
Abstract
Objective
This study aims to describe the results achieved in the management of rectus sheath hematoma (RSH) using glue embolization.
Method
Data about all consecutive patients presenting with RSH, between January 2005 and December 2020 were retrospectively reviewed. RSHs were classified according to the Berna CT scan Classification. Clinical and technical outcomes were evaluated during in-hospital period and 1-month follow-up.
Results
Among 74 patients presenting with RSH, CTA revealed an active bleeding in 61 (n = 42, 69% women; median age = 68.8 y range: 47-91). 19 cases of type 1 RSH (25.7%), under anticoagulation therapy and hemodynamically stable, were successfully managed conservatively. Conversely, endovascular embolization with cyanoacrylate glue diluted with ethiodized oil (Lipiodol Ultrafluid, Guerbet, France) was needed in n = 42 (56.8%) patients, in 16 cases after failure of conservative management; a single session of percutaneous glue embolization was adequate to achieve technical and clinical success in all patients with stabilization or progressive improvement of hemoglobin values after procedure (7.1 + 1.8 g/dL pre-procedure vs 11.1 + 1.6 g/dL post-procedure). No major complications occurred. Two minor complications were reported: 1 case (2.4%) of puncture site-related complication (local self-limiting hematoma) and 1 case (2.4%) of post-embolization syndrome (abdominal pain) spontaneously regressive. The median hospital stay was 7 d. At 30-day follow-up, 2 patients (2.7%) died of multiorgan failure.
Conclusions
In the management of RSH, glue embolization was shown to be safe and efficacious. Glue allowed the immediate occlusion of both the “front and back doors” of bleeding without the need to reach the bleeding point, preventing potentially life-threatening recurrence.
Introduction
Rectus sheath hematoma (RSH) is a rare clinical entity whit an incidence of 1.2-1.5 cases per year among patients undergoing imaging for acute abdominal pain and an associated mortality close to 4%. 1
RSH is usually localized between the anterior and posterior sheath of the rectus abdominis muscle and occurs secondarily to a direct tear of the rectus muscle or a laceration of either the superior or inferior epigastric vessels. This vascular injury may occur spontaneously and most frequently in patients receiving anticoagulation therapy or may be associated with a direct blunt or penetrating muscular trauma. Other risk factors are female gender, older age, hypertension, collagen vascular disorders surgery, intense contractions or severe coughing, pregnancy, and primitive coagulation disorders. 2
Early recognition is pivotal to reduce potential complications, and computed angiotomography (CTA) always led to a correct and early diagnosis of active hemorrhage.
Bleeding is usually self-limiting when anticoagulation is stopped and/or reversed. However sometimes, persistent bleeding despite interrupting medical therapy requires interventional management. 3
If surgery plays a limited role in the management of RSH, because it is indicated in cases of abdominal compartment syndrome after failure of the interventional treatment, 4 the endovascular approach with transcatheter arterial embolization (TAE) is currently considered the first-line therapy. 5 Vascular occlusion may be performed using multiple embolic agents, such as particles, gelatin sponge, and coils. The use of glue is less frequently reported.
In this setting, in this paper, we describe the results achieved in RSH management by glue embolization in a single institution (“Santissima Annunziata Hospital” in Taranto, Italy) between January 2005 and December 2020.
Methods
Data Collection, Population, and Study Design
This study was conducted retrospectively, revising data from clinical and radiology records. It is not classified as research requiring formal ethics approval by the local ethics committee according to the Italian regulatory system. 6 Written informed consent was obtained from the patients for publication of their clinical data and accompanying images, and all data were anonymized.
We collected data about anticoagulant therapies, history of trauma, or other predisposing conditions (abdominal procedures, severe coughing, strenuous exercise, and hematologic disorders).
Before the procedure, all patients underwent clinical evaluation and the diagnosis of RSH was made by CTA in all cases.
