
Abstract
Objective
Patients can be at risk of carotid artery dissection and ischemic stroke after cervical chiropractic manipulation. However, such risks are rarely reported and raising awareness can increase the safety of chiropractic manipulations.
Case Report
We present two middle-aged patients with carotid artery dissection leading to ischemic stroke after receiving chiropractic manipulation in Foshan, Guangdong Province, China. Both patients had new-onset pain in their necks after receiving chiropractic manipulations. Excess physical force during chiropractic manipulation may present a risk to patients. Patient was administered with recombinant tissue plasminogen activator after radiological diagnoses. They were prescribed 100 mg and clopidogrel 75 mg daily for 3 months as dual antiplatelet therapy. There were no complications over the follow-up period.
Conclusion
These cases suggest that dissection of the carotid artery can occur as the result of chiropractic manipulations. Patients should be diagnosed and treated early to achieve positive outcomes. The safety of chiropractic manipulations should be increased by raising awareness about the potential risks.
Introduction
Spontaneous dissections of the vertebral or carotid arteries account for 2% of ischemic stroke patients, but in young and middle-aged patients, it can account for 10% to 25% of ischemic stroke cases. 1 While there are many reports on cervical dissections, including vertebral or carotid arteries dissection, posterior circulation ischemic stroke following cervical chiropractic manipulation, there is a paucity of reports on dissections of the carotid arteries and stroke induced by cervical chiropractic manipulation. 2
Chiropractic manipulation therapy has been a common practice for many Chinese people to help relax the body. However, most privately owned chiropractic manipulation centers are not monitored by hospitals or medical institutions in China. Cervical chiropractic manipulation may cause serious complications and even death, 3 a risk that is possibly not widely noted by chiropractors. We report two patients who developed carotid artery dissections and ischemic stroke after receiving cervical chiropractic manipulation. We review the literature and discuss the mechanism, diagnosis, and treatment of cervical dissections and stroke following cervical chiropractic manipulation. We propose strategies to minimize the risk of cervical chiropractic manipulation in the future.
Case Report
Case 1
A 51-year-old man with a history of mild hypertension noted new-onset right neck pain 2 days following chiropractic manipulation. He was admitted to the emergency department with weakness in his left arm and leg for 1 hour with an NIH Stroke Scale (NIHSS) score of 3. Non-contrast computerized tomography (CT) of the brain was normal. After administration of recombinant tissue plasminogen activator (rt-PA), the patient improved, and the NIHSS score was 1 after 1 hour. Head and neck computerized tomography angiography (CTA) (Figure 1) confirmed right internal carotid artery occlusion. CTA: right internal carotid occlusion.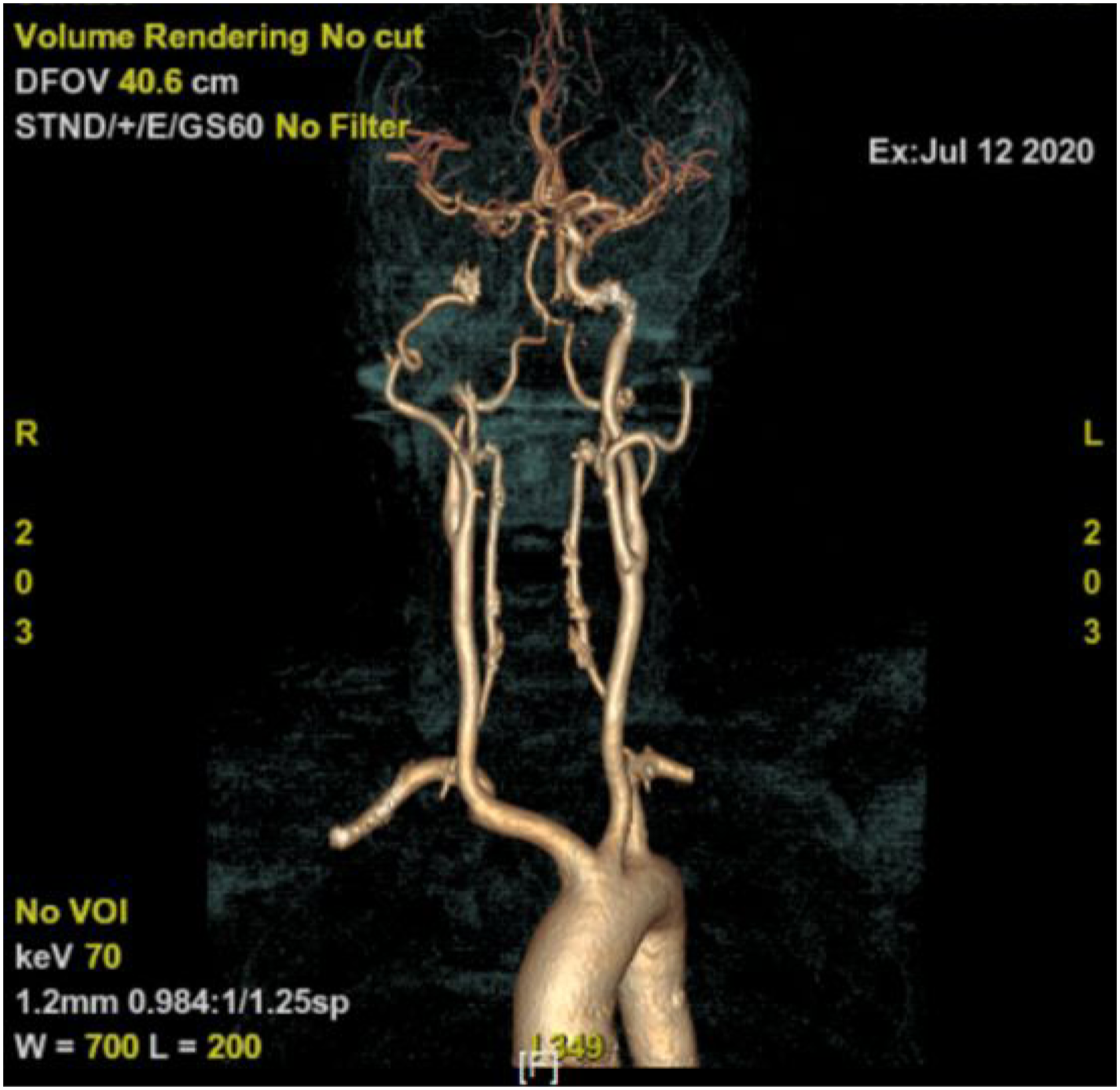
