
Abstract
Inferior mesenteric artery (IMA) aneurysms represent the minority of visceral aneurysm presentations. A 57-year-old female was admitted with a symptomatic IMA aneurysm secondary to atherosclerotic disease. She was treated with open excision which revealed a contained ruptured of a true aneurysm. This case highlights the challenges of an accurate preoperative diagnosis of IMA aneurysm and the correct position of the recent guidelines on visceral aneurysms issued by the Society of Vascular Surgery (SVS).
Introduction
Inferior mesenteric artery (IMA) aneurysms have a low prevalence and are the rarest of the visceral aneurysms, representing less than 1% of them. 1 They can present in a number of ways, ranging from being asymptomatic to haemodynamically unstable patients secondary to rupture. Inferior mesenteric artery aneurysm can be the sole vascular anomaly or it can be associated with other pathologies. The following case describes a histological pseudoaneurysm which had been reported as a true aneurysm radiologically.
Case Presentation
A 57-year-old female presented to the general surgery department with a 5-day history of constant, severe cramping pain in her lower abdomen which radiated to her back. Her past medical history included bipolar disease and gastro-oesophageal reflux disease.
On admission, her haemoglobin was 121 g/dl, the biochemical profile including liver function tests were normal and inflammatory markers were not raised.
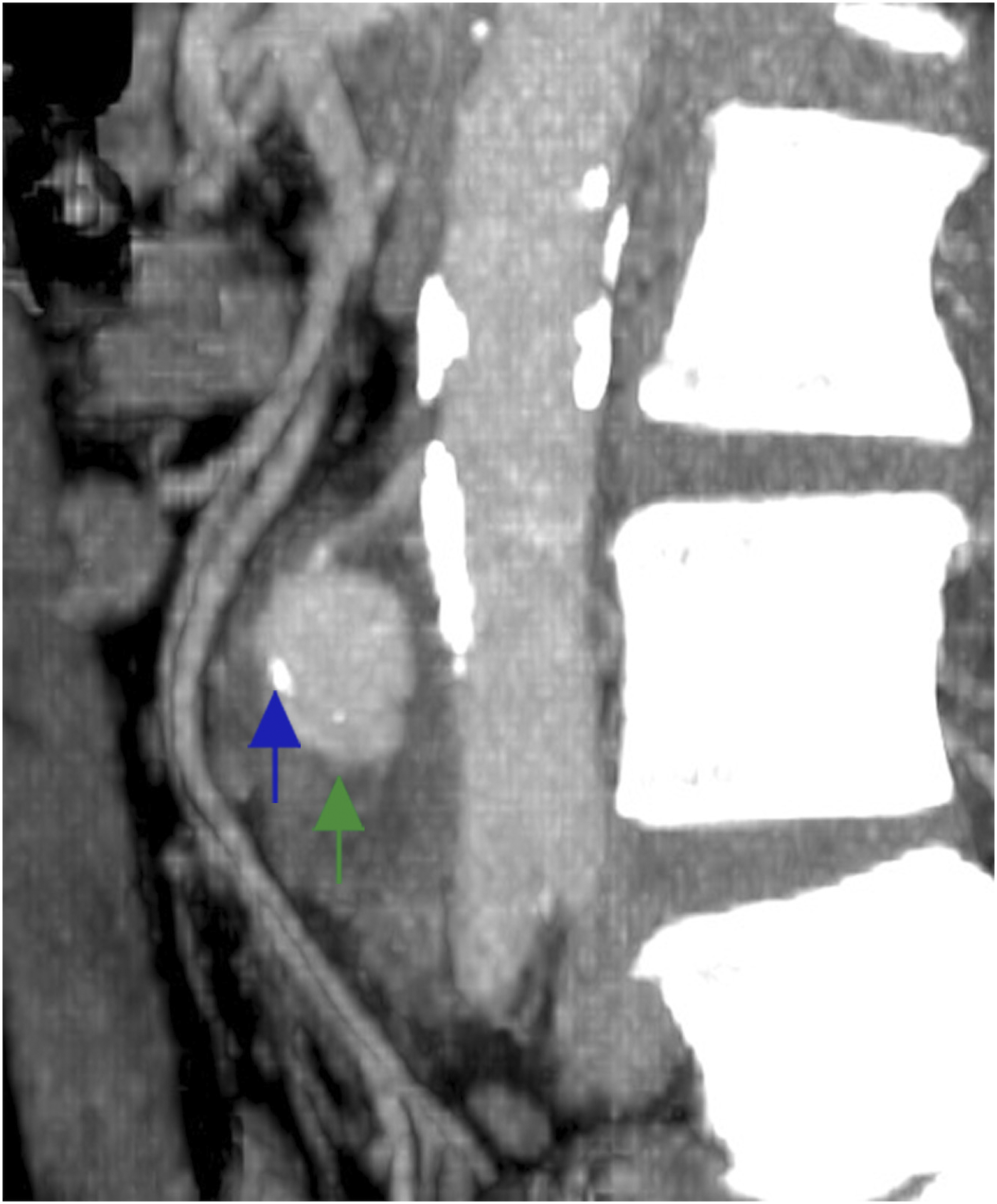