All RSHs were classified according to the Berna CT scan Classification by 2 expert radiologists
7
(Figure 1). Types of RSH classified according to the by Berna et al. CTA classification. (A) The hematoma is unilateral and confined to the muscle (type 1). (B) The hematoma is set between the muscle and the fascia transversalis (type 2). (C) The hematoma extends into the Retzius space and the peritoneal space (type 3).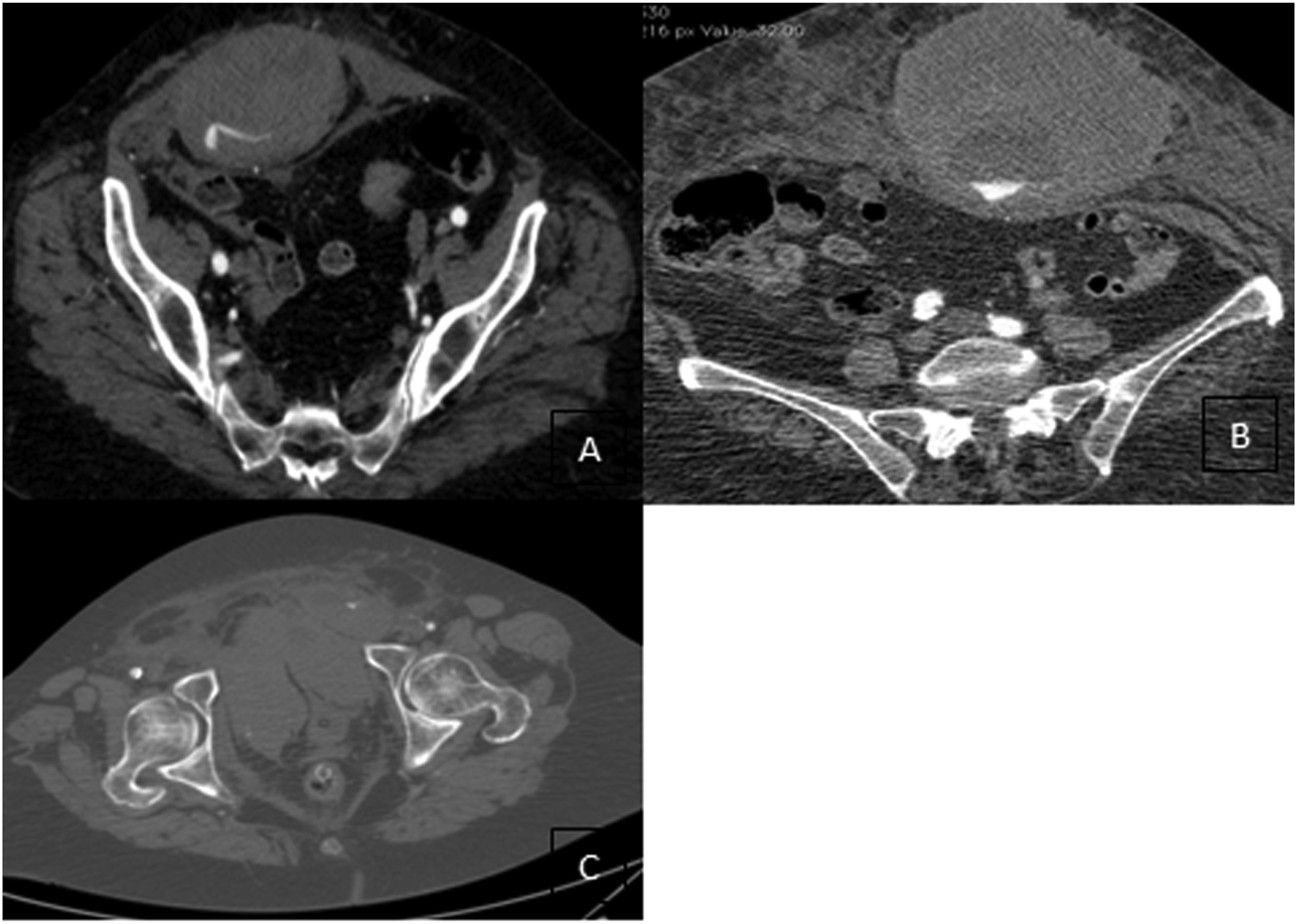
Indication for Treatment
Since 2005, we have developed a protocol to manage patients affected with RSH at our institution.
All patients presenting with Berna type 1 or 2 RSH and on anticoagulation therapies are managed conservatively if hemodynamically stable. Conservative management consists in reversal of anticoagulation, analgesia, rest and blood transfusions, or fluid resuscitation when needed.
Conversely, indications for endovascular treatment include: - hemodynamic instability with clear signs of shock, hypotension, and tachycardia; - persistent bleeding with a decrease in hemoglobin value of > 2 g/dL after at least 3 h from the first test, despite reversal therapies; - Berna type 3 RSH with active contrast extravasation at preoperative CTA; and - bleeding following trauma or iatrogenic injuries.
Outcomes Measurement
The primary outcome was the rate of clinical and technical success achieved immediately after the procedure. Clinical outcomes were evaluated during the in-hospital period.
Clinical success was evaluated in terms of total control of bleeding stabilization of the vital signs, as well as improvement in the hemoglobin, of the patients and no further requirement for blood transfusion. The hemoglobin was checked at 3, 6, and 24 h after the procedure.
Technical success was defined as the achievement of the complete occlusion of the injured vessel with cessation of active hemorrhage/embolization of injured vessel at the completion angiography.
Secondary outcomes included the rates of major complications (procedure-related mortality and non-target embolization with distal ischemia)
Minor complications including post-embolization syndrome, the intervention site (local hematomas/bleeding/pseudoaneurysm formation), or procedural complications (catheter trapping) were also collected.
Procedural Details
Embolization procedure was performed by three consultant interventional radiologist using a coaxial microcatheter technique.