Magnetic resonance imaging (MRI) showed right frontal punctate infarction (Figure 2). Diffusion-weighted MRI with punctuate focus of ischemic in the right frontal lobe.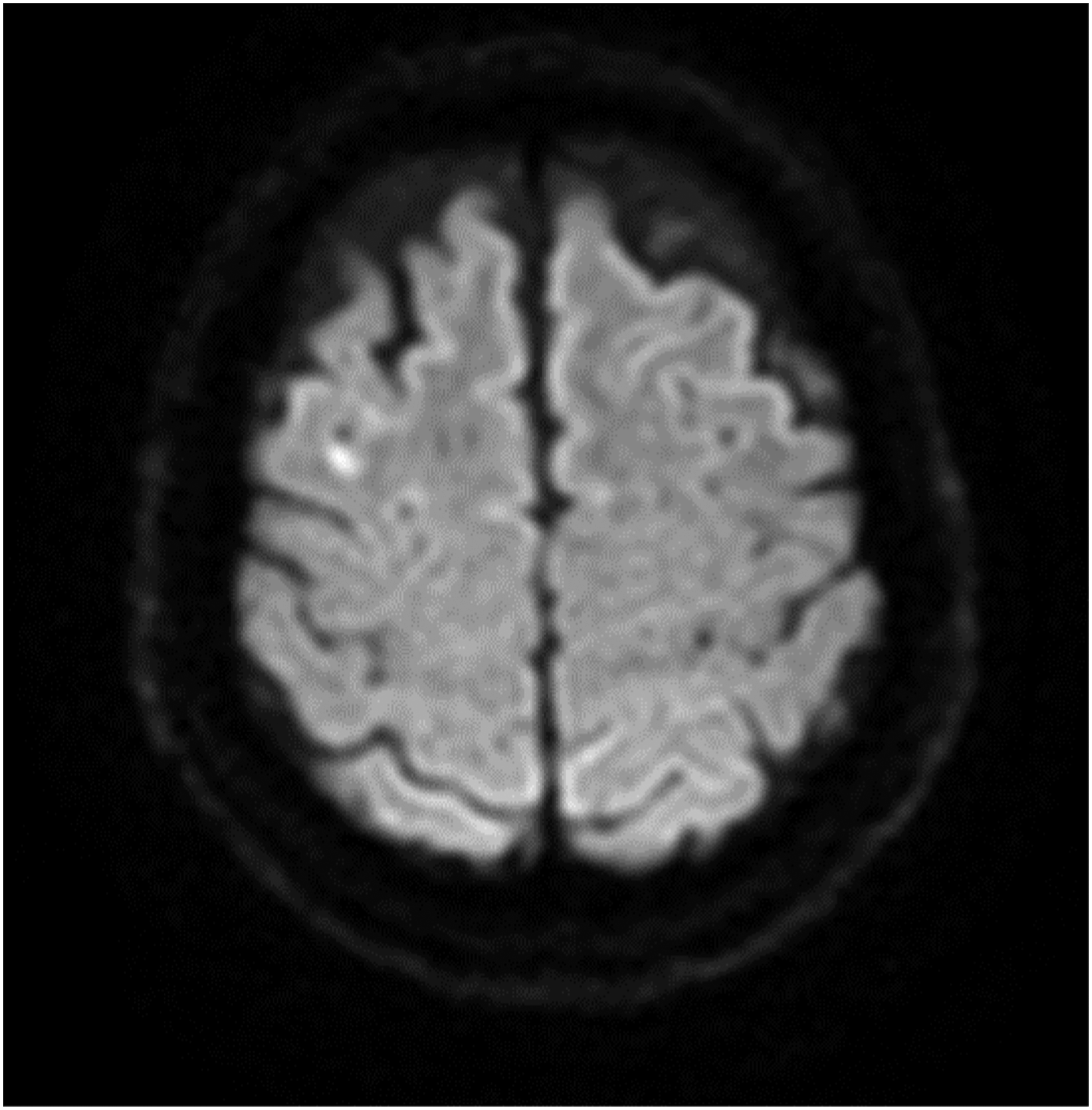
3D-digital subtraction angiography (DSA) showed dissection of the right C3 segment of the internal carotid artery (ICA) (Figure 3). DSA demonstrated dissection of the right C3 segment of the petrous internal carotid artery (arrow).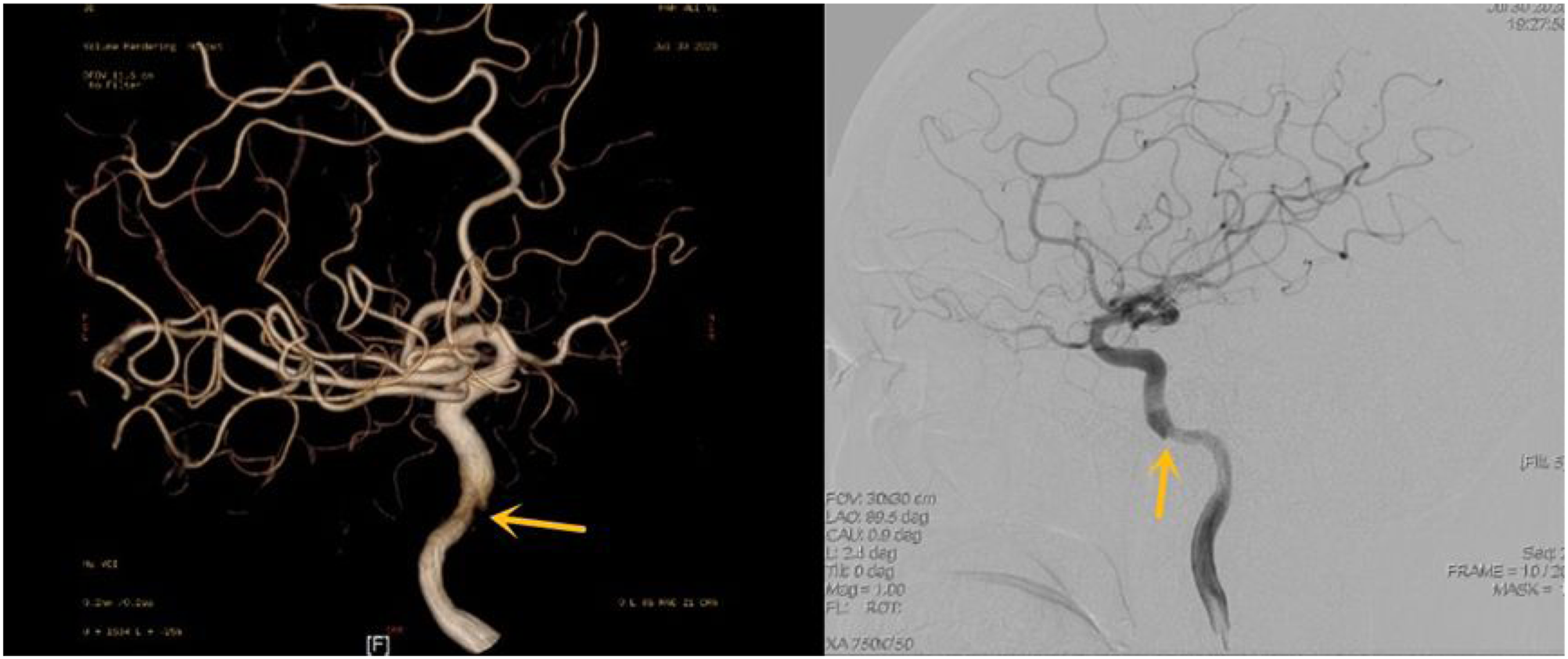
Aspirin 100 mg and clopidogrel 75 mg were given daily for 3 months as dual antiplatelet therapy. At 3 months, the patient was asymptomatic with a modified Rankin Scale (mRS) of 0 (Figure 4) and normal CTA. After 1 year of follow-up, he remained asymptomatic with an mRS of 0. At 3 months follow-up, head and neck CTA were normal.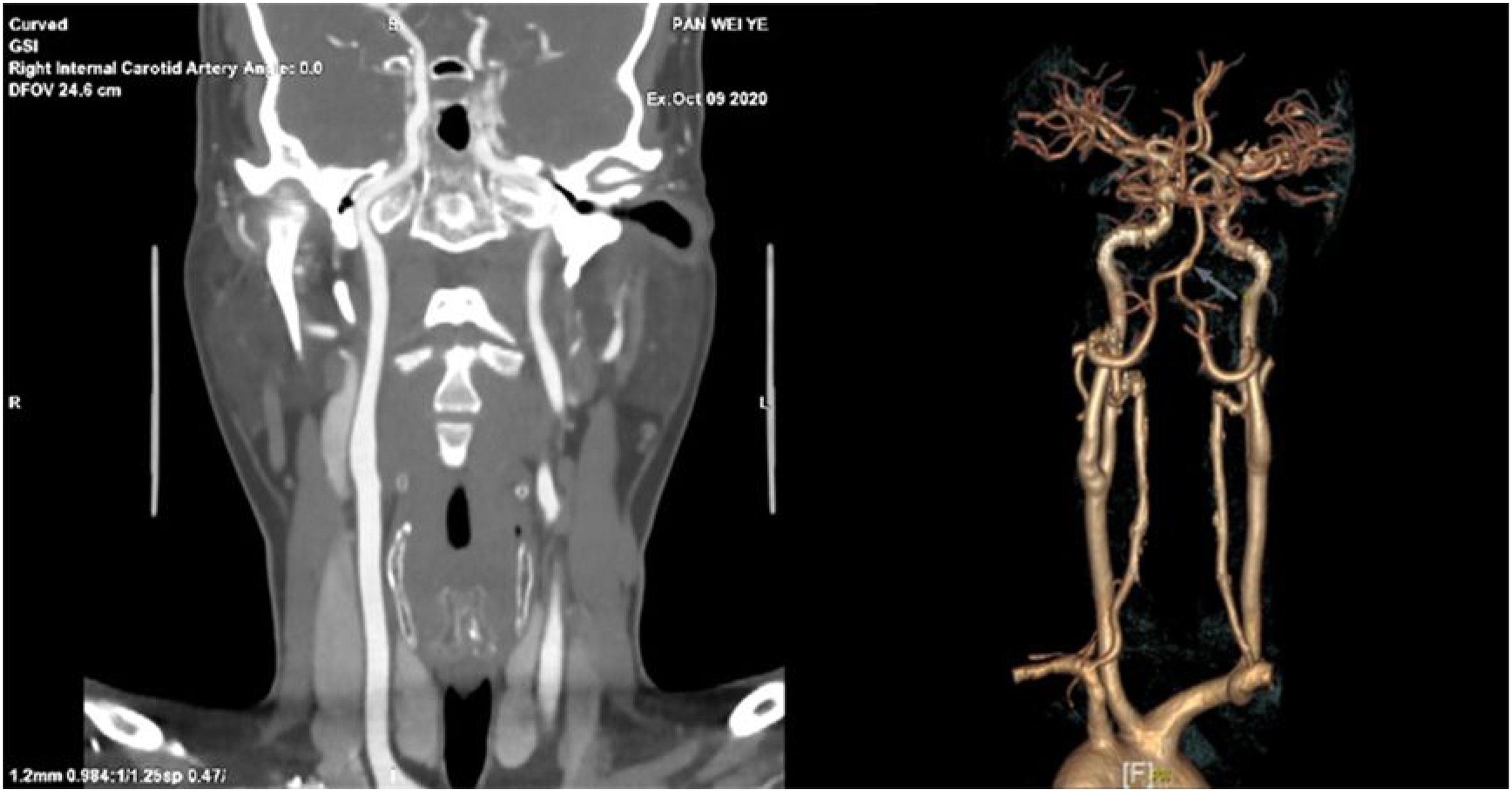
Case 2
A 55-year-old man with a history of cigarette smoking, no other cerebrovascular risk factors, received cervical chiropractic manipulation 1 day prior to presentation to the emergency department with new-onset of left hemiparesis, facial paralysis, right neck pain, and dysarthria lasting for 5 hours with an NIHSS score of 3. Non-contrast CT of the brain revealed right temporal cerebral infarction. A head MRI showed right