
Abstract
In this report, we describe a 35-year-old female with neurogenic thoracic outlet syndrome (NTOS) who presented with a post-pull pneumothorax following first rib resection and anterior scalenectomy (FRRAS). During the FRRAS, a large amount of scar tissue was observed surrounding the first rib, resulting in a tear in the pleura as the rib was resected. This created a pneumothorax which required chest tube placement and observation overnight. The patient was discharged 1 day post-operatively, feeling well but was then re-admitted 2 days later due to the presence of a recurrent pneumothorax. A chest tube was placed again, and the patient was monitored until symptom resolution. The occurrence of a post-pull pneumothorax has never been reported following FRRAS in TOS patients. The patient’s symptoms have improved 4 months post operation.
Introduction
Neurogenic thoracic outlet syndrome (NTOS) is a disease caused by compression of the interscalene triangle from anterior scalene muscle inflammation. TOS has an incidence of 3–80/1000 individuals of the population, and 95% of those cases present as neurogenic. 1 The most common complication of first rib resection and anterior scalenectomy (FRRAS) is a pneumothorax when the rib is resected. Here we report a case of an NTOS patient who developed a pneumothorax during the FRRAS and then later re-developed the pneumothorax 3 days after surgery.
Case Report
A 35-year-old female nurse with a previous diagnosis of neurogenic thoracic outlet syndrome presented to our clinic with worsening symptoms following a motor vehicle accident. She received Botox injections in both the right and left scalene muscles which provided temporary relief. Physical therapy regimen did not improve her symptoms. However, the motor vehicle accident resulted in increasing weakness and numbness within her right arm, leading to a decreased activity state.
Upon physical exam, the right anterior scalene muscle was both enlarged and tender. Ulnar nerve strength was moderately weak while both medial and radial nerve distributions were strong on the right. The left side presented with normal strength in ulnar, medial, and radial nerve distribution. The patient had a positive elevated arm stress test (EAST) at 30 seconds with both numbness and pain. Bilaterally, there was no presence of a subclavian bruit upon abduction. The exam demonstrated symptoms consistent with right (NTOS), and a right first rib resection and anterior scalenectomy (FRRAS) was recommended.
The patient underwent a transaxillary first rib resection and anterior scalenectomy. The subclavius tendon, first rib, anterior scalene muscle, and middle scalene muscle were easily identified within the space. The anterior and middle scalene muscles were tightly wrapped around both the subclavian artery and nerve root, and the subclavious tendon was large. The first rib was surrounded by a large amount of scar tissue, which resulted in a small tear in the pleural membrane. A 12-French chest tube was placed in a separate incision between