
Abstract
Introduction
Arterial aneurysms of upper extremities are rare. While lower extremity aneurysms account for approximately 90% of peripheral aneurysms, upper extremity aneurysms are only 1%.1-4 True aneurysms of the brachial artery are very uncommon, with a reported incidence estimated to be around .17% of the population. 5
The increasing prevalence of invasive procedures such as arterial lines, dialysis access, and cardiac catheterizations via the upper extremity, can lead to a higher number of complications, with brachial artery pseudoaneurysms being observed more frequently. 6
The aetiopathogenesis of true aneurysms is multifactorial with a definite role of genetic predisposition, atherosclerosis, smoking, hypertension, and dyslipidemia. 7 Blunt repetitive trauma is the most common cause of true upper extremity arterial aneurysms, usually related to occupational or recreational activities and located in the ulnar artery. 1 True brachial artery aneurysms have also been reported on patients with previous arteriovenous fistula surgery for dialysis,8,9 and only a few cases of true idiopathic brachial artery aneurysms have been described in the literature.3,10,11
Patients with brachial artery aneurysms are often symptomatic and may present a palpable mass, pain or paresthesias in the arm. If not diagnosed promptly, acute limb ischemia might occur due to distal embolization. 9 Definitive diagnosis can be confirmed with Doppler ultrasonography, computed tomography angiogram (CTA), magnetic resonance angiography (MRA), or selective angiography, although this is usually reserved for treatment planning.
Herein, we present a case of a 65-year-old woman who presented with pallor and pain of her left arm and hand, and a true arterial brachial aneurysm was diagnosed and successfully treated. A review of the literature is performed.
Case Report
A 65-year-old woman presented with a transient episode of pallor and acute spontaneous pain in her left forearm and hand. Her medical history only included systemic arterial hypertension under treatment with valsartan/amlodipine 15 mg/5 mg daily. There was no history of infectious diseases, trauma, or punctures in her left arm. She was a non-smoker and had no history of drug abuse. The patient denied any family history of vasculitis or genetic diseases. On physical examination, there was a pulsatile mass in the proximal segment of the left forearm near the elbow with minor erythema and slight tenderness. She had palpable, symmetrical radial and ulnar pulses and did not have any heart murmurs.
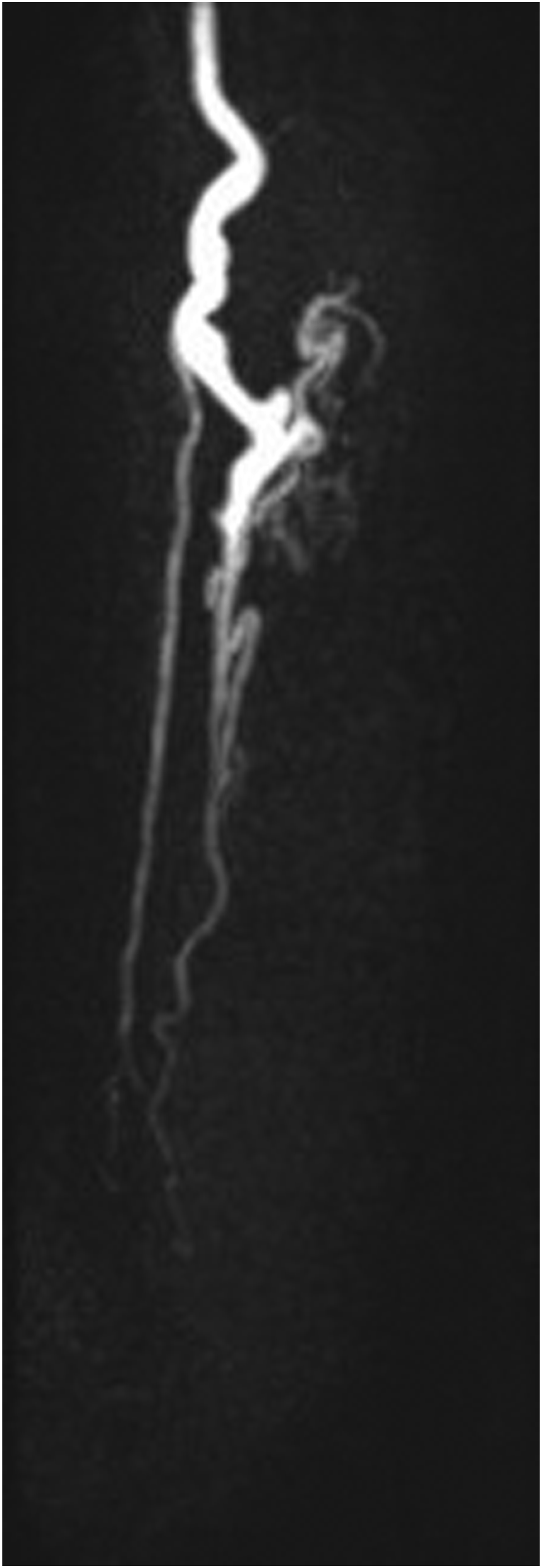