By the means of a .35″ hydrophilic guide wire (Radiofocus, Terumo Inc, Japan) and a Cobra or J-curve guiding catheter (Cook Inc, USA), the vessel of interest was cannulated under fluoroscopy guidance. The arteriogram was thus performed by injecting 8 mL of iodinated contrast material at the rate of 4 mL/s. Then, a 2.7-Fr Progreat microcatheter (Terumo Inc, Japan) was used to super-selectively access the target artery.
In case of bleeding from the inferior epigastric artery, we performed a contralateral 6-French common femoral arterial puncture. After using the crossover technique, the external iliac artery was selectively catheterized and subsequently, the inferior epigastric artery.
For each procedure, inferior epigastric artery microcatheterization was performed to interrupt bleeding. If microcatheterization of the vessel was impossible to achieve or unsuccessful, proximal positioning of the microcatheter in the main vessel was preferred.
In case of bleeding from the superior epigastric artery, a right common femoral approach was performed and the microcatheter was positioned as close as possible to the bleeding point.
Embolizations were performed using different dilutions, particularly from 1:2 to 1:5 glue (Glubran2, GEM, Viareggio, Italy) diluted with ethiodized oil (LUF—Lipiodol Ultrafluid—Guerbet—France), according to microcatheter closeness to bleeding and operator experience.
The endpoint of embolization was reflux of glue and lipiodol into the bleeding point at fluoroscopic control.
Statistical Analysis
Data were collected in a computer database and analyzed with statistical software (IBM SPSS Statistics 22, 2017). The data are reported in percentages and absolute values. Continuous variables are expressed in the mean or in the median of the values obtained.
Results
During the study period, a total of 74 patients presented with RSH at our department. Hematomas were spontaneous (n = 58, 78%), post-traumatic (n = 14, 18.9%), or of an unknown origin (n = 2, 2.7%).
Thirteen (17.6%) patients without active bleeding and medically managed were not considered for further analysis.
Conversely, in n = 61 (n = 42, 69% women; median age = 68.8 y; range: 47-91) cases, the CTA revealed an active bleeding. The most common clinical presentations were intense abdominal pain and an abdominal mass (n = 58, 95%), hypotension (n = 33, 54.1%), and persistent drop of hemoglobin (n = 26, 42.6%).
Preoperative and Operative Data.
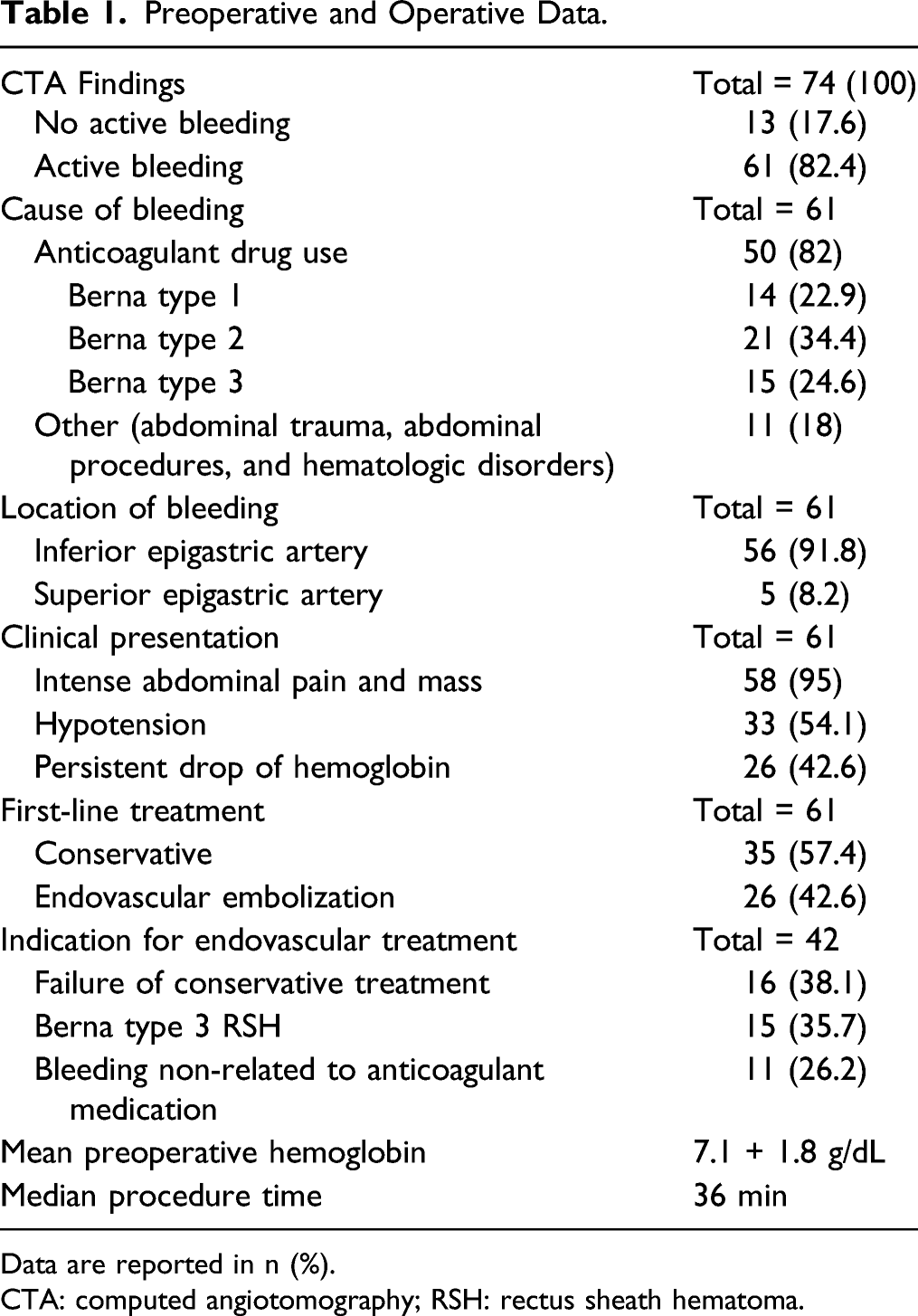
Data are reported in n (%).