A mixed phase computerised tomography (CT) scan of her abdomen and pelvis was performed, which identified an IMA aneurysm measuring 3.2 × 2.9 × 5.4 cm (Figure 1). Small flecks of calcification were noted within the aneurysmal wall which was noted to be irregular and thin-walled (Figure 2). Otherwise, the scan was unremarkable apart from mild diverticulosis without signs of acute infection. Axial CT image of an inferior mesenteric aneurysm (green arrow) anterior to the abdominal aorta (blue arrow). Sagittal CT image of the inferior mesenteric artery aneurysm (green arrow) showing the calcium deposited in the wall (blue arrow).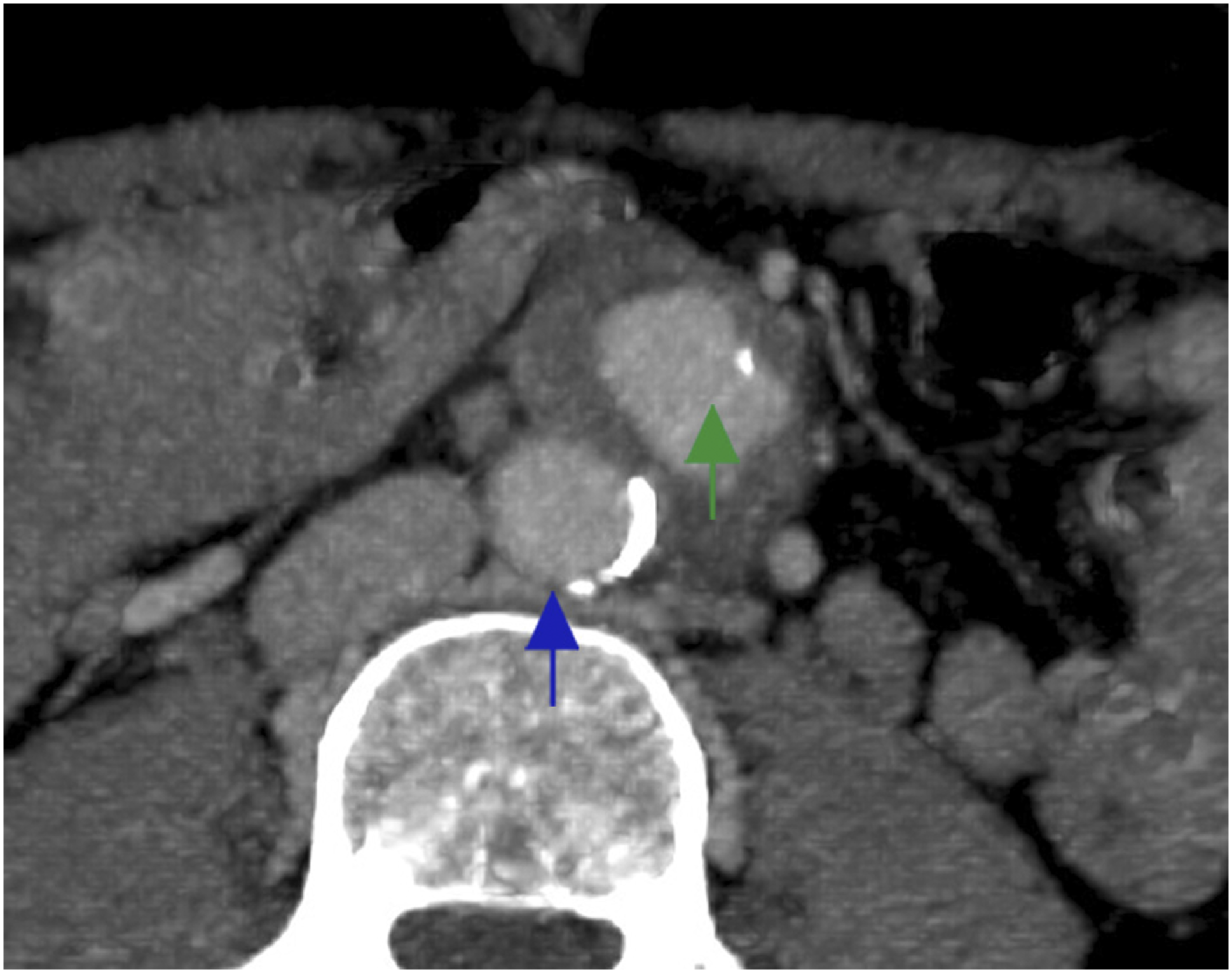
The case was discussed in the local vascular multidisciplinary team meeting. Despite the limitations of a mixed phase CT scan, the superior mesenteric artery (SMA) and the coeliac artery (CA) were found to be patent with