The patient was started on dabigatran 150 mg PO bid to prevent further ischemic episodes. An echocardiogram was performed which ruled out valvular pathology or endocarditis. An upper extremity arterial doppler ultrasound was performed showing a 23 mm diameter fusiform aneurysmal dilatation of the distal brachial artery with turbulent flow with intraluminal thrombus Doppler ultrasound images of the left upper extremity showing fusiform aneurysmal dilatation of the brachial artery with a diameter of 23 mm. A partially occupied intraluminal echogenic material is seen, allowing a 12 mm patent lumen in the proximal third of the forearm. Magnetic resonance angiography showing an 18 mm aneurysm of the distal brachial artery, which extended to the bifurcation. White arrow showing the aneurysm. Preoperative angiography images. (A) Upper arm with brachial artery with fusiform aneurysm (white arrow). (B) Forearm with radial artery (white arrow), interosseus artery (black arrow), ulnar artery (white triangle). (C) Hand with arterial vasculature showing an ulnar dominant artery (white triangle).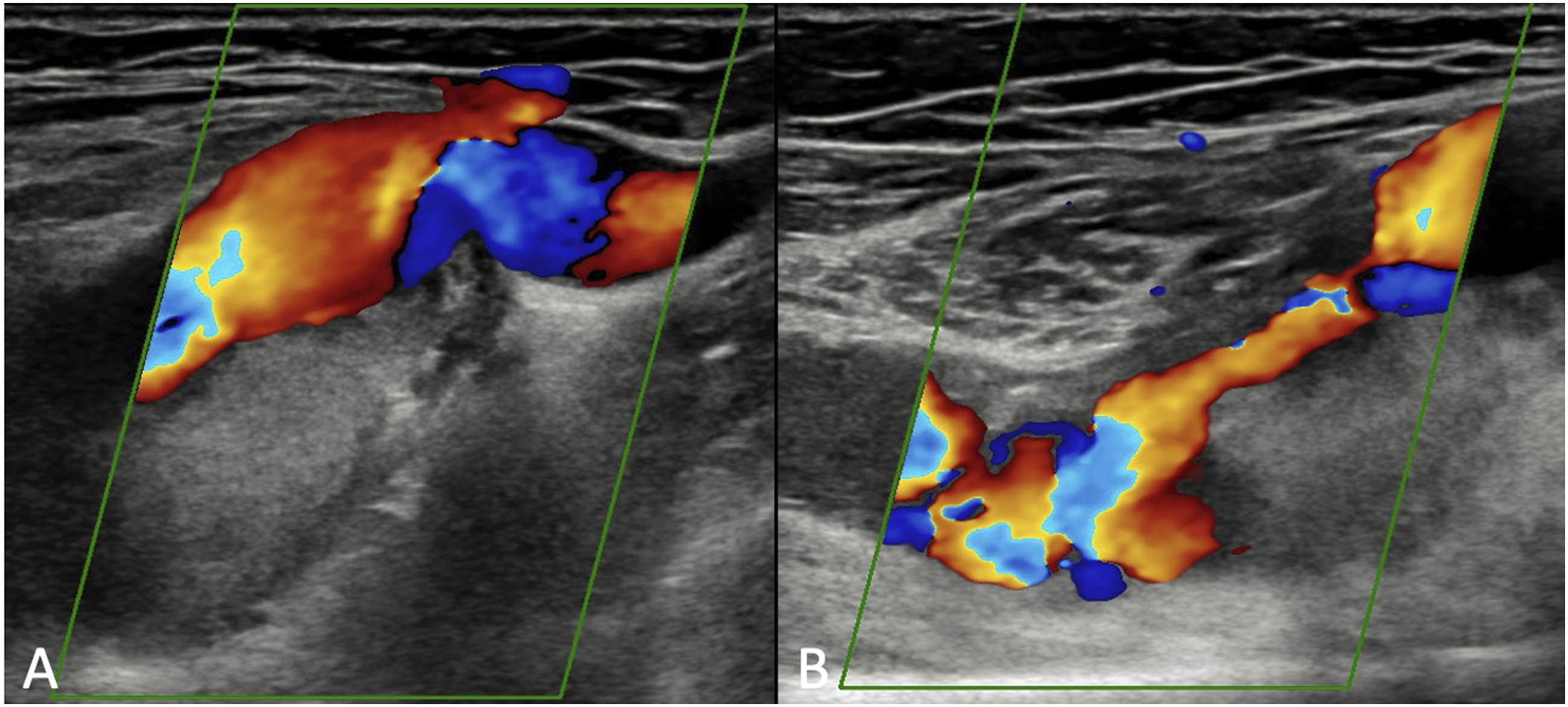

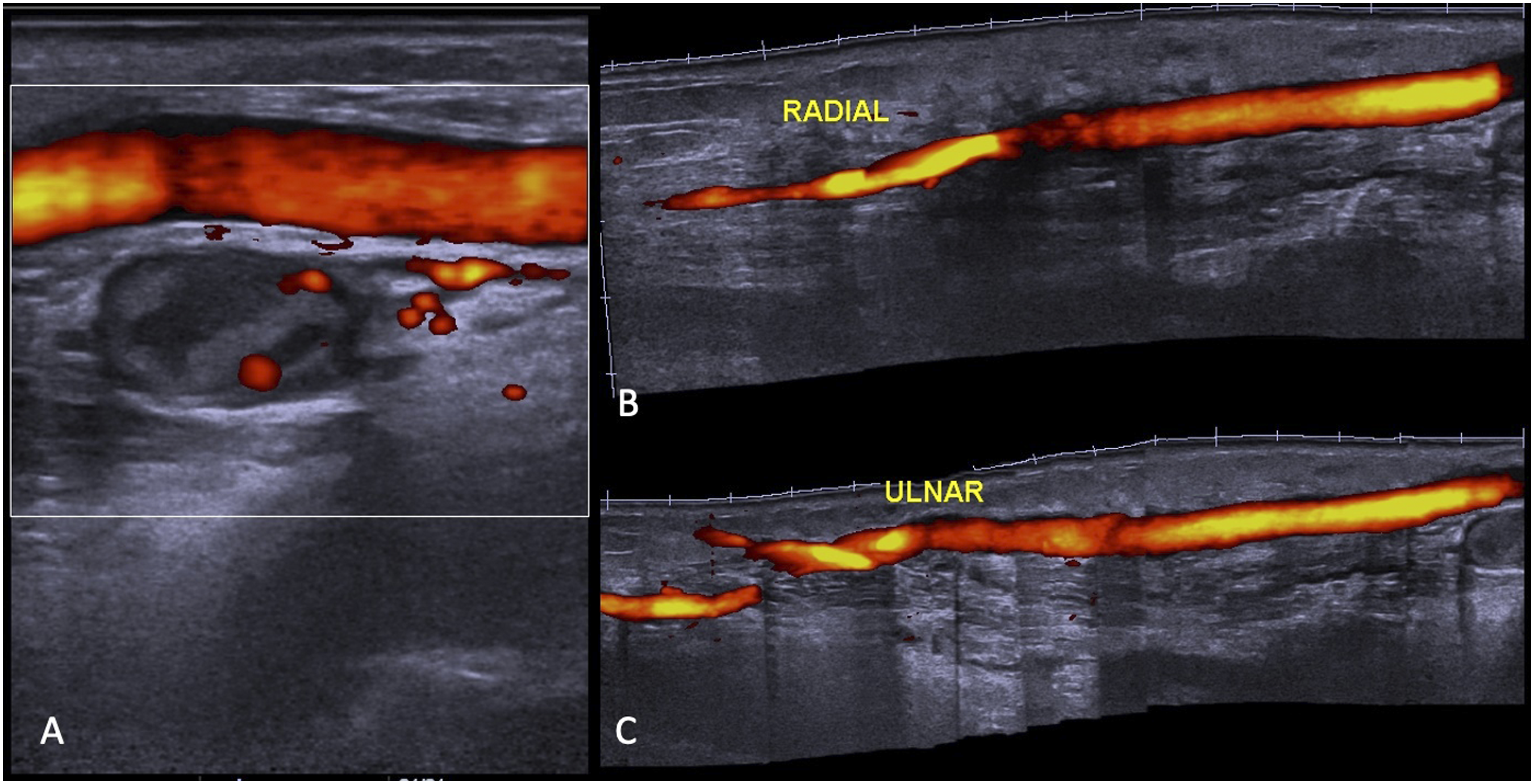