frontal, parietal, occipital, and temporal cerebral infarction in watershed territory (Figure 5). Diffusion-weighted MRI showed right frontal, parietal, occipital, and temporal cerebral infarction in watershed and embolic territory.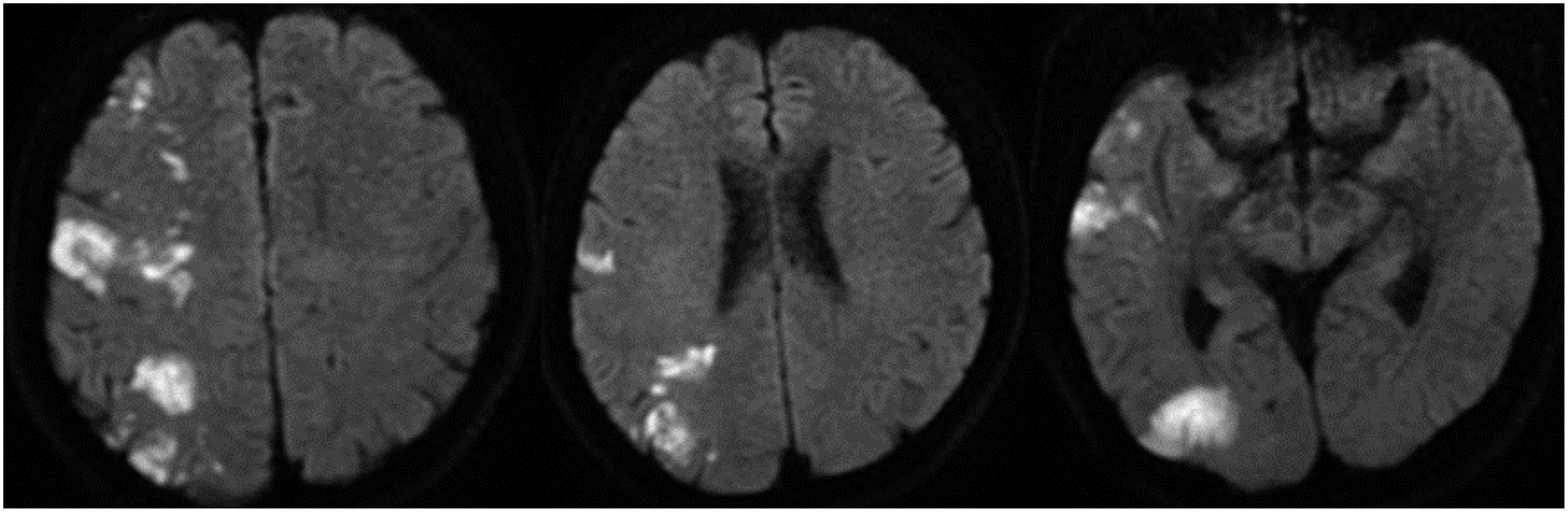
Head and neck MRA showed possible dissection of the siphon segment of the right ICA (Figure 6). Aspirin 100 mg and clopidogrel 75 mg were prescribed daily for 3 months as dual antiplatelet therapy. At 3 months and 6 months follow-up, the patient was asymptomatic with an mRS of 0. Head and neck MRA showed possible dissection of the upper petrous segment of the right ICA (arrow); other vessels were normal.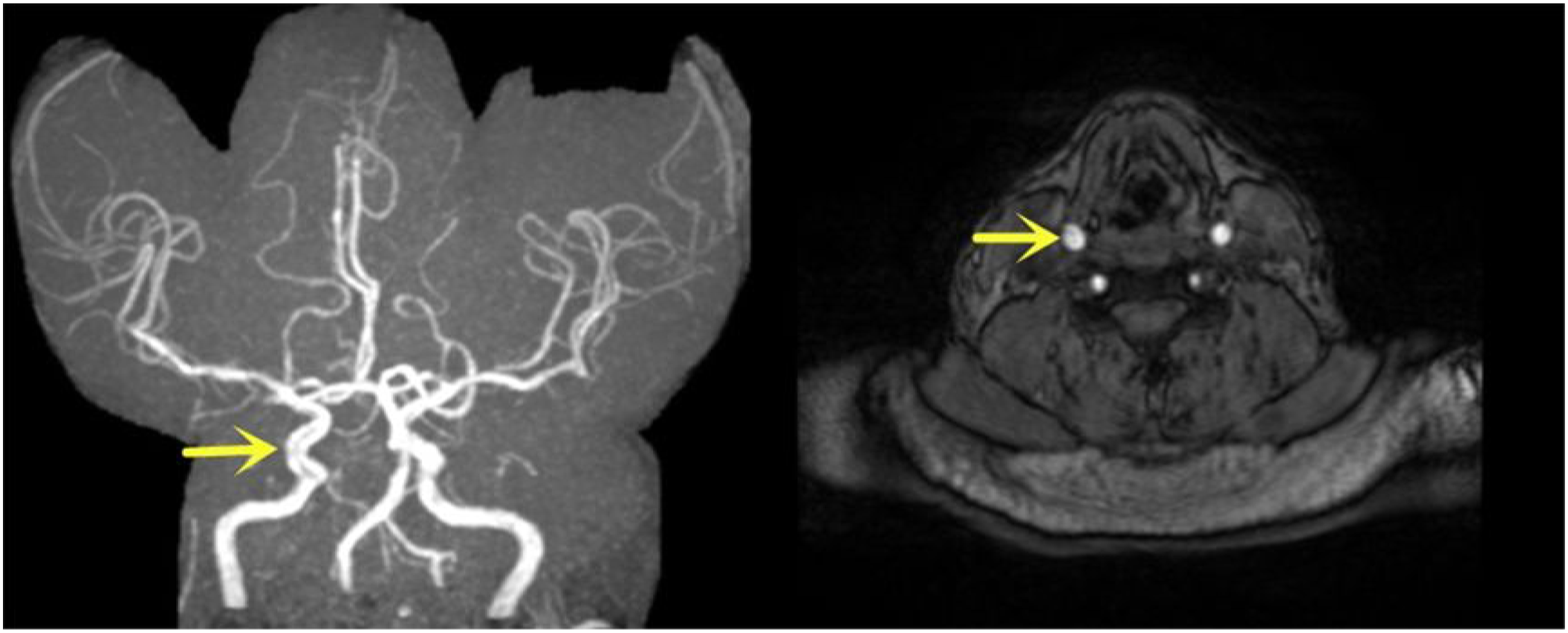
Discussion
Although there is no direct evidence that chiropractic manipulation causes cervical artery dissection, clinical reports have found that mechanical forces may contribute to cervical artery dissections. Population controlled studies have previously found correlations between chiropractic manipulation and vertebral artery dissection in young stroke patients. 4 The ICA is vulnerable to force applied to the neck between the base of the skull and the carotid bulb, and shear forces, particularly, can tear the intimal wall to cause dissection. 1 Patients with calcified carotid arteries may pose a risk for cerebral embolization induced by cervical spinal manipulation. Those with calcified carotid arteries should avoid aggressive cervical chiropractic manipulation and neck massage. 