
Abstract
Thoracic Outlet Syndrome (TOS) is a rare condition caused by compression of the neurovascular structures of the thoracic outlet. Patients with TOS are found to have a greater prevalence of supernumerary or abnormal first ribs compared to the general population. Symptoms can sometimes be incited by a neck injury, especially in patients with abnormal cervical anatomy. This case report highlights a unique patient with bilateral cervical ribs who presented with complicated symptoms following a neck injury who required a series of surgical interventions to improve.
Introduction
Thoracic Outlet Syndrome (TOS) is a rare condition that results from compression of the neurovascular bundle within the thoracic outlet—a confined space above the first rib and behind and under the clavicle. 1 Different classifications of TOS exist depending on the neurovascular structure being compressed: arterial, venous, or neurogenic. The most common of these variants is neurogenic TOS, with an incidence of well over 90%. 1 This form of TOS results from irritation to the brachial plexus which can present with pain, paresthesia, and occasional paralysis of the affected extremity.
Treatment strategies for neurogenic TOS involve conservative treatment via physical therapy first and escalation to surgery whenever physical therapy fails to improve symptoms. As noted in previous studies, symptomatic improvement can be expected in a large percentage of patients undergoing surgery for neurogenic TOS, with a strong correlation between patient-rated outcomes and percentage decline in the QuickDASH score. 2 It is important to note that patients with TOS are often found to have a greater prevalence of cervical ribs compared to the general population—these ribs are more commonly found to be unilateral rather than bilateral.3,4 Given the rarity of bilateral symptoms in the general population, this case report will highlight a unique patient with bilateral cervical ribs who presented with complicated symptoms following a neck injury, requiring a series of surgical interventions to improve.
Case Presentation
This patient is a 32-year-old female with no significant past medical history who presented to the clinic with numbness and pain in the neck and temporary paralysis of her left arm, as well as occasional episodes of numbness in her right arm following exercise and weight lifting. Three months earlier, she had participated in a CrossFit competition. During the weightlifting part of the competition, her left arm became temporarily paralyzed and the weakness and numbness persisted after the competition. She was seen by an orthopedic surgeon who performed an MRA/MRI which showed bilateral cervical ribs with