CTA: computed angiotomography; RSH: rectus sheath hematoma.
The management strategy adopted in the population in analysis is reported in Figure 2. Management strategy in the population in analysis.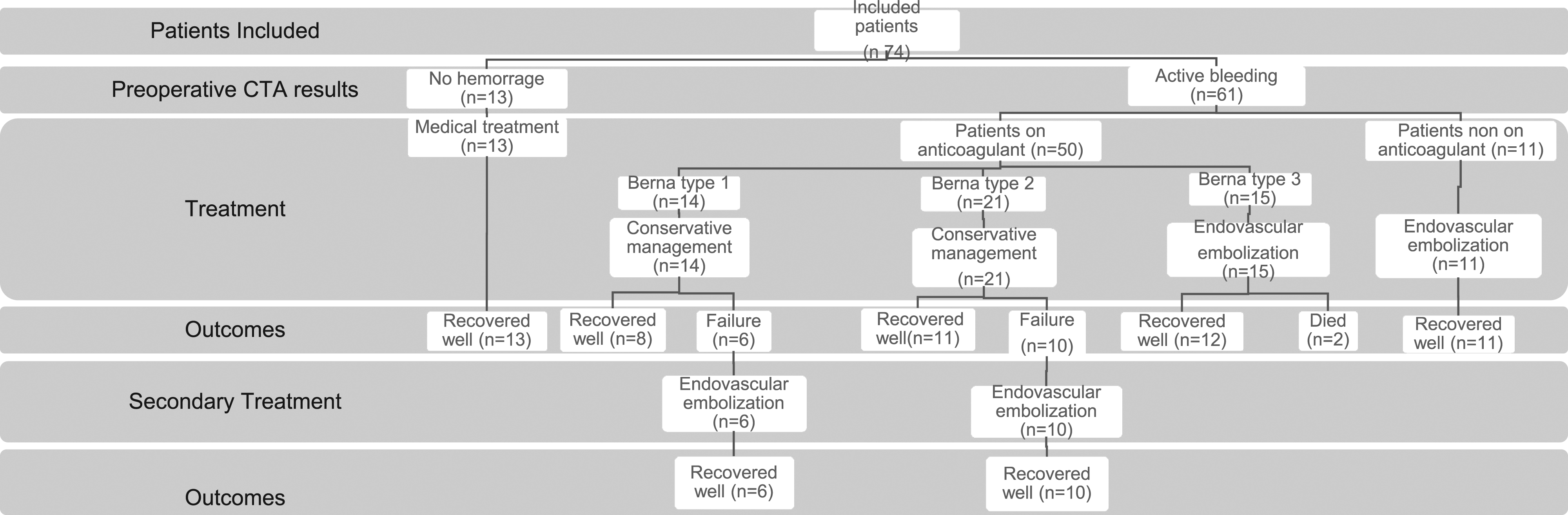
Patients under anticoagulant were classified as Berna type 1 in n = 14 (22.9%) cases, as Berna type 2 in n = 21 (34.4%) cases, and as Berna type 3 in n = 15 (24.6%). According to the