
Abstract
Thoracoabdominal aneurysms pose technical challenges for endovascular repair due to involvement of visceral and renal vessels. We report a case series of four patients diagnosed with thoracoabdominal aneurysm who underwent complex endovascular repair with Fenestrated Device and chimney grafts (FEVARCh). FEVARCh is a technically feasible approach for repair of thoracoabdominal aneurysms that involve renal, superior mesenteric, and celiac arteries for patients not appropriate for open surgical repair. Further studies are needed to understand the implications of resultant Type 1a endoleaks and strategies to minimize the displacement of the main body graft with adjunct chimneys.
Introduction
Thoracoabdominal aortic aneurysms (TAAA) present unique anatomical challenges due to the extent of aneurysmal disease and involvement of the visceral and renal arteries. While endovascular repair for abdominal aortic aneurysms (EVAR) and thoracic aortic aneurysms (TEVAR) has become common practice, an open approach is still considered gold standard for TAAA. In 2010, Greenberg et al. described a reinforced fenestrated EVAR technique for thoracoabdominal aortic aneurysms; however, it was not until 2012, after the approval from the Food and Drug Administration, that the Zenith Fenestrated endograft platform (ZFEN; Cook Medical, Bloomington, Ind) became widely available.1,2 Greenberg et al. 3 introduced the chimney graft technique in 2003 where a covered stent is deployed parallel to the main aortic stent-graft with the intent to extend the proximal seal zone in short-neck aneurysms and maintain renal patency using bare-metal stents. Complex endovascular repair of TAAA has been traditionally categorized into fenestrated endovascular aneurysm repair (FEVAR) or debranching of the renal and visceral arteries with chimney followed by a standard EVAR. 4 Fenestrated devices theoretically allow for a more physiological deployment of additional grafts and minimize the risk of microembolization to the renal arteries in patients with preexisting thrombus. 5 The limitation of fenestrated grafts is there is a maximum of two fenestrations and a single scallop. Chimney grafts have the benefit of extending proximal landing zones and is immediately available off-the shelf. 6 A combined approach enables providers to treat complex TAAA that would have been otherwise not amenable to an endovascular repair. Here we present a four patient case series describing repair of TAAA using FDA-approved Zenith Fenestrated graft combined with a chimney graft approach (FEVARCh).