the second and third ribs to treat the pneumothorax (figure 1). Anesthesia performed a pectoralis major block to relieve post-operative pain. Initial post-operative chest radiograph shows right chest tube in place following right FRRAS. No obvious pneumothorax appreciated. Small hematoma present in right upper lobe.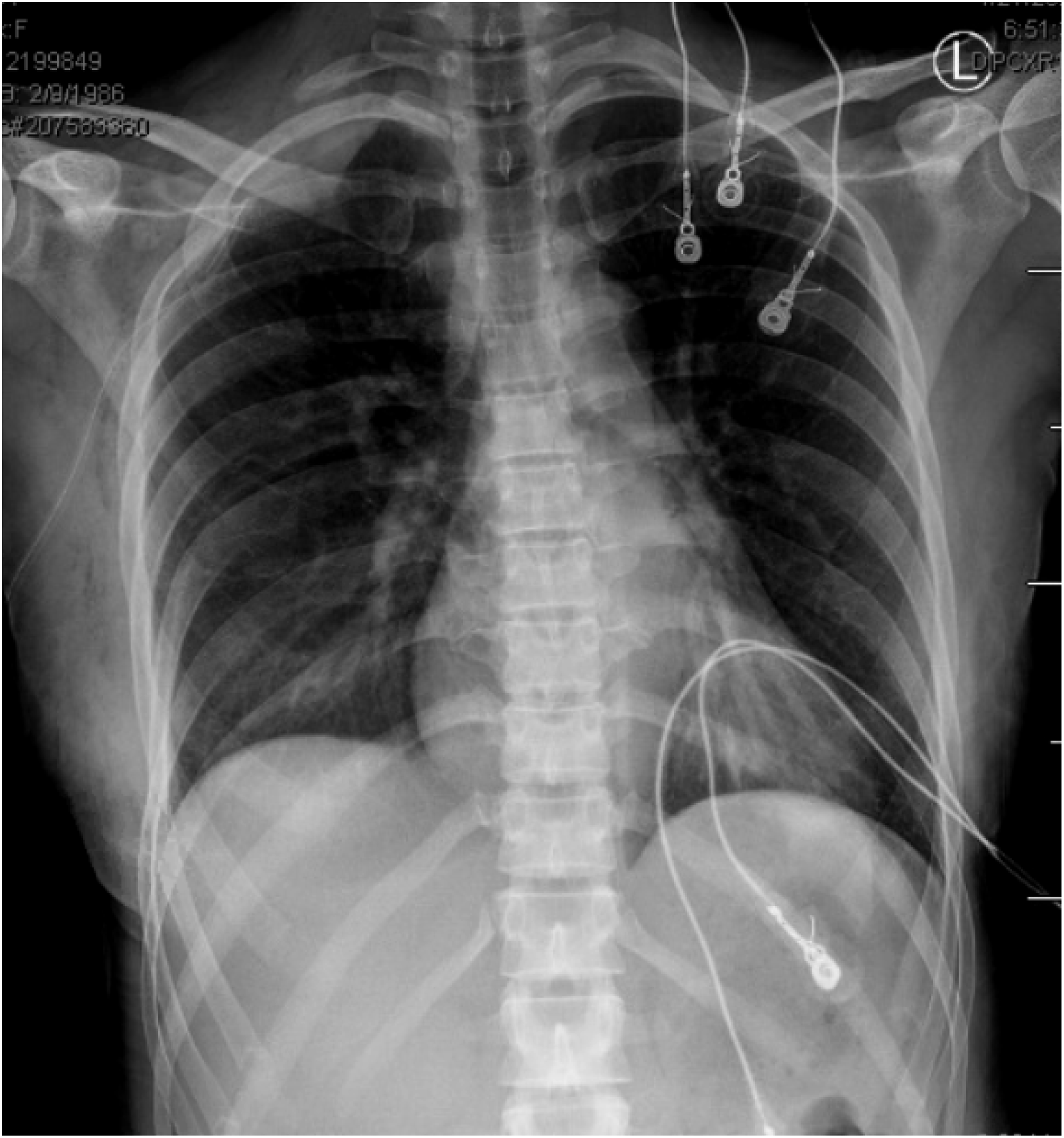
The chest tube remained on suction until midnight which was then changed water seal. The next morning, the patient’s chest tube was removed after a chest radiograph confirmed no pneumothorax, however, a small hematoma was observed in the right upper lobe. The patient was observed for 4 hours after the chest tube was pulled, and then discharged feeling well without any respiratory complaints (figure 2). Overall, the patient stayed 1 night in hospital before discharge. At our hospital, this patient’s case describes chest tube removal protocol. Chest radiograph upon interval chest tube removal 1 day post-operative after right FRRAS. No pneumothorax observed. Small hematoma present in right upper lobe. Patient was stable without any respiratory complaint.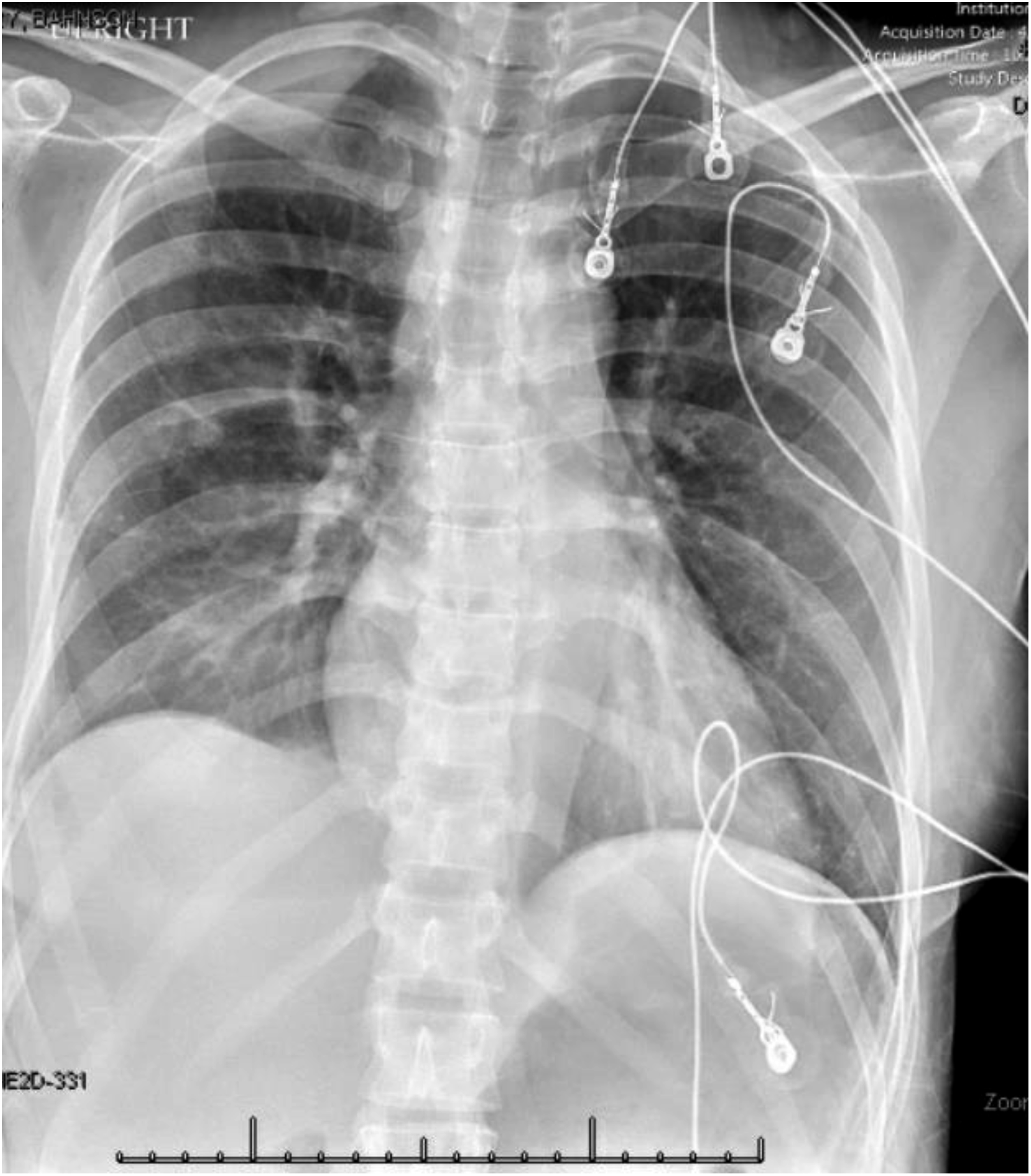
Two days after discharge, the patient called to report shortness of breath, and we recommended that she report to the nearest emergency room (ER). She presented in the ER with increasing shortness of breath and increasing chest discomfort. A chest radiograph demonstrated the presence of a moderated right pneumothorax (figure 3). The patient was re-admitted to Wake