sufficient evidence of collateral circulation to the left colon. Endovascular intervention was precluded because of the small neck of the aneurysm and lack of local experience cannulating the IMA via the Drummond artery. Hence, it was decided to perform an open surgical repair involving primary ligation of the aneurysm without revascularization. If, intraoperatively, concerns regarding bowel ischaemia or viability were raised, a revascularisation procedure or colonic resection was to be considered. The management plan was discussed with the patient who signed an informed consent for the procedure.
A midline laparotomy was performed, and the IMA aneurysm was dissected (Figure 3) and excised (Figure 4). The proximal and distal ends were suture ligated. The patient was discharged from hospital 6 days after the operation having had no post-operative complications. Intraoperative pictures of the IMA aneurysm (green arrow) showing relationship to the common iliac vessels and the aorta bifurcation (blue arrow). Excised inferior mesenteric aneurysm.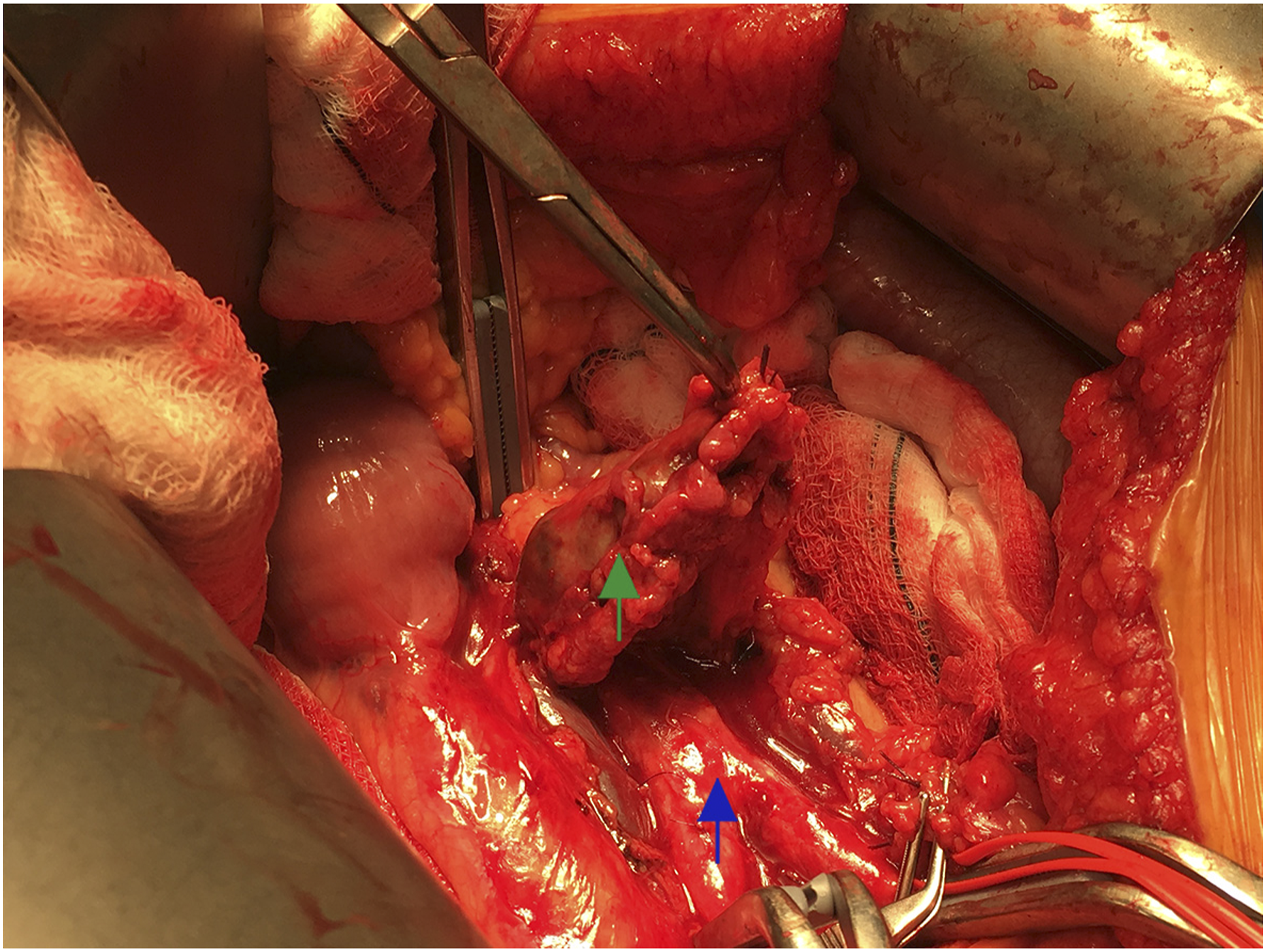

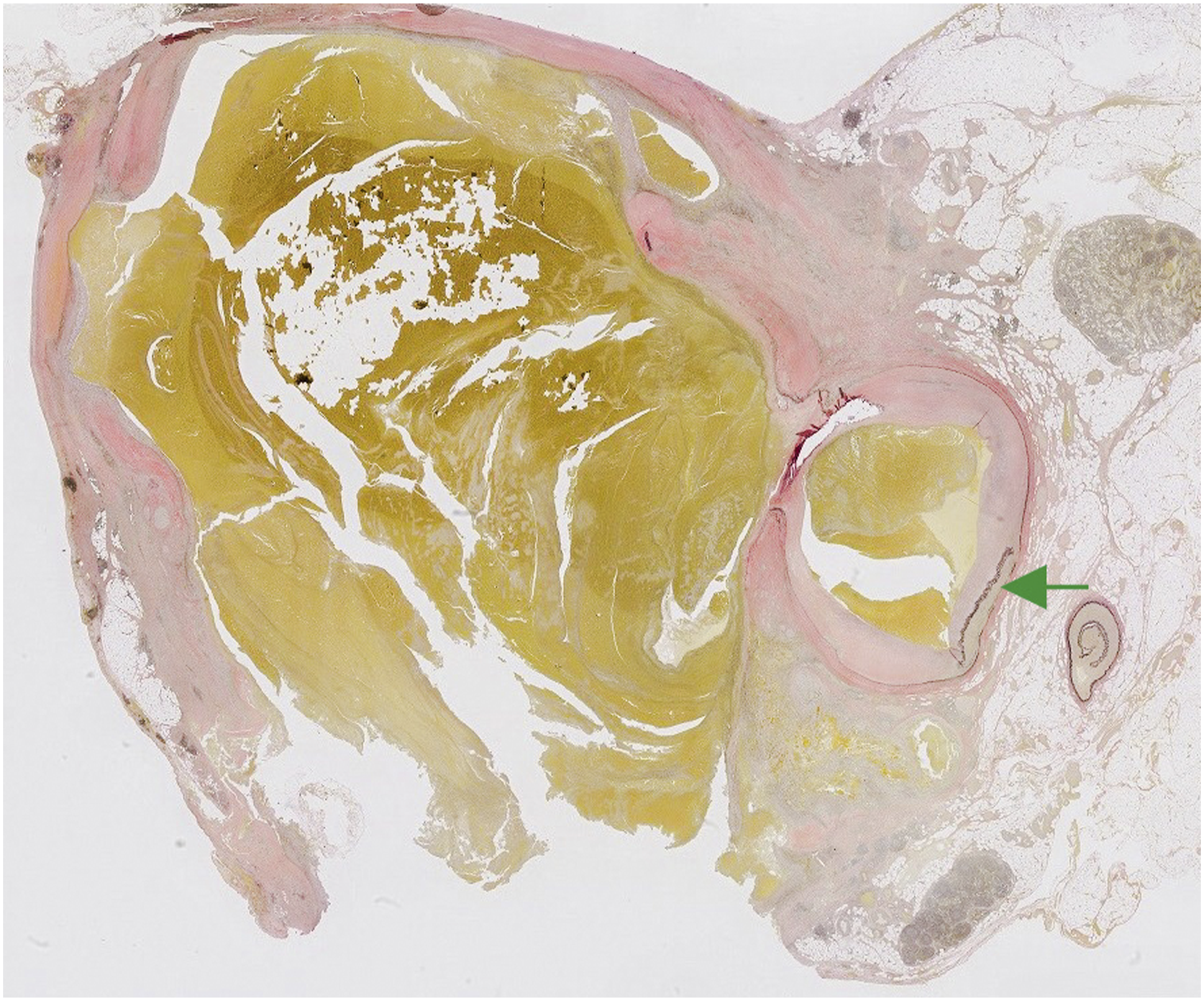
Histopathological examination of the excised artery showed the presence of calcified atheroma in its wall, supporting atherosclerosis as its aetiology (Figure 5). Furthermore, it showed disruption in the arterial wall and complex blood filled spaces with organising thrombus, surrounded by fibrosis in the adjacent adipose tissue. Elastin van Gieson (EVG) stain (Figure 6) demonstrated a site of probable rupture in the arterial wall and the absence of an elastic layer