Case Series
Patient 1
A 73-year-old man with a past medical history of pulmonary hypertension presented to clinic for management of an asymptomatic 5.4 × 5.2 cm descending thoracic aortic aneurysm and 5.6 × 5.8 cm abdominal aneurysm involving the celiac, superior mesenteric and renal arteries, and bilateral iliac aneurysms (Figure 1A). A planned staged approach was recommended due to the extent of aortic treatment that was required. A spinal drain was placed prior to FEVARCh to lower the risk of spinal cord ischemia. He underwent a TEVAR (Figure 1B) followed by repair with thoracic endoprosthesis along with fenestrated graft in combination with a right renal artery chimney, stenting of superior mesenteric artery and left renal artery as part of the fenestrated repair. Because of the limitations of the design of the custom stent-graft and the need for additional seal zone, only one renal artery is incorporated in the repair. There was exclusion of the aneurysm sac with a small amount of contrast at the renal gutter at the conclusion of the case (Figure 1C). Surveillance imaging revealed a type 2 endoleak arising from covered celiac artery. After a failed attempt by Interventional Radiology at embolization, he underwent laparoscopic ligation of the proximal celiac artery and accessory hepatic artery. He recovered well from the operation. Follow up CTA demonstrated persistent type IA gutter endoleak with outflow via the celiac axis. Interventional Radiology was consulted for trans-lumbar approach at celiac artery embolization. Repeat CTA showed no endoleak. (A) Descending thoracic aortic aneurysm measuring 5.4 × 5.2 cm, abdominal aneurysm measuring 5.6 × 5.8 cm. (B) TEVAR deployment. (C) Zenith fenestrated graft with right renal artery chimney, SMA and left renal artery stent.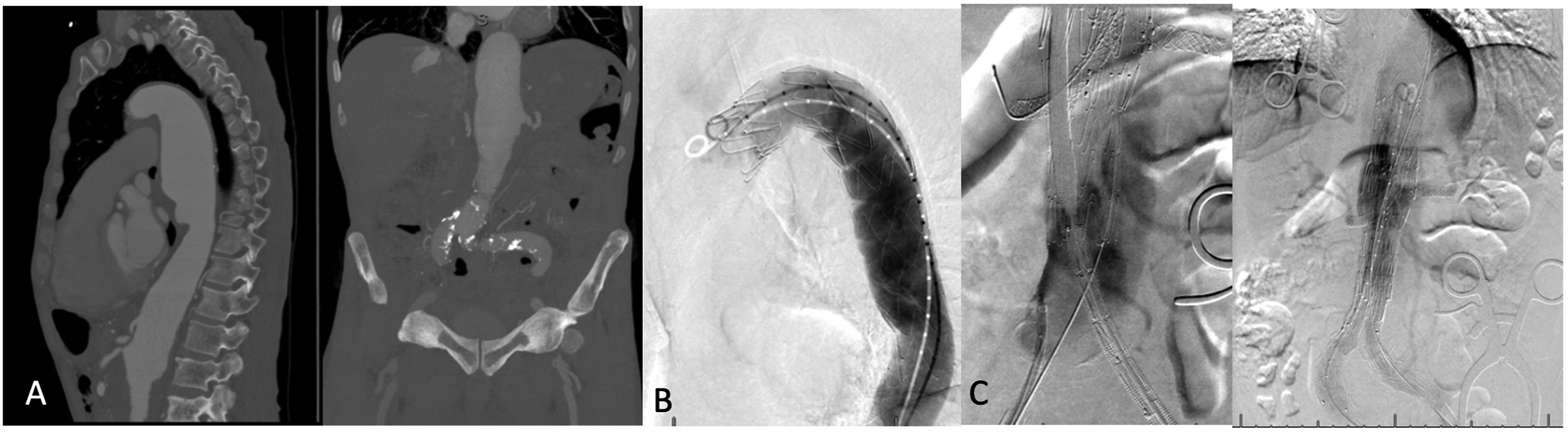
Patient 2