protocol previously reported, n = 35 (57.4%) patients classified as RSH Berna type 1-2 underwent conservative treatment that was successful in n = 19 cases (Figure 3). CTA illustrating a Berna type 2 spontaneous and self-limiting RSH. (A) Patient 1. Arterial and delayed phase. (B) Patient 2. Arterial and delayed phase.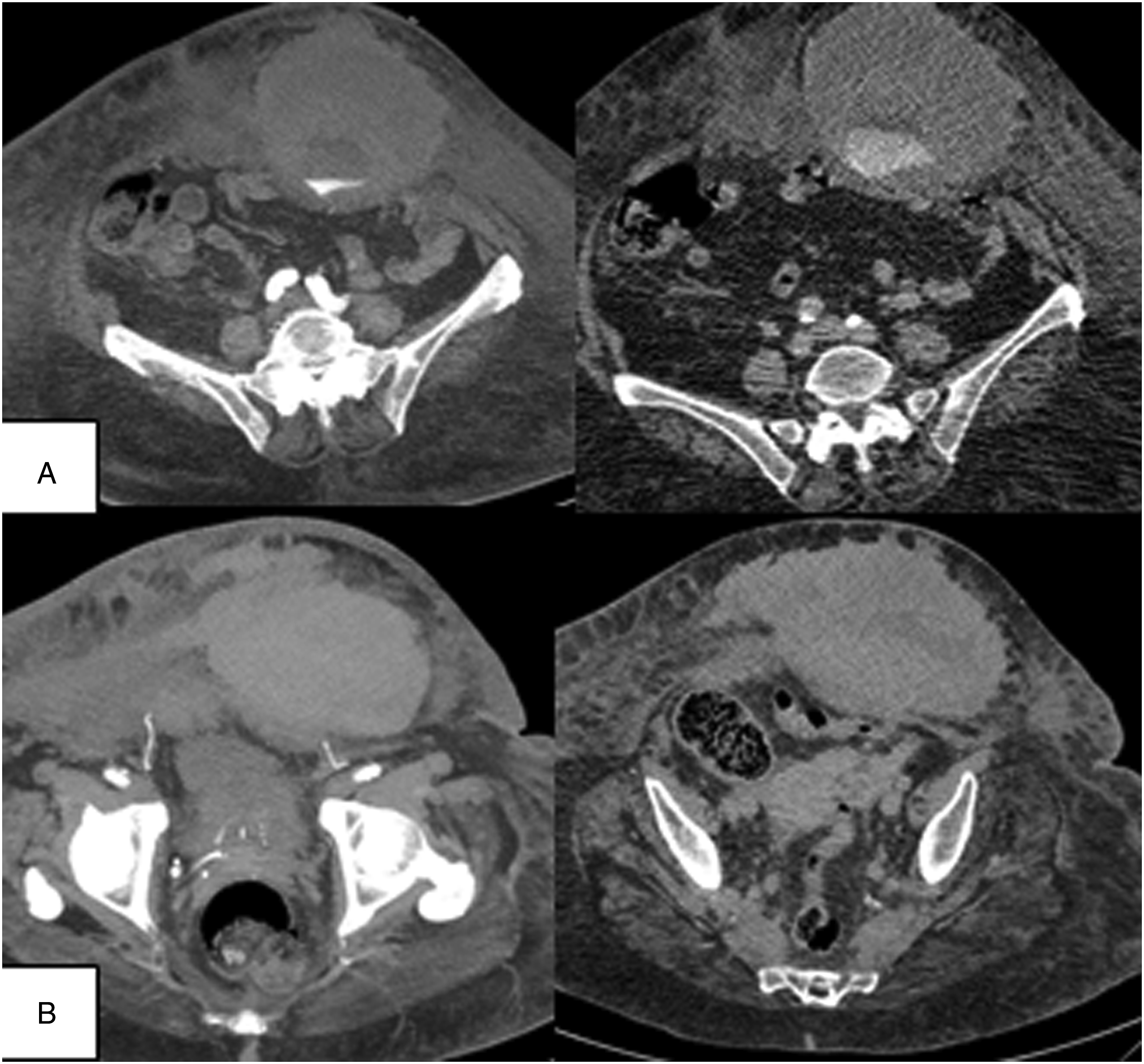
Outcomes Achieve in Actively Bleeding Patients and Complications.