around the blood filled spaces, suggestive of a ruptured true aneurysm or pseudoaneurysm. Haematoxylin and eosin stained section, showing the inferior mesenteric artery (blue arrow), with the calcified atheroma (green arrow), and the blood-filled space within the adjacent adipose tissue, surrounded by fibrosis (yellow arrow). Elastin van Gieson stained section, showing the discontinuous, wavy internal elastic lamina of the arterial wall (green arrow), and the absence of the elastic layer around the blood-filled space.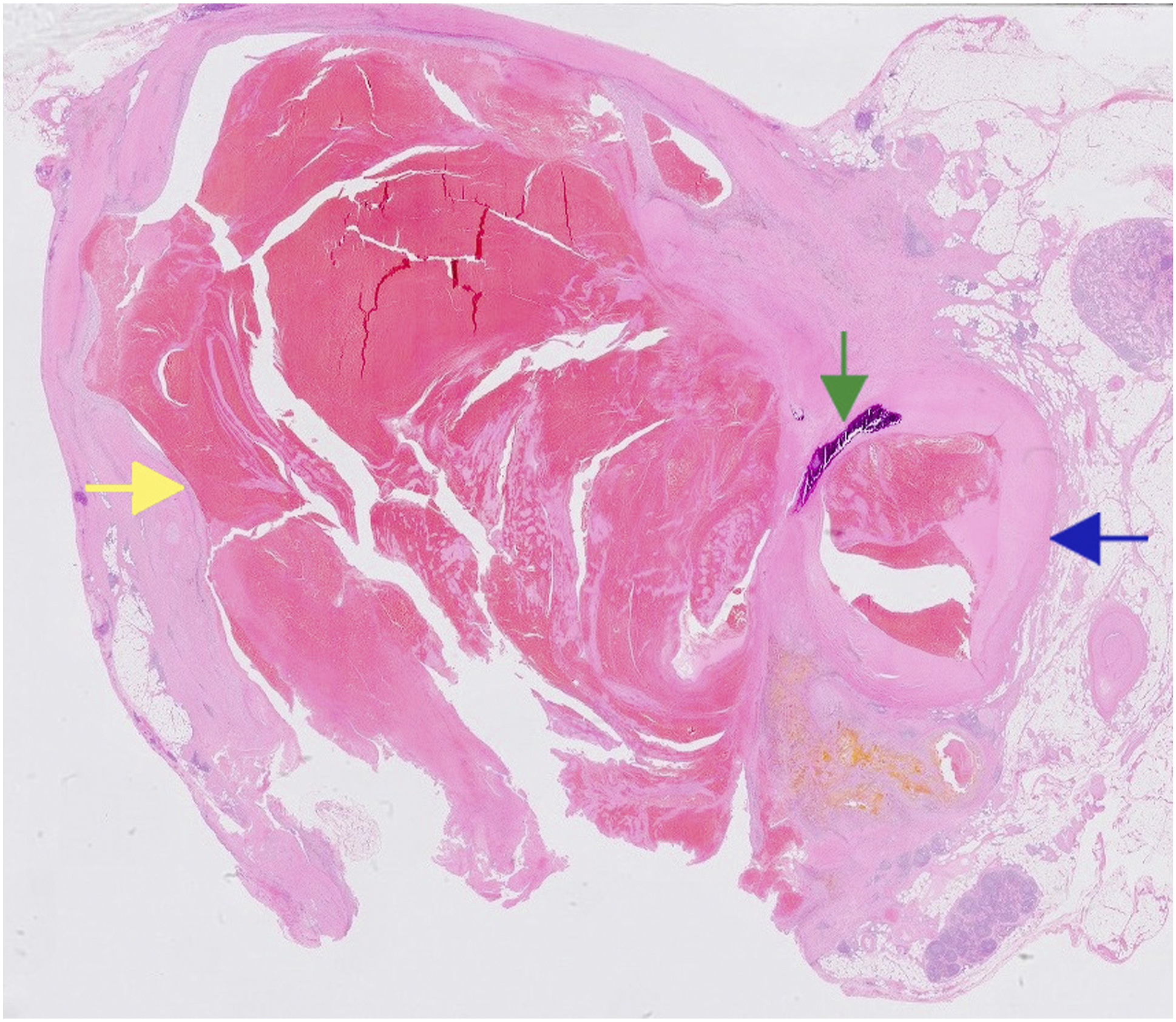
The patient was followed up in the outpatient clinic having made a full recovery from her operation. No subsequent post-operative symptoms such as altered bowel habit or signs of ischaemic colitis were noted during a 6-month follow-up period.