88-year-old woman with a past medical history of hypertension was followed in clinic for a known paravisceral, asymptomatic abdominal aortic aneurysm. Over six months, the aneurysm had significant interval growth from 3.4 cm to 4.8 cm (Figure 2A). She underwent repair with a fenestrated graft with stenting of superior mesenteric artery and left renal artery. The right renal artery was included as a chimney graft to gain as much length as possible. The celiac artery was treated with an unstented, large fenestration. After selective cannulation and placement of stents, the paravisceral aneurysm was nicely excluded without evidence of an endoleak and termination above bilateral hypogastric arteries (Figure 2B). She recovered well from the operation. (A) Abdominal aneurysm measuring 4.8 cm. (B) Zeneth fenestrated graft with chimney of right renal artery, SMA and left renal artery stenting.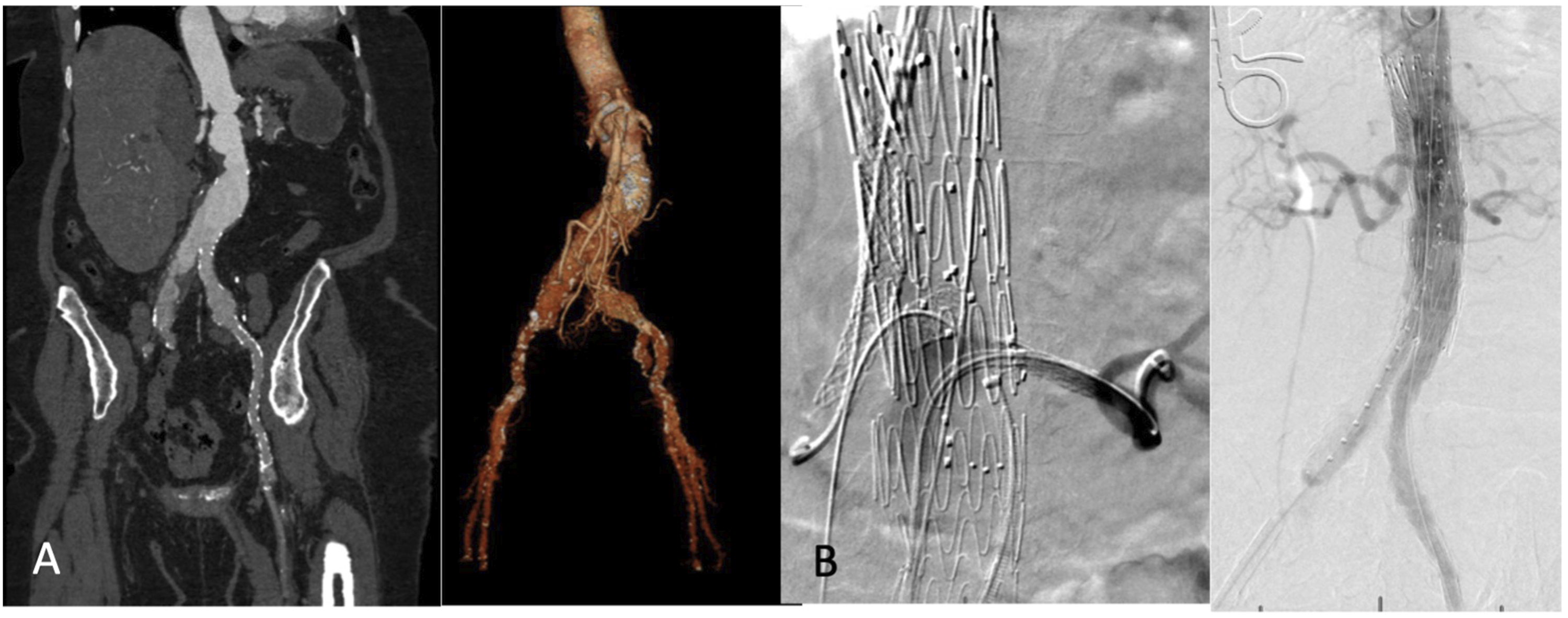
Follow up CTA demonstrated small type 2 endoleak at the level of inferior mesenteric artery. Duplex surveillance over the next year revealed resolution of endoleak and patent superior mesenteric and renal arteries.
Patient 3
71-year-old man with a past medical history of hypertension and tobacco use presented to clinic for an incidentally discovered saccular aneurysm of the posterior wall of the abdominal aorta measuring 4.7 × 4.2 × 3.0 cm near the superior mesenteric artery (Figure 3A). He underwent repair with a fenestrated endovascular device with stenting of the right renal and superior mesenteric arteries and chimney stenting of the left renal artery. The celiac artery was treated with unstented, large fenestration. At the conclusion of the case, there was widely patent visceral vessels and no evidence of endoleak (Figure 3B). He recovered well from the operation. Follow up CTA revealed patent vessels and no endoleak. (A) Abdominal aorta measuring 4.7 × 4.2 × 3.0 cm. (B) Zenith fenestrated repair with chimney and stenting of left renal artery and stenting of right renal and SMA.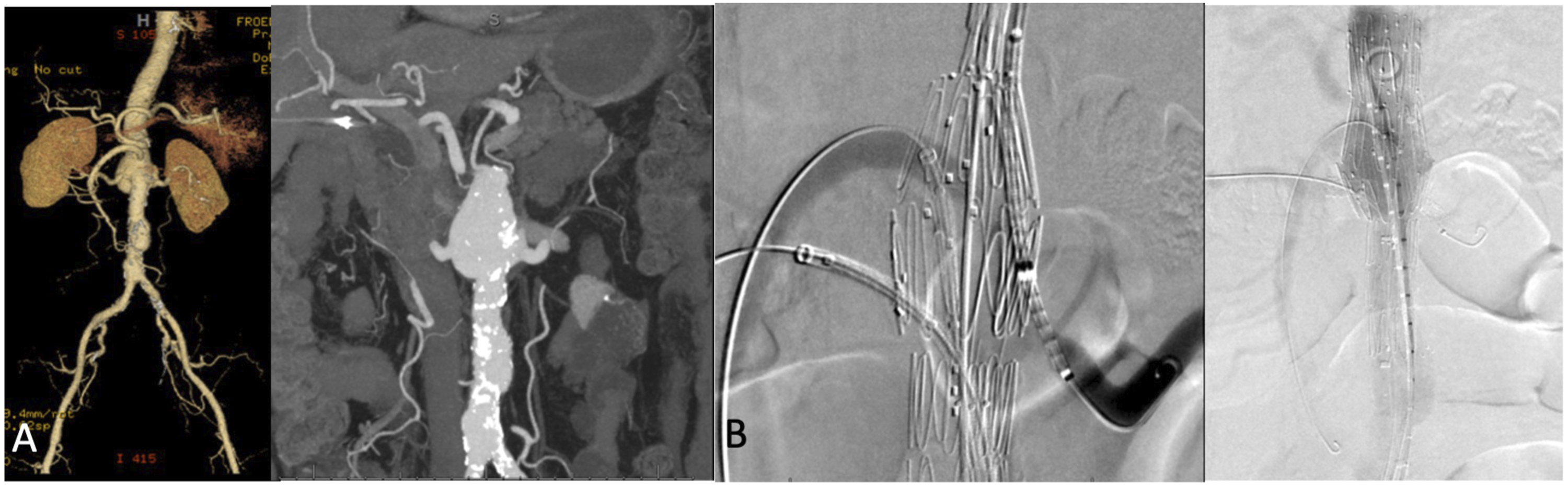
Patient 4
66-year-old man with a history of coronary artery disease, chronic kidney disease, and obesity was seen clinic for an incidentally discovered type II TAAA (Figure 4A). He underwent a staged approach with TEVAR followed by FEVARCh. He required a left carotid artery to subclavian artery bypass initially to gain an appropriate seal zone for the thoracic endograft. Twenty fourhours later, he underwent the planned TEVAR with coverage of the left subclavian artery (Figure 4B). Four months later, he underwent repair of the pararenal abdominal aortic aneurysm with