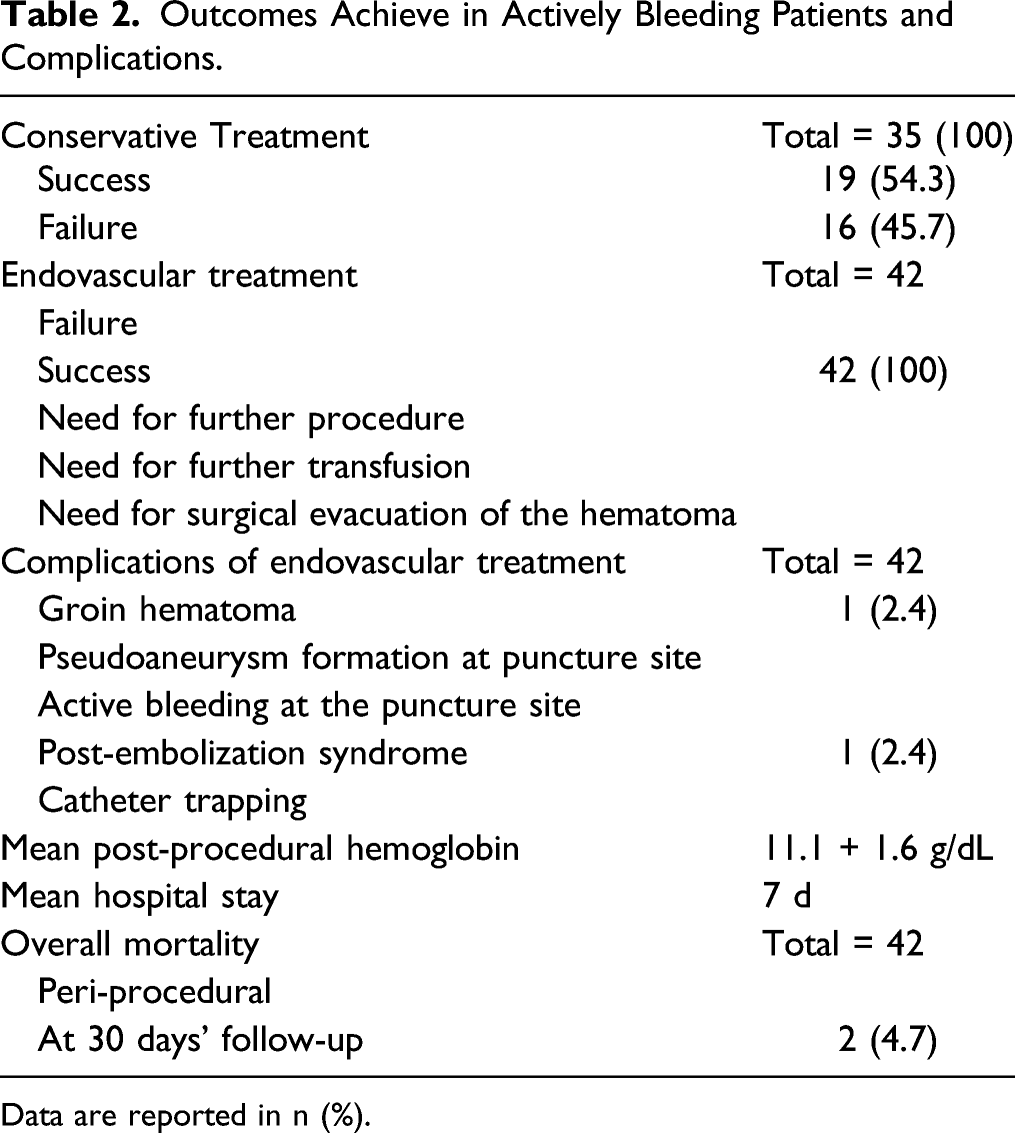
Data are reported in n (%).
The decision to perform the interventional procedure in patients who had failure of conservative management was undertaken according to the hemoglobin levels and after the diagnosis of active bleeding at the CTA. During wait and see management, the procedure was performed at a mean of 6 hours after the initial diagnosis (range: 3-24).
Embolization was technically successful in all cases without any post-treatment arterial bleeding at the completion arteriography (Figures 4 and 5). Median procedure time was 36 min. After the procedure, there was no need for additional transfusion; none of the patients presented new hemorrhages or required more than 1 session of TAE. Hemoglobin levels increased in all cases after the embolization (7.1 + 1.8 g/dL pre-procedure vs 11.1 + 1.6 g/dL post-procedure). CTA illustrating a Berna type 3 RSH. (A and B) The CTA confirms bleeding from the inferior epigastric artery. (C and D) Maximum intensity projection (MIP) and multiplanar reconstruction (MPR) post-processing imaging. (E) The angiography shows bleeding from a small feeding vessel of the inferior epigastric artery. (F) The glue embolization (glue:lipiodol = 1:4 dilution) allows to occlude