The patient was taken to the operative room for an open repair. One incision was made in the distal left arm and another on the proximal forearm. A 20 x 60 mm fusiform aneurysm of the distal brachial artery was found extending from the cubital fossa to the upper forearm. A brachial artery to radial and ulnar arteries bypass with reversed saphenous vein was performed Surgical sketch. A brachial artery to radial artery side-to-side bypass with great saphenous and a saphenous graft to ulnar artery side-to-end bypass. Aneurysm sac embolization with Gelita-spon ® (Gelita Medical, Eberbach, Germany). UA: ulnar artery; IA: interosseous artery; RA: radial artery. Postoperative angiography images. (A) Brachial artery with exclusion of the aneurysm sac. (B) Adequate perfusion to radial and ulnar artery from saphenous graft. (C) Arterial vasculature of the hand. Doppler ultrasound images from 3 months follow up. (A) Saphenous graft with adequate patency. (B) Radial artery (C) Ulnar artery. CT angiogram from 3 months follow up.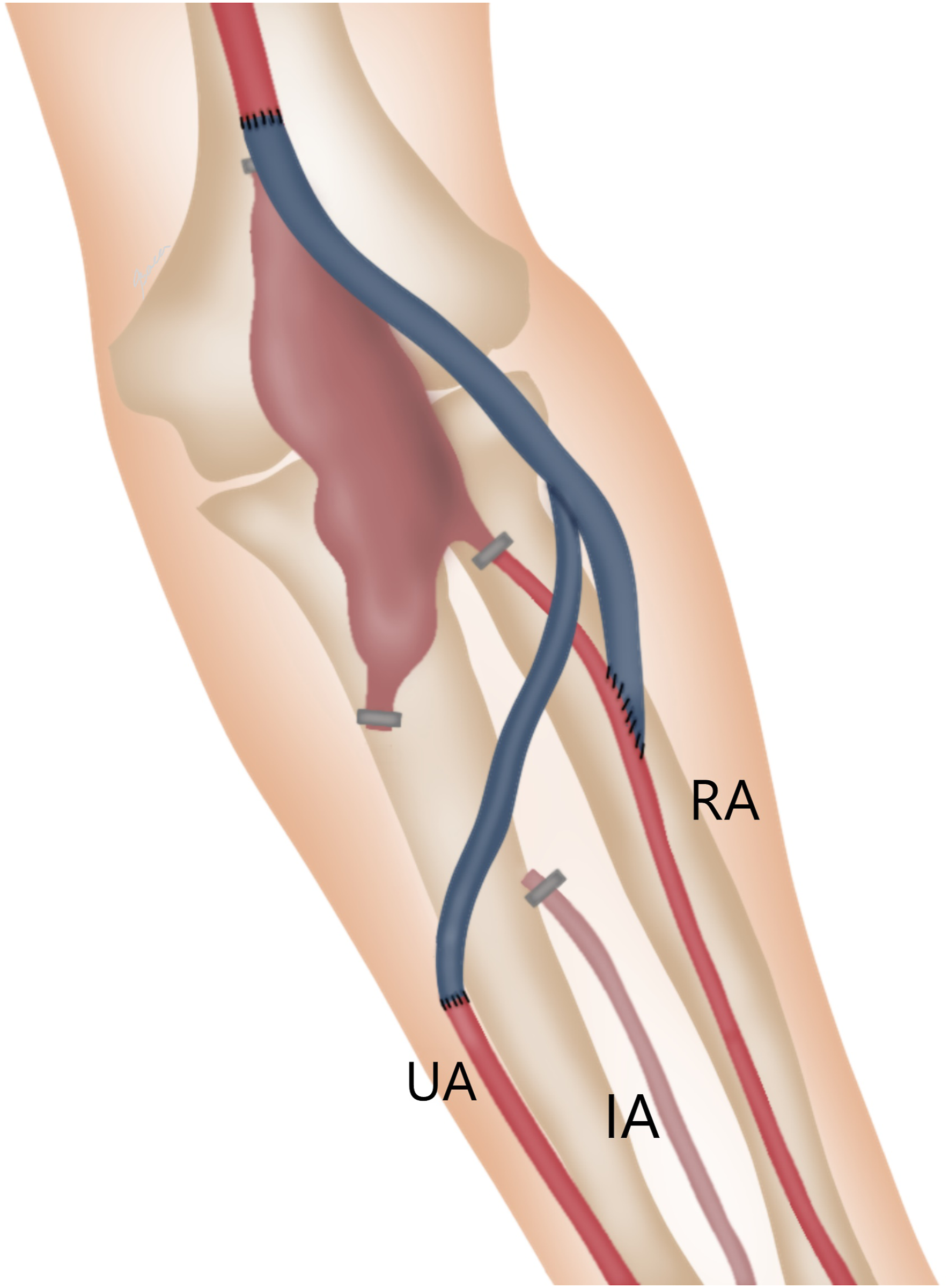


Discussion
An arterial aneurysms is a dilatation of the vessel greater than 50% of the normal diameter. 12 True aneurysms are rare in the upper extremities, 5 and can be found in descending order of frequency in the subclavian, axillary and brachial arteries, and much less in the ulnar or radial arteries. 2