placement of a fenestrated endovascular device that involved stenting of the superior mesenteric artery and the left renal artery, and chimney balloon-expandable Viabahn stent to the right renal artery. All visceral vessels and both hypogastrics remained patent (Figure 4C). Surveillance imaging the following year revealed type 2 endoleak arising from left subclavian artery. He underwent endovascular embolization with coiling of the proximal portion of the left subclavian artery. He recovered well from the operation. Follow up CTA demonstrated stable aneurysm sac at 4.1x4.5 cm, patent vessels, and no evidence of endoleak after two years. (A) Abdominal aortic aneurysm measuring 6.1 × 6.0 cm. (B) TEVAR deployment following left carotid artery to subclavian bypass. (C) Zeneth fenestrated repair with stenting of SMA and left renal artery with chimney of right renal artery.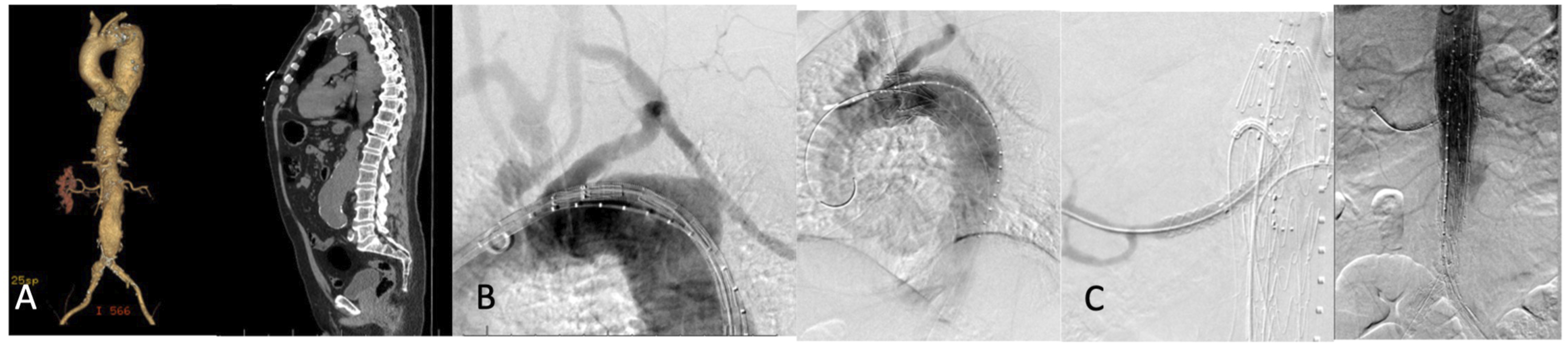
Discussion
Thoracoabdominal aneurysms have traditionally been repaired with an open approach given the challenges of mesenteric and renal vessel preservation. However, open repairs carry significant morbidity and mortality, with peri-operative mortality rates in large series at 13%. 7 Endovascular approaches provide a less invasive option, but data remains limited in a superior surgical approach. In addition, there is no commercially approved devices in the United States to treat this patient population. FEVAR and chimney EVAR success is based on maintaining branch vessel patency, preservation of renal function, and appropriate aneurysmal exclusion. Comparison of the two approaches shows similar outcomes with FEVAR having numerically improved but not statistically significant 30-day mortality (2.4%vs5.3%) and renal dysfunction (9.8%vs12%).6,7 However, given the current design restraints of ZFEN, two thirds of complex AAA are not amenable to fenestrated repair. ZFEN currently allows three custom modifications to the main body consisting of scallops and fenestrations ranging from small to large with only small fenestrations and scallops amenable to visceral stent placement.8,9 Adjunct chimney placement becomes ideal for patients with closely spaced visceral arteries, short abdominal aortas, or aneurysms which require coverage of the renal, superior mesenteric, and celiac arteries. 