the feeding vessel and the inferior epigastric artery in one shot. (G) The completion angiogram does not show any residual bleeding. CTA illustrating a Berna type 3 RSH. (A) The CTA confirms bleeding from the inferior epigastric artery. (B) The angiography shows bleeding from a small feeding vessel of the inferior epigastric artery. (C) The glue embolization (glue:lipiodol = 1:5 dilution) allows to occlude the feeding vessel and the inferior epigastric artery in one shot. (D) The completion angiogram does not show any residual bleeding.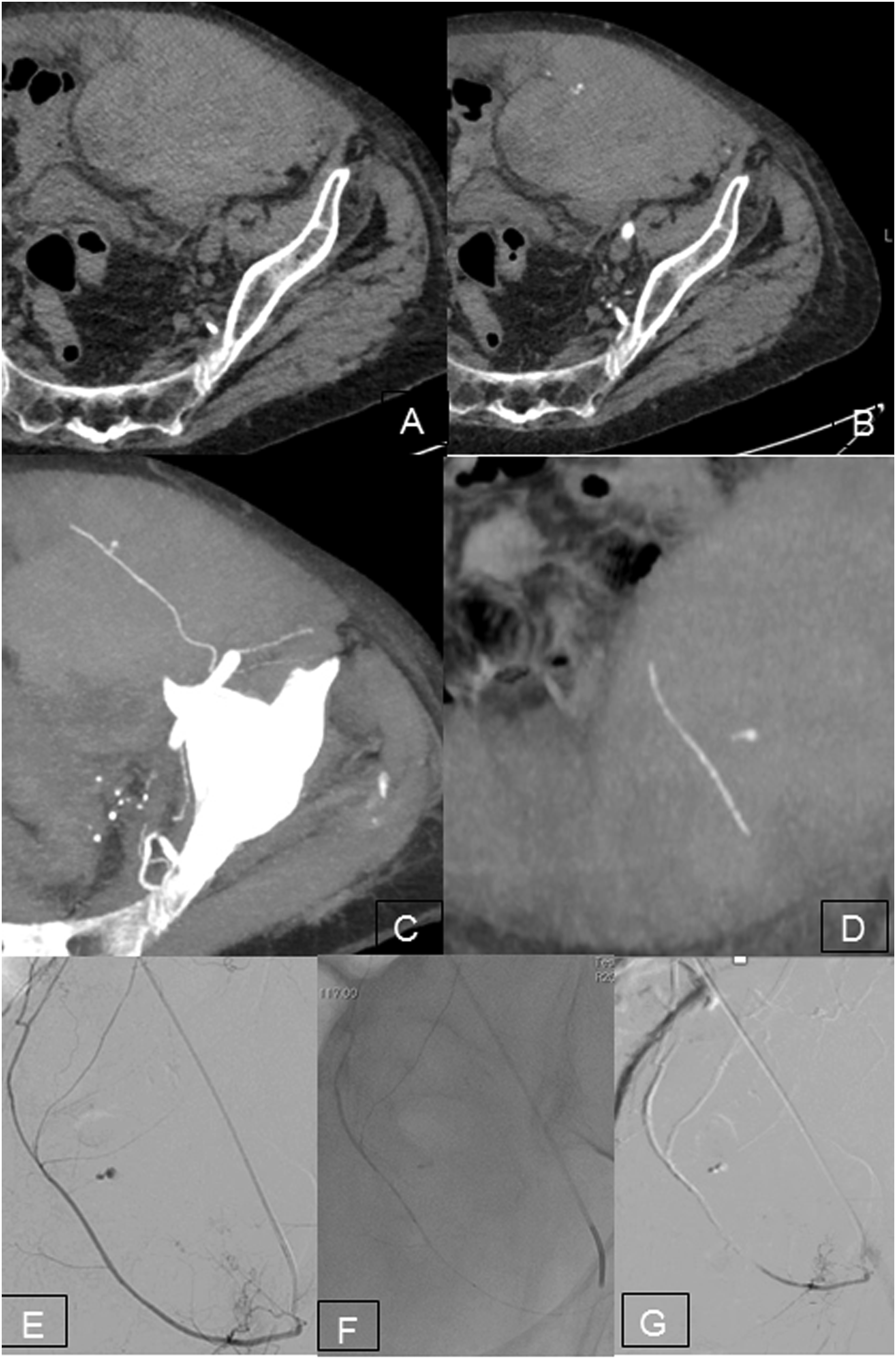

No major complications (procedure-related mortality and non-target embolization with distal ischemia) were encountered.
Two minor complications were reported: 1 case (2.4%) of puncture site-related complication (local self-limiting hematoma) and 1 case (2.4%) of post-embolization syndrome (abdominal pain) spontaneously regressive (Table 2). No cases of pseudoaneurysm formation nor catheter trapping were reported. None of the patients in analysis underwent surgical evacuation of the hematomas.
The median hospital stay was 7 d.
At 30-day follow-up, all patients were in good clinical condition but 2 (4.7%) died from multiorgan failure non-related to the bleeding event.
