostal artery aneurysms were described in literature.11,12
Case Presentation
A 64-year-old man was admitted to our emergency room with sudden onset of acute diffused abdominal and chest pain, radiating to the back. No history of trauma reported.
His past medical history includes hypertension, hyperlipidemia, and an elective endovascular aneurysm repair (EVAR) of abdominal aorta two years earlier. On follow up, a type II endoleak without sac enlargement was observed. Six months prior to the current admission, he presented with acute right leg ischemia due to right limb graft thrombosis without clear etiology. A femoro-femoral bypass with Gortex 8 mm ring left to right was performed. No thoracic pathology was observed upon CTA which was performed.
Vital signs on admission were as follow: blood pressure 136/68, pulse rate 73 bpm, body temperature 36.6 C, and saturation 99% in room air. The physical examination was unremarkable, without pulsatile abdominal mass. Laboratory investigation revealed leukocytosis (WBC = 18.61 K/microL) with neutrophilia (NEUT.abs = 16.88 K/microL), C-reactive protein level (CRP) 1.08 mg/dL, hemoglobin 14.9 g/d, creatinine 1.1 mg/dL, and urea 32 mg/dL.
CTA demonstrated intramural thoracic aortic artery hematoma beginning at the left subclavian artery and extending to the celiac trunk. An already known type II endoleak without sac enlargement was demonstrated, maximal IH thickness diameter of 11 mm, maximal aortic diameter of 40 mm. (Figure 1) CTA images. (A) Sagittal view shows an intramural aortic hematoma; (B and C) Axial view shows intramural aortic hematoma and normal intercostal arteries diameter.
The patient was treated with anti-impulse medical therapy in the intensive care unit.
Blood pressure was successfully controlled and the pain resolved. CTA 48 hours later revealed a stable intramural hematoma and aortic diameter, focal contrast enhancement was observed at T9 level (4 mm) and a new moderate left hemorrhagic pleural effusion.
Due to these findings, thoracic endovascular aortic repair (TEVAR) was performed. (Figure 2). Axial CTA image shows a moderate left hemorrhagic pleural effusion with aT9 intercostal micro artery aneurysm 4 mm.
Since the patient underwent EVAR in the past and in order to reduce risk of paraplegia, we intended to cover less than 20 cm length (above the level of T9) and observe.
TEVAR was performed with a Navion Medtronic stent-graft (40-40-175), distal to left subclavian artery. The procedure was performed under a CSF drainage and an evoked potential monitoring.48-hour follow-up CTA showed an enlargement of T9 focal enhancement to 9 mm and a new T11 focal enhancement, 4 mm.