compression of her left subclavian artery on abduction and an acute disc extrusion at C5-C6 with encroachment on the left C6 nerve root. Given the immediacy of the patient’s symptoms during the competition along with an absence of similar neuromuscular symptoms in the patient’s past, it was deemed for this extrusion to be acute in nature rather than chronic by the orthopedic surgeon (Figure 1). (a) Left cervical rib; (b) Right cervical rib; (c) C5-C6 disc extrusion; (d) MRA (arms down) without occlusion of the subclavian arteries; (e) MRA (arms up) with occlusion of the left subclavian artery.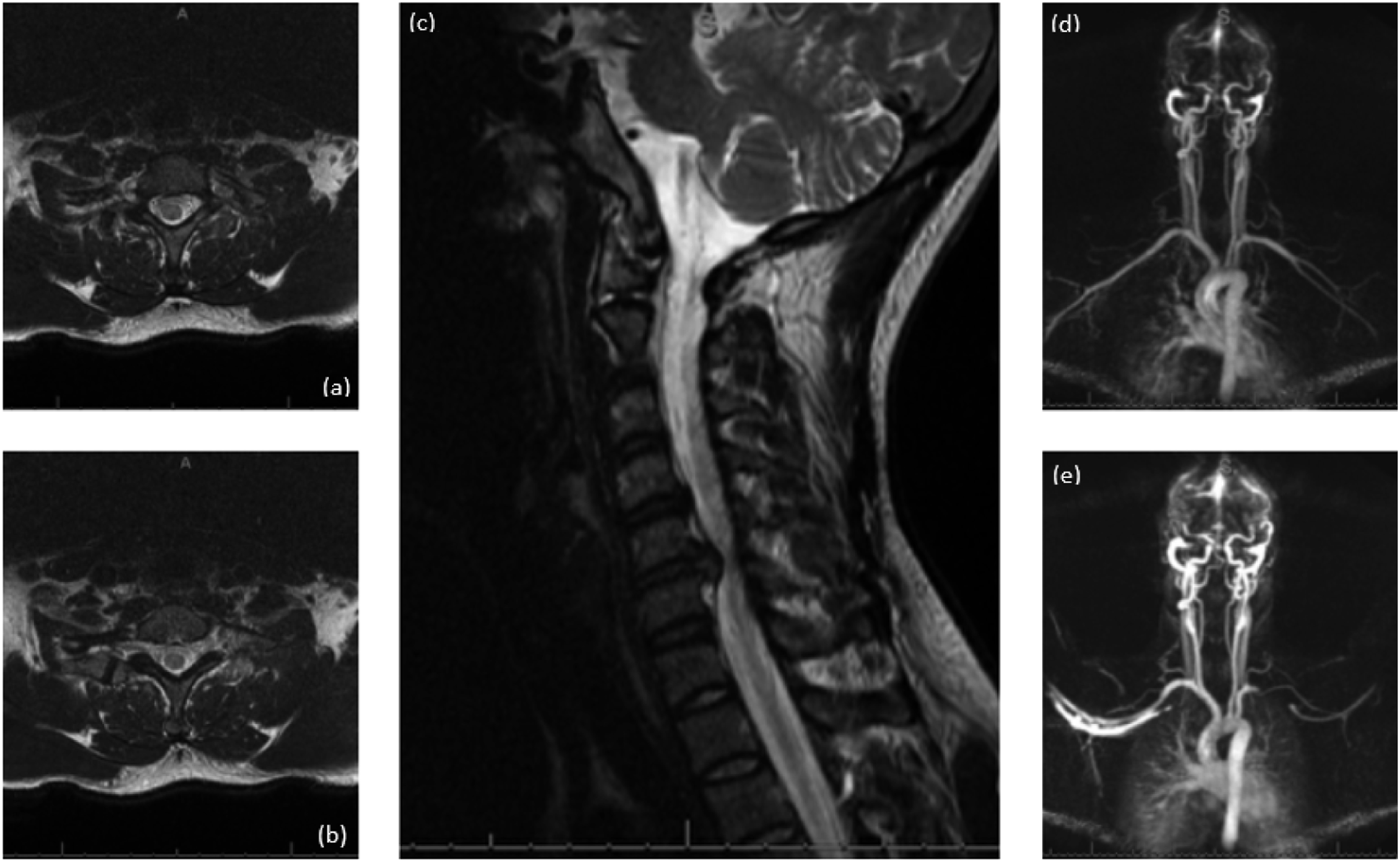
She was recommended massage and physical therapy, which did not improve her symptoms. Upon presenting to our vascular surgery clinic, in addition to the previously mentioned symptoms, she also described ischemic symptoms on abduction in her left upper extremity with pain in her hand and forearm. On physical exam, she had bilateral large anterior scalene muscles with palpable cervical ribs bilaterally. She also had decreased strength in the left ulnar distribution, bilateral subclavian bruits with arms abducted, bilateral positive Adson’s tests, and a positive elevated arm stress test (EAST) on the left in 15 seconds. Her signs and symptoms were consistent with left arterial and neurogenic TOS with concomitant C5-C6 disc extrusion.
Initially, she underwent a discectomy and decompression of her herniated disc with neurosurgery, given her symptom acuity and history of paralysis. In addition, it was also deemed appropriate to perform the neurosurgical intervention first to minimize the risk of unintended spinal cord or nerve damage related to the positioning during the procedure with vascular surgery. Following the discectomy and decompression, the patient had partial improvement with persistence of weakness and numbness in the ulnar distribution in her left upper extremity. As a result, upon complete recovery following her disc surgery, she underwent left transaxillary first rib resection and anterior scalenectomy with left cervical rib excision. An incision was made just below the axillary line between the pectoralis major muscle and latissimus dorsi muscle. The first rib was then elevated with a rib elevator for complete visualization of the cervical rib and the first rib and anterior scalene muscle insertion were resected along with the subclavius tendon. Following resection, additional space was created within the thoracic outlet using the rongeur on both the cervical rib and the remaining portion of the first rib. Following the procedure, the patient’s postoperative course was uneventful and she continued physical therapy until her next follow-up visit.