Discussion
RSH is a rare clinical condition presenting with multiple and often non-specific symptoms. Abdominal pain and a palpable mass in one of the lower abdominal quadrants are the most characteristic clinical manifestations of this condition. 3 Several clinical signs can lead to the suspicion of RSH during physical examination: the Fothergill sign (positive when the contraction of the abdomen reveals a less mobile midline mass), the Laffont sign (presence of ecchymosis over the abdominal mass), the Nadeu sign (abdominal pain due to the elevation of lower limbs or head), or the Carnett sign (positive when pain increases from supine decubitus to the sitting position). 8
As previously mentioned, the most common factor predisposing to RSH is the spontaneous bleeding during anticoagulation therapy. In this setting, taking into account the rising number of patients treated with anticoagulant drugs (including vitamin K antagonists and new oral anticoagulants—NOAC), it is likely that spontaneous RSH will be more frequently diagnosed in the future. At any rate, RSH may also develop following a direct abdominal trauma, abdominal surgery or intense contraction, pregnancy, and coughing. Primitive coagulation disorders are predisposing factors too. 2
The diagnosis can be difficult and is not infrequently mistaken for other causes of abdominal pain or acute abdominal injury, but early recognition is pivotal to reduce potential complications associated with rectus sheath hematoma. Ultrasonography and, even more, CT always led to a correct diagnosis of RSH. Based on CTA findings, Berna et al have described a useful method of classification for RSH: type I hematomas that are slight and do not require any hospitalization because they usually are self-limiting; type II and type III RSH are, respectively, moderate and severe hematomas and do require hospitalization and treatment because patients may develop complications such as hemodynamic instability, abdominal compartment syndrome, and occasionally, death. 7
Recommendations for the management and treatment of RSH have not been yet clearly defined 9 : at the moment, if patient is hemodynamically stable, RSH treatment substantially consists in medical procedures including reversal of anticoagulation, analgesia, rest, ice, compression, and blood transfusions when needed. 2 The indication for endovascular treatment is not well standardized and normally based on RSH size, patient’s general conditions, or the risks for complications. Actively bleeding hematomas leading to continuous hemoglobin decline and contrast extravasation at the CTA need to be aggressively treated since the arteriography with selective embolization of the blessed epigastric arteries were demonstrated to be highly effective.5,10
In this series, we reported failure of conservative treatment in about the half of cases. In this perspective, we believe that an aggressive percutaneous treatment should be considered as the first approach in severe active arterial bleeding and otherwise be discussed on a case-by-case basis according to clinical and radiological data.
In fact, the possibility to perform a selective catheterization, the use of microcatheters and the versatility of embolization material allow appropriate management in several setting so that Zack JR et al suggest that the endovascular treatment should be considered as the gold standard. 5
Indication for open surgery (evacuation of the hematoma and hemostasis with vessel ligation) should be addressed only after the failure of the other therapeutic options.11,12
The vessel occlusion may be performed using multiple embolic agents such as particles, gelatin sponge, and coils that are effective in controlling bleeding in most cases. Coils are widely used because they are ideal for bleeding in a single vessel, usually with a larger diameter. When embolization requires precision, they are easily positioned at the target location, with immediate interruption of the bleeding.9,13 However, it persists the risk of re-bleeding from collaterals or recanalization. 14
Conversely, glue embolization allows preventing re-bleeding because both the “front and back door” branches feeding the bleed are occluded during the procedure without the need to be administered at the bleeding site; additionally, thanks to its liquid nature, it is useful in situations where it is impossible to catheterize very small or irregular branches. Actually, to treat bleeding from small and tortuous vessels and a rich collateral net, coil embolization is often difficult and non-resolute; moreover, particulate agents cannot be precisely placed in the site of the vessel injury and may occlude the microcatheters or vessels proximal to the bleeding site. 15
Nevertheless, the use of glue is less frequently reported probably due to the risk of possible uncontrolled reflux during the injection with consequent ischemic complications. To our knowledge, the present study represents the largest single center series reported in the literature: in our experience, all patients were treated by injecting glue via a microcatheter without complications related to uncontrolled reflux during the injection as also previously reported. 10
Using glue, microcatheter entrapment may also occur even if it is relatively rare. In this, peripheral circulation generally does not lead to adverse clinical consequences; however, this complication may be minimized carefully selecting the glue:Lipiodol dilution. In fact, the glue can be mixed with ethiodized oilLUF in different ratios to modify the polymerization time, allowing to embolize more distally or proximally depending on glue:LUF ratio. 15
The speed of injection should be also modulated according to vessels to treat, and during the injection, forceful movements of the catheter should be avoided, removing redundant loops in microcatheter to guarantee more control if pullback maneuver is required. 15
Furthermore, in term of costs, embolization with glue appears to be more cost-effective. 16 Normally, coil embolization requires multiples coils or a combination of materials to be efficacious, making related costs rise. For instance, Wick et al, 16 in their study, used pushable or detachable microcoils in 46 patients, and in 60.8% of cases they needed to combine with PVA (polyvinyl alcohol) particles of different sizes. Conversely, 1 mL of glue, that is sufficient for successful treatment in the majority of cases, is comparable in cost to a single conventional pushing coil. 17
Conclusion
Glue embolization represents an effective and safe therapeutic approach for the treatment of RSH-related arterial bleeding and should be considered as the first approach in severe active arterial bleeding. By a single, cost-effective embolic agent, definitive embolization was achieved, with no severe procedure-related complications.
Limitations
This is a retrospective study from a single institution focused only on a small sample size of RSH. Additionally, there was no control group treated with other embolic agents to compare the efficacy of glue embolization. Third, being a retrospective study, no complete long-term follow-up was available.
Despite these limitations, this study documents a real-world scenario for use of glue in treatment of RSH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.