10 Another benefit of FEVARCh is ability of the main body to anchor to the native aorta via the visceral fenestrations which is not achieved with chimney followed by EVAR. Complete elimination of migration was shown in one institutions study of greater than 100 ZFEN. 11 We have specifically designed the FEVARCh approach to extend the proximal seal zone on the aorta to attempt to minimize the gutter leak.
Two of the four patients discussed in this report had small type 1A endoleaks at the conclusion of the case. These types of “gutter” leaks are the result of main body graft displacement due to additional revascularization of the visceral vessels. Wang et al. 9 reported technical success in 6 patients undergoing ZFEN with chimney into visceral arteries (three renal, two celiac, and one accessory renal) with 2 patients having type IA “gutter” endoleaks. Another 6 patient case series reported similar results for three suprarenal aneurysms and three thoracoabdominal aneurysms. One patient in that study developed type 1A “gutter” leak. 12 Long term outcome data is missing on the significance of these leaks; however, on recent study by Ullery et al. 13 demonstrated spontaneous resolution 44.3%, 65.2%, and 88.4% of patients with “gutter” leaks at 6, 12, and 18 months post-operatively. Additional strategies to minimize “gutters” include limiting chimney size in order to produce an adequate seal and preemptively coil the celiac artery which was needed post-operatively for Patient 1. 14
FEVARCh is a technically feasible option for complex thoracoabdominal aneurysms. There were no incidences of paraplegia in our case series. This approach allows the use of only one parallel graft to minimize the risk of gutter leak. Type 1 endoleaks or “gutter” leaks are commonly described in the literature and were present within our series. Initial data suggests that these endoleaks can undergo spontaneous resolution. Long term data and larger series are required to determine outcomes of this approach.
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R.M has been paid consulting fees by Endospan, Medtronic, and W.L. Gore & Associates.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Informed consent has been obtained from the patient (or patient’s family/guardian) or through prior IRB approval through the Aortic Center for publication of the case report and accompanying images.