At her 3-month post-op visit, the patient had recovered uneventfully from her left rib resection but was still having pain and discomfort on the right side. She continued with massage therapy and physical therapy with a return visit in 6 months. After 6 months, the patient was still having symptoms in her right arm. On physical exam, she was found to have a palpable right cervical rib with tenderness to touch, a right subclavian bruit on abduction, a positive Adson’s test, and now a positive EAST on the right. Her left side had otherwise recovered uneventfully with a full range of motion without pain or discomfort. She was also unable to drive or work on her computer without pain or discomfort on her right side. As a result, given these lifestyle limitations, we opted for a right transaxillary first rib resection and anterior scalenectomy with cervical rib excision in the same fashion as the contralateral side. Following this surgery, her immediate postoperative period was uneventful with daily improvement in range of motion and gradual resolution of her extremity pain and discomfort (Figure 2). Resected right first rib along with portions of the fused cervical rib.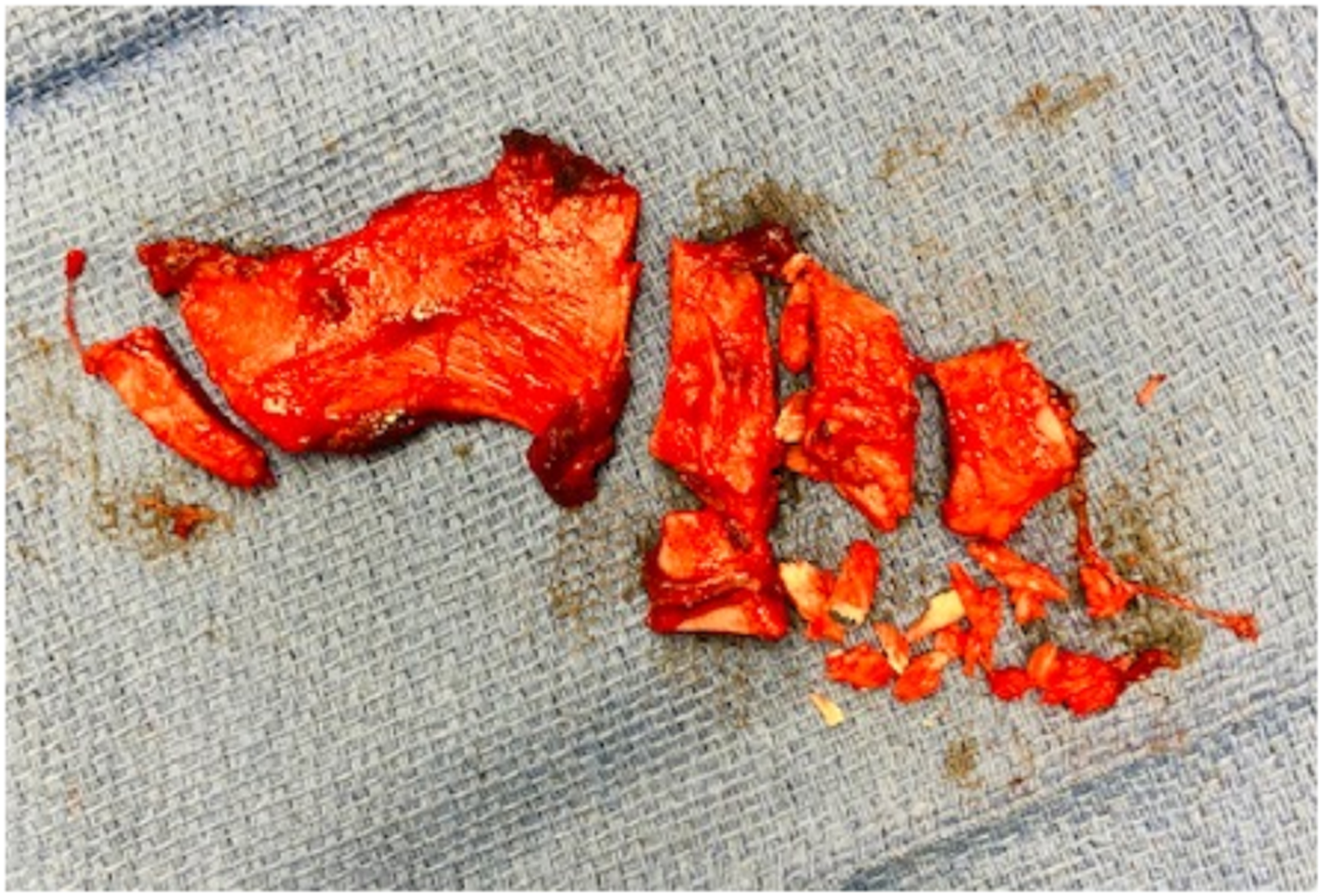
Discussion
Different types of TOS exist depending on the neurovascular structure being compressed. Arterial TOS is caused by compression of the subclavian artery, most often from a cervical rib or anomalous first rib, which results in distal ischemia to the affected limb. 1 Incidence of arterial TOS is fairly rare and accounts for no more than 1% of cases. 1 Similarly, venous TOS results from compression of the subclavian vein, which can present either with or without thrombosis. This is the second most common type of TOS variant, with an incidence of about 5%. 1 The last and most common type of TOS, with an incidence of well over 90%, is neurogenic TOS. 1 This results from brachial plexus compression usually from scarred scalene muscles secondary to neck trauma or supernumerary ribs. 1
Different forms of TOS variants can sometimes coexist with one another. According to a previous study by Chang et al., different forms of TOS can coexist especially in patients with large cervical ribs. 5 As noted in this study, 8 out of 58 patients with TOS had cervical ribs that caused both neurogenic and arterial symptoms. 5 Furthermore, in a separate study by Likes et al., a small subset of patients had an arterial component in addition to their neurogenic symptoms. 6 According to this study, patients with concomitant arterial and neurogenic TOS tended to be younger and with a shorter duration of symptoms at presentation compared to patients with neurogenic TOS alone. 6 Similar to our patient in this case, patients with concomitant symptoms did not improve with physical therapy alone and often required surgery for complete resolution of symptoms. 6 Such failure in symptom resolution with physical therapy alone is likely attributed to chronic compression and damage to the subclavian artery from abnormal cervical anatomy.