Discussion
IMA aneurysms present either incidentally as part of diagnostic imaging for other conditions or with non-specific symptoms such as abdominal pain, lower back pain and haemodynamic instability due to rupture.2,3
Atherosclerosis is considered to be the main aetiology which can predispose directly to visceral artery aneurysm formation. 1 However, a number of authors have suggested that the whole process may be secondary to CA and SMA occlusion resulting in a high flow state through the IMA and aneurysmal degeneration.2,4-6 Less frequent pathologies such as connective tissue disorders, infections causing mycotic aneurysms, autoimmune diseases (Behcet’s disease, polyarteritis nodosa and Takayasu’s disease), segmental artery mediolysis, trauma or iatrogenic injury5,7-9 may lead to IMA aneurysms.
Recent guidelines from the Society of Vascular Surgery (SVS) have advised the treatment of all colonic visceral aneurysms due to an associated 70% rupture rate. 10 A significant number of literature studies advocated intervention when the aneurysm diameter is 1 cm in the proximal segment and 2 cm in the distal segment of the IMA and for all pseudoaneurysms.3,5,11
The histopathological findings of a possible pseudoaneurysm were unexpected as it did not support the intraoperative observations during dissection and manipulation of the vessel. Furthermore, the patient did not have any of the risk factors that might cause the formation of a pseudoaneurysm, such as iatrogenic vessel injury (recent abdominal surgery or visceral artery catheterisation), radiological or biochemical indication of intraabdominal sepsis or any past medical history or radiological findings of vasculitis. Therefore, the findings represent a contained aneurysmal rupture into the mesentery which, with time, could have evolved into an uncontained rupture and resulted in a different clinical presentation with haemodynamic instability.
In our case, as the patient was fit for surgical intervention, she met the criteria for an open excision as posed by the SVS guidelines and the previous literature evidence. 10 The new guidelines ensure that there is no delay in treatment of misdiagnosed small true aneurysms which are in fact pseudoaneurysms.
There is no clear superiority of the type of intervention due to the rarity of the condition. The guidelines recommend an open approach for cases requiring haematoma evacuation. 10 Primary simple excision with revascularisation or colonic resection is not always required if there is sufficient collateralisation. Open excision with revascularisation has been performed and proven to be effective with a number of different methods. Tan et al 2 describe the re-implantation of the IMA artery into the left iliac artery emphasising the need for the anastomosis to be tension free. Others have reimplanted the IMA into bypass grafts when concurrent iliac disease has been treated. 9 Troisi et al 4 describe the use of a prosthetic tube graft to revascularise the IMA after excision of the artery. Tube interposition graft was used due to the elongation caused by the aneurysmal segment instead of an end to end anastomosis. Edogawa et al 5 described a case involving revascularisation of an occluded SMA followed by aneurysm excision and further revascularisation of the IMA. All of these authors performed reconstruction procedure either for severe stenosis or occlusion of the collateral circulation (SMA and CA).
Endovascular therapy is advocated as a means of appropriate treatment although associated with the risk of bowel ischaemia and subsequent need for early post-interventional surveillance. 10 A variety of endovascular techniques have been presented in the literature as case reports or series.9,12 Hansraj et al 9 describe coil embolisation of the IMA aneurysm via an antegrade approach embolising the outflow first. The patency of the collateral blood supply to the bowel (marginal artery of Drummond) is important when vessel embolisation is being considered. 13 The main contraindication to endovascular approach as a definitive repair would be infective mycotic aneurysms. The introduction of foreign body into an infective field is not justified without prolonged course of antibiotic therapy first. 14
Conclusion
IMA aneurysms are an extremely rare vascular pathology and therefore negate any clear evidence-based guidelines published. Despite radiological investigations, diagnostic uncertainty can still be present. The most recent guidelines advocate a much lower threshold for intervention than previously advocated in the literature. It is appropriate to consider endovascular or open repair bearing in mind the indications and contraindications of each approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.