Forest Baptist Hospital for the placement of a new chest tube. She was monitored for 2 nights and then discharged with symptom resolution that was confirmed with a chest radiograph (figure 4). Chest radiograph from Emergency Room 3 days post-surgery demonstrates a large right pneumothorax (highlighted by yellow arrows). Small hematoma present in right upper lobe. Chest radiograph of patient 3 days after re-admission showing resolution of recurrent pneumothorax. Residual hematoma present in right upper lobe.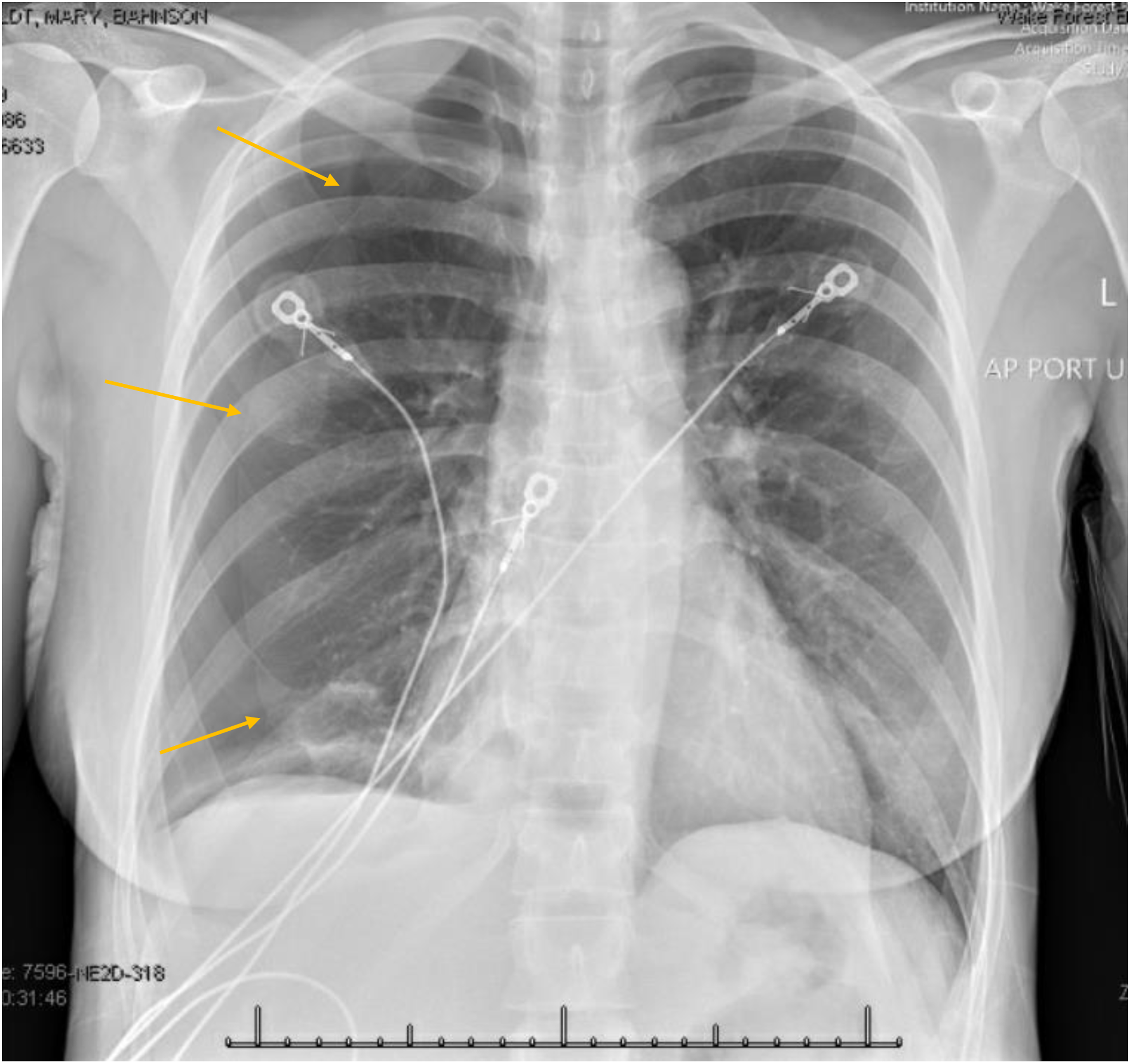

At 2 weeks post-operation, the patient reported symptom improvement and had begun physical therapy. The patient continues to remain symptom free 4 months post-operation.
Discussion
Neurogenic thoracic outlet syndrome (NTOS) is the compression of subclavian vessels and nerves of the brachial plexus. 2 Causes of this condition are typically associated with repetitive injuries due to patient’s line of work, physical trauma, and anatomical defects. 2 Symptoms often present as pain in the neck, shoulder, and arm as well as associated numbness, pain, and weakness in the fingers.2,3 These symptoms are exacerbated when the arm is positioned overhead, which is demonstrated by a positive elevated arm stress test (EAST). 2
Initial management for NTOS includes conservative measures which entails physical therapy and/or pain control interventions such as an anterior scalene muscle block.2,4 Once a patient fails conservative therapy, surgical FRRAS is recommended as treatment.