Intramural hematoma pool is another etiology we considered; it is defined as a focal contrast-enhancing collection within the intramural hematoma. Therefore, we decided to observe and perform another follow-up CTA.
One week later, CTA showed enlargement of the focal enhancement to 11 mm and 8 mm, respectively. (Figure 3) CTA images. (A) axial CTA shows T9 intercostal artery aneurysm; (B) sagittal view of T9intercostal artery aneurysm; (C) axial CTA shows T11 intercostal artery aneurysm.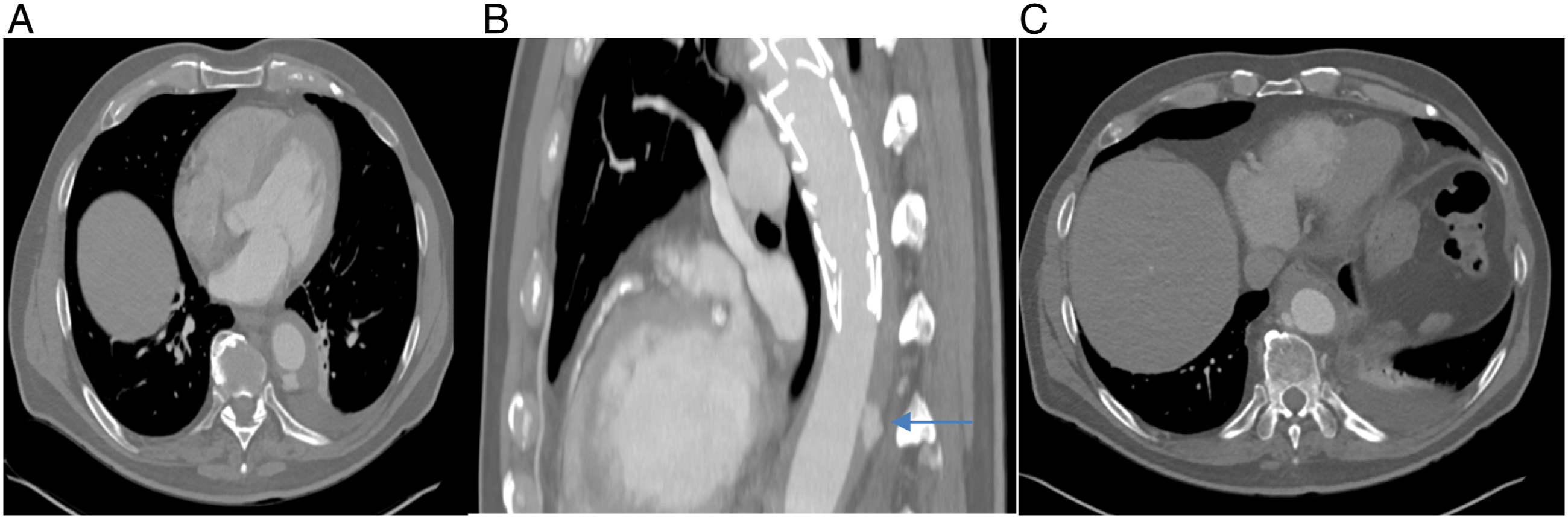
We performed selective angiography via left common femoral artery approach. A connection to both the intercostal artery and the aortic lumen was demonstrated as expected in intercostal artery aneurysm.
We successfully treated the two aneurysms with AXIUM Helix coils (Figure 4) Selective Intercostal angiography. (A) aneurysm of T9 intercostal artery prior to embolization(Afferent artery, aneurysm, and efferent artery). (B) after occlusion with micro coils, and complete exclusion of the aneurysm sac. (C) aneurysm of T11 intercostal artery prior to embolization. (D) after occlusion with micro coils, and complete exclusion of the aneurysm sac.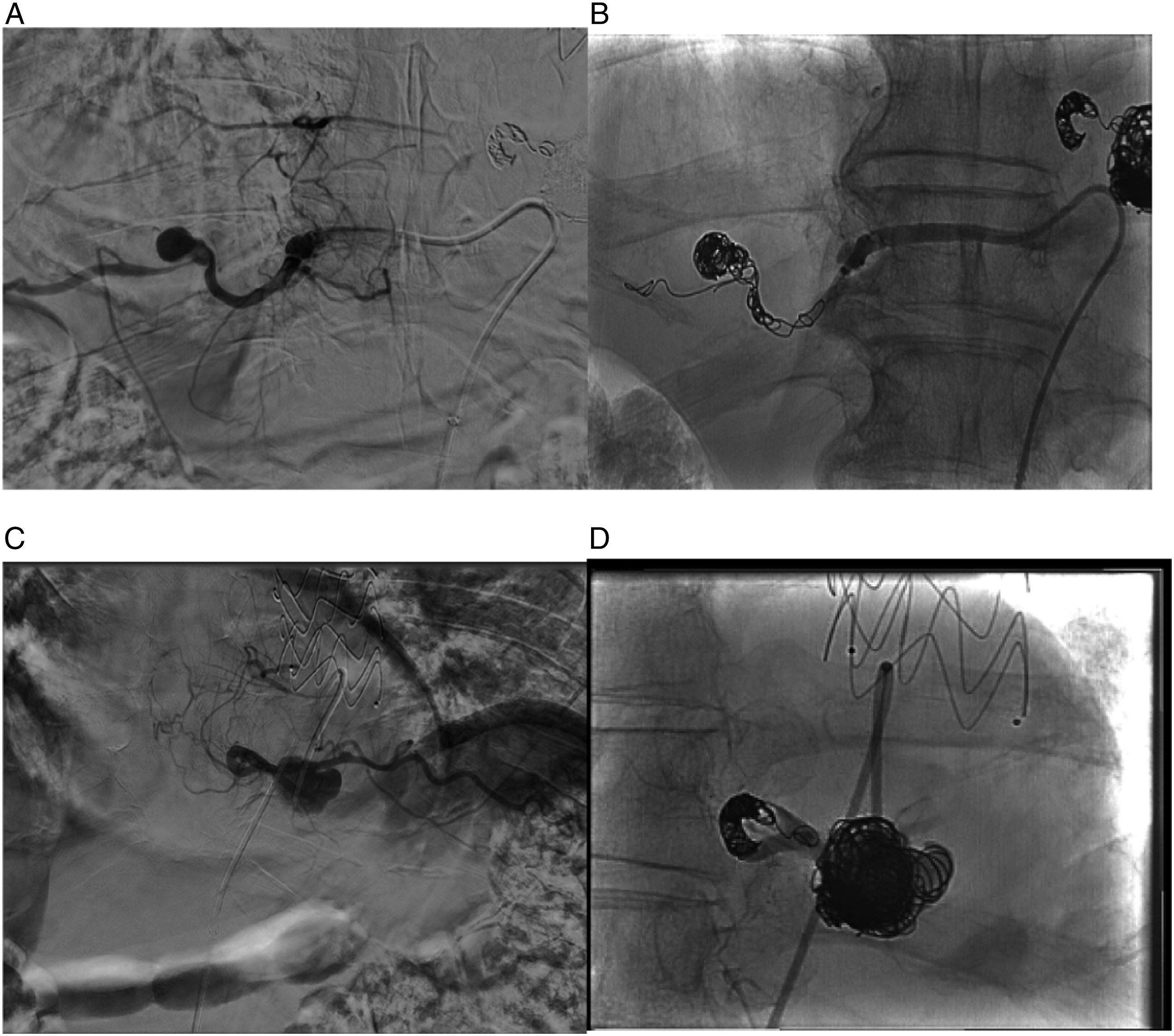