Quality of life is highly variable in patients with neurogenic TOS. Symptoms can range from mild with occasional pain and paresthesia to severe with debilitating paralysis. Milder forms can sometimes be treated with physical therapy alone but when symptoms persist, surgery is often curative in these patients. According to a study by Rochlin et al., about 30% to 40% of patients with neurogenic TOS do not respond to physical therapy alone and will require surgery for symptomatic resolution. 7 Surgical decompression was shown to significantly improve quality of life in both the short and long term in these patients. 7 Some studies have shown symptomatic improvement in a large percentage of patients undergoing surgery for neurogenic TOS, with a strong correlation between patient-rated outcomes and percentage decline in the QuickDASH score. 2 When residual symptoms persist, these are often minor and commonly affect the shoulder, neck, and upper extremity.2,7 As seen in our patient in this case, minor postoperative symptoms are often preferable over their debilitating preoperative limitations, making surgical intervention essential for proper management of these patients.
Regardless of the site of compression, patients with TOS are found to have a greater prevalence of cervical ribs compared to the general population. Based on previous studies, the prevalence of cervical ribs is .74%, with variation based on the sex and race of the population. 3 Females tend to have a higher prevalence of cervical ribs compared with males (1.09% and .42%, respectively). 3 The prevalence of bilateral cervical ribs is an even more rare occurrence with an overall prevalence of .14%. 4 Compared to the general population, patients with TOS are found to have a higher prevalence of supernumerary ribs, with values ranging from 8.5% in some studies to 29.5% in other studies.4,8
The presence of cervical ribs and anomalous first ribs can predispose patients to develop TOS after a neck injury. Neck trauma is the most common cause of neurogenic TOS, with symptoms resulting in as high as 80% of patients. 9 Similarly, vascular compression of the subclavian vessels can often result from traumatic injury to the neck, especially in patients with underlying anatomical variations. 10 This is thought to result from narrowing of the scalene triangle due to spasm of the scalene muscles, in addition to inflammation and scarring of structures surrounding the neurovascular bundle within the thoracic outlet. Given the overall rarity of arterial TOS, most of the documented cases of TOS after trauma seem to be neurogenic in nature.
There have been very few documented cases of TOS after acute cervical disk disease. According to a study by Kai et al., some patients with disc injury display chronic residual symptoms even after the resolution of their cervical disc disease. 11 This finding likely suggests that TOS may be combined with cervical disc disease, rather than being caused by cervical disc injury itself. 11 Many of the patients with residual symptoms in this study had disc injuries at the level of C5-C7, similar to our patient in this case. These findings suggest that the development of TOS is a multifactorial process that necessitates both the right circumstance, such as an abnormal cervical anatomy, and the proper inciting factor, such as cervical injury and inflammation. Appropriate staging of conservative therapy and surgical intervention is essential for excellent results.
Conclusion
We presented a rare case of bilateral TOS following neck trauma. This case illustrates how both neurogenic and arterial TOS can present as a result of neck injury in patients with abnormal cervical anatomy. It also demonstrates how compressive symptoms can persist even after a patient’s primary cervical disc injury is resolved. Given the prominent and disabling symptoms of neurovascular compression, one must consider TOS as a potential diagnosis in the long-term follow-up of these patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.