The most common complication of a first rib resection and anterior scalenectomy (FRRAS) is a pneumothorax.2-5 There is continued debate on the incidence of pneumothorax following FRRAS. Sanders et al determined the risk of development of pneumothorax after FRRAS to be 9%, 3 Freischlag et al up to 10%, 5 and Hosseinian et al. found 34% of patients who underwent a transaxillary FRRAS developed a pneumothorax. 2
The prevalence of a pneumothorax from a FRRAS parallels the physiology of the disease. Patients with (NTOS) often have large amounts of scar and connective tissue within the interscalene triangle as a result of chronic repetitive motion or injury. 1 As the first rib is resected, this scar tissue can pull on the pleural membrane, leading to a tear that exposes the lung which is subsequently treated with a chest tube. This event was seen in our patient’s FRRAS.
Treatment of a pneumothorax includes the placement of a chest drain, or if more severe the placement of a chest tube for air evacuation.3,4 The chest tube is typically removed 1 day post-surgery but is dependent on specific factors such as the absence of an air leak, a fluid amount of less than 200cc, and fluid that is benign in character. 6 After the chest tube is removed, the patient is observed for signs and symptoms of breathing difficulties. 7 If the patient develops signs of respiratory compromise, a post-pull chest x-ray is obtained to evaluate for a pneumothorax. The patient is considered stable if asymptomatic of breathing difficulty. Furthermore, a PPP may be undetectable upon discharge if a post-pull chest radiograph is not performed. There are currently no guidelines to demonstrate that a post-pull chest x-ray is necessary as long as the patient is asymptomatic and stable upon chest tube removal. 6
As of date, there has been no published data showing a recurrent pneumothorax occurring several days following chest tube removal following FRRAS. Causes of this patient’s recurrent pneumothorax remain unclear. Our discussion acts to clarify and explore what contributed to the development of the patient’s recurrent pneumothorax.
One possible explanation is that the recurrent pneumothorax may have been the result of a post-pull pneumothorax (PPP). A PPP is defined as the presence of air in the hemithorax on post-pull chest imaging. 7 PPP is associated with premature chest tube removal, or an air leak that allows air to enter the pleural space during the tube removal. 7 PPP has been shown to occur after chest tube discontinuation following invasive procedures. 8 Hendriks et al found the prevalence of PPP to be .23% after cardiac surgery 7 and Kugler et al. determined that 21.3% of 710 trauma patients were discharged with a residual PPP, but only 4% required re-intervention at a median of 7 days post-discharge. 8 Both of these studies reflect a more invasive surgical procedure than a transaxillary FRRAS, which could pose a greater risk of the re-development of a pneumothorax following chest tube removal. This may shed light on why a PPP has never been reported following FRRAS and why PPP is not extensively analyzed within the literature.
An alternate explanation of the recurrent pneumothorax includes chest wall thickness. Anand RJ et al investigated chest wall thickness as a risk factor for the development of pneumothorax after chest tube removal. 6 In this study, chest wall thickness was measured as the distance between the skin and the pleura at the level of the nipple via CT. 6 Anand RJ et al determined that those who have thinner chest walls are significantly more likely to experience PPP. Patients with thicker chest walls have more adipose tissue to provide a “seal” against the chest wall to which lowers the risk of the development of a PPP. 6 Our patient had a BMI of 20.00 kg/m2 which demonstrates a low amount of adipose tissue. However, without quantitative measurements of our patient, it is impossible to attribute our patient’s recurrent pneumothorax to a thin chest wall.
Conclusion
As demonstrated in our patient, pneumothorax is a known complication of FRRAS. However, the subsequent development of a recurrent pneumothorax 3 days post-operation of FRRAS has never been described. Since there is limited published research of a PPP following FRRAS it is of high priority to listen to the complaints of the patient in the initial post-operative period. Factors such as a thin chest wall, substantial scar tissue, and early chest tube removal may have contributed the development of recurrent pneumothorax in this patient. Future research should be done to determine if this recurrence would have been prevented by accounting for chest wall thickness in a thin patient or increasing the interval between chest tube placement and chest tube removal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the patient (or patient’s family/guardian) for publication of the case report and accompanying images.