The Cleveland Clinic identified only one brachial arterial aneurysm out of 581 procedures performed on brachial arteries over 11 years. 5 Likewise, the Mayo Clinic, after reviewing all true upper extremity aneurysms cases in a two-decade period, identified only two brachial artery aneurysms. 1
Upper extremity aneurysms are usually secondary to other conditions such as trauma, 13 infection, 14 thoracic outlet syndrome, 15 previous arteriovenous fistulae, 8 vascular malformations16,17; arteritis such as giant cell arteritis polyarteritis nodosa and Takayasu’s arteritis, 18 and connective tissue disorders such as Ehlers–Danlos or Marfan syndrome, 19 among others, 20 with the vast majority being false or pseudoaneurysms. Mycotic upper extremity aneurysms have also been reported. Leon et al 21 reviewed 149 upper extremity aneurysms, of which 52 compromised the brachial artery, mainly affecting males with an average age of 41.4 years (range 23-86 years). Most cases were secondary to intravenous drug abuse followed by endocarditis. In our patient, we ruled out an infectious etiology after no history of fever, elevated while blood cell count, elevated c-reactive protein, nor other factors suggesting a mycotic origin were found. In addition, an arteriovenous malformation was ruled out on multiple imaging studies. Finally, other etiologies were also ruled out since the patient had no history of trauma or iatrogenesis in that arm.