CTA two weeks after the initial presentation demonstrated two new intercostal artery aneurysms at the level of T11 and T12. Embolization with CONCERTO Helix coils was successfully performed. (Figure 5) CTA and selective angiography images. (A and B) T11 intercostal artery aneurysm. (C and D) T12 intercostal artery aneurysm.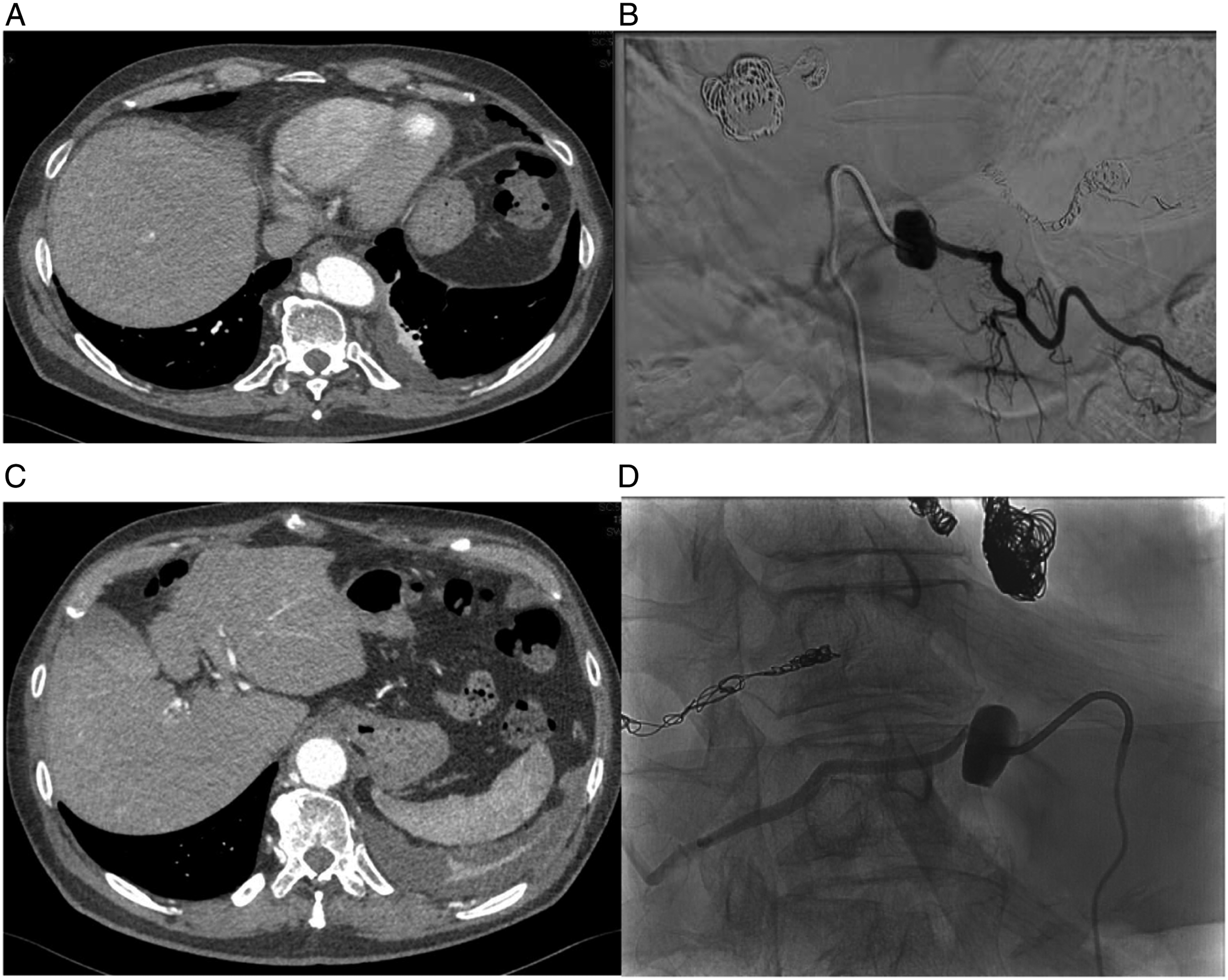
A completion-CTA one week later revealed a favorable aortic remodeling, a reduction of the aortic intramural hematoma size and an obliteration of all four intercostal artery aneurysms.
Three months after discharge, a follow-up-CTA showed a complete resolution of the intramural hematoma and an obliteration of all treated intercostal arteries, without new intercostal artery aneurysms. (Figure 6) CTA images. (A) sagittal view, resolution of the IH; (B) Three-dimensional reconstruction of the thoracic aorta after TEVAR and embolization of 4 intercostal artery aneurysms.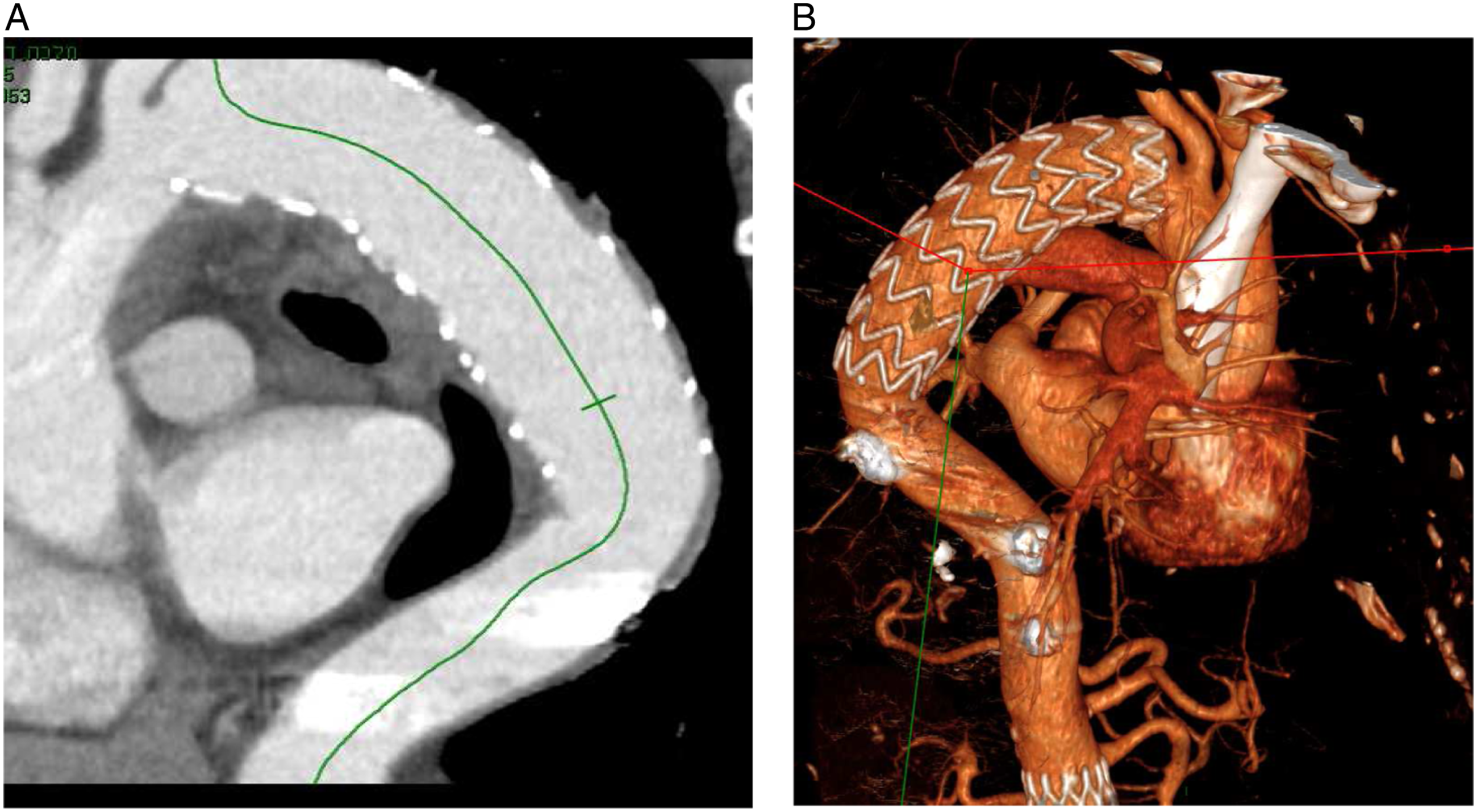
An annual CTA follow up was recommended to rule out an aortic and intercostal disease progression.
Conclusion
This case presents a patient with an IH and ICAs as demonstrated in angiography, in the absence of a clear etiology.
A hemorrhagic left pleural effusion is not an absolute indication for TEVAR; however, the maximal descending aorta diameter was 40 mm and the maximal IH thickness was more than 11 mm. Therefore, we decided to perform TEVAR with short coverage from the LSA and observe clinically and radiologically.
The focal enhancements on follow-up CTA were inconclusive, diagnosis included IBP, ULP, and intercostal artery aneurysms. Due to their diameter increase and the formation of new ones, we performed diagnostic selective angiography that showed true intercostal artery aneurysms.
Optional treatment by extending the TEVAR would both increase the paraplegia risk and will not exclude the retrograde flow to the ICA. Therefore, ICA selective embolization was performed with success.
Although the intercostal micro-aneurysms were not detected initially, lack of ICAs in the initial CTA might be due to the pressure exerted by the hematoma or that they were too small to be detected but continued to grow on follow up.
Rupture of these micro-aneurysms is a possible mechanism of intramural aortic hematoma. On one year CTA follow up, the IH hematoma on the uncovered aorta dissolved, without development of new ICA.
Footnotes
Authors’ contributions
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.