5 Focal ischemia can occur within hours to weeks induced by a dissection because the arterial blood supply is reduced or because thrombosis and embolism risk is increased as the vessel wall at the dissected location undergoes turbulence. 6
The diagnosis of cervical artery dissection is based on a complete history and physical examination and auxiliary examinations. 4 Patients with internal carotid artery dissection typically exhibit clinical features of pain in the neck, face, or head. Partial Horner syndrome can be accompanied after hours or days, followed by retinal or cerebral ischemia. The classic triad of ischemia, pain and Horner syndrome is present in one-third of patients. 4 If dissection of the carotid artery is suspected, ultrasonographic techniques are useful and cost-effective as the initial assessment. Helical CTA, as a minimally invasive technique, can provide high resolution images of both the arterial lumen and vessel. Because the high resolution of MRA and MRI can reveal the intramural hematoma, MR techniques are the gold standard for the diagnosis of vertebral and carotid artery dissection. 1
Thrombolysis treatment should be administered without delay in carotid artery dissection-related acute ischemic stroke patients without contraindications. Tissue-type plasminogen activator is safe to use in acute ischemic stroke patients secondary to cervical dissection, and does not increase the risk of intracranial hemorrhage, compared with the control group.4,7 Patients with TIA or ischemic stroke after vertebral arterial or extracranial carotid dissection were treated by antithrombotic therapy for at least 3 months to prevent recurrent events. 