Most of the time, the diagnosis of arterial brachial aneurysm is made due to the presence of a pulsatile mass or compression symptoms, such as pallor, pain or paresthesia. 22 Other less frequent complications include venous edema, skin erosion, or compartment syndrome.22,23 Our patient presented with transient ischemic symptoms, and because she was treated promptly, serious complications were avoided.
The differential diagnosis of arterial brachial aneurysm includes arteriovenous malformation, lymphadenopathy, lipoma, hematoma, abscess, and pulsating tumors such as bone sarcoma, and osteoclastoma. 23 The diagnosis can be confirmed by images studies such as CTA, MRI, selective arteriography, or Doppler ultrasound. The latter being the first diagnostic approach, but findings can be misleading as it is operator-dependent. 24 Therefore, CTA or MRA are preferred methods for diagnostic evaluations of upper limb vascular diseases due to their high-image resolution capacity. 25
Bautista-Sanchez et al 24 recently performed a systematic literature review finding only 35 cases of true brachial aneurysms reported, excluding patients with a history of arteriovenous fistula. Most of the patients were male (57%), and median age was 52 years. Pulsatile mass was the most common manifestation, and mean aneurysm size was 32.8 mm (range: 9-70 mm). The most common etiology was idiopathic (74.2%), followed by infectious and atherosclerotic, accounting for two cases each (5.7%). It was equally encountered in both sides, accounting for 17 (48.5%) cases each side, respectively.
Various treatment modalities have been reported ranging from conservative treatment (antibiotics) to excision and arterial ligation or reconstruction with an end-to-end anastomosis, vein graft interposition, or vein patch. Surgical or endovascular treatment should be offered immediately after diagnosis to avoid ischemic complications due to distal embolization, the former being the treatment of choice due to good patency and long-term results, with low morbidity rates.3,9 In the case presented, revacularization with bypass was performed to avoid new episodes of ischemia due to embolism. Bypass with greater saphenous vein interposition graft has been the most frequently employed treatment.2,3,23-27 We decided to use the right great saphenous vein in this patient, because it was the largest conduit available. The cephalic vein 14 or the basilic vein 28 have also been used with the theoretical advantage of avoiding an incision in lower extremity and preserving the saphenous vein for possible future vascular reconstructions. Other treatment options include primary end-to-end anastomosis 29 or PTFE interposition. 17 Endovascular treatment has exceptionally been used. Yigit et al 30 reported a 31-year-old female with Behçet disease with a 26 x 16 mm brachial artery aneurysm, that was treated using two covered stents. There are no randomized control trials available in the literature regarding the best treatment for this condition, due to the exceptionality of the disease; however, the most broadly accepted therapeutic intervention based on retrospective data and expert opinion includes operative resection of the aneurysm with interposition vein grafting. 9 Moreover, the overview and management of true arterial brachial aneurysms has been extrapolated from case reports and case series regarding treatment of false aneurysms, or others secondary to AV fistulas, trauma, infection, or iatrogenic causes. Further studies describing true idiopathic brachial artery aneurysm are needed for better understanding this disorder.
In conclusion, patients with brachial aneurysms should be operated on because of the risk of limb loss due to possible distal embolization. Revascularization with autologous saphenous vein graft and exclusion of the aneurysm with local embolization is a good treatment alternative in a patient with symptomatic brachial aneurysm with distal embolization as the clinical case described.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.