8 There are two randomized trials of Antiplatelet and anticoagulant treatments on carotid dissection, CADISS and another one afterward in Lancet. Antiplatelet and anticoagulant treatments are used to prevent thrombus and secondary embolism, and there are no differences in the rates of subsequent stroke or death between antiplatelet and anticoagulant treatments. 4 Stroke patients with cervical dissection have a low risk of recurrence at up to 1 year follow-up. 9 There is no difference in preventing stroke, or residual stenosis and occlusion, between anticoagulant or antiplatelet treatments. 8 If anticoagulation is chosen as the initial antithrombotic of choice, the duration of treatment is usually 3 to 6 months, and then transitioned to long-term antiplatelet treatment. The transition to antiplatelet usually takes into consideration of the irregularity of the vessel wall, residual arterial stenosis, and persistent artery occlusion though its evidence is lacking for risk of recurrent stroke in such situations. Indefinite antiplatelet treatment should be maintained for patients with recurrent cervical dissection history, family history of cervical dissection or underlying connective tissue disorder. 4 Endovascular treatment may be considered in patients with contraindication to antithrombotic use and failure of medical management. 10 Endovascular treatment could be considered for patients who have recurrent events despite antithrombotic treatment. 9 Endovascular therapy can be considered the effective treatment for pseudoaneurysm occlusion of low morbidity and mortality rates, and its success rate of was 84%. 11 For lesions causing severe clinically relevant stenosis or occlusion, the Wingspan stent system can be used for its high radial force and facilitation of angioplasty with the Gateway balloon. 12
Patients with cervical dissection can have favorable outcomes if diagnosed early and receive timely treatment, but serious neurological consequences also can occur. 4 A review reported twenty-six fatalities involving the dissection of a vertebral artery after chiropractic manipulation. 13
The incidence of cervical dissection following chiropractic manipulation is probably low, but it potentially causes serious consequences, even death. The following proposals are recommended to reduce the risk of cerebrovascular events after chiropractic manipulation: (1) Standardizing training of chiropractors, with coverage of anatomy, physiology, safe chiropractic manipulation guidelines to minimize the risk of cervical dissection and cerebral embolism. (2) If circumstances permit, an accredited organization should monitor and regulate chiropractic centers, especially private centers without a license in developing countries, and all chiropractors should receive standardized training to get a vocational certificate before practice. (3) Some patients who have neck pain often seek help from chiropractors to relieve their symptoms, and chiropractors should be aware of the risk of cervical dissection and exclude those clients so as not to aggravate cervical dissection by chiropractic manipulation. (4) Clients who receive chiropractic cervical manipulation should be informed about the potential risk, and if they develop neurological symptoms, they should go to see a doctor for early diagnosis and treatment.
Conclusion
Chiropractic manipulation may potentially lead to dissection and stroke. Most patients have favorable outcomes if diagnosed early and receive timely treatment, but serious sequelae may occur, including death. Raising awareness and education on this potential relationship is important to improve the safety of cervical chiropractic manipulation for patients.
Footnotes
Author contributions
Y.C. and M.M. drafted the manuscript; S.Y., W.W., W.L. and G.C. diagnosed and treated the patients; Z.H. analyzed the cases; K.O. provided the radiology images; M.M., T.N.N. and J.W. analyzed the cases and provided critical revision of the manuscript; Y.C. and W.W. collected the data; All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval by a research ethics committee was not required.
Informed Consent
All patients included in this study consented to the publication of the case report.