
Abstract
Purpose
To describe the efficiency of the candy-plug technique using an Excluder aortic extender and obtain optimal aortic remodeling.
Case
A 46-year-old male patient had a history of acute type B aortic dissection and progressive dilation of the descending aorta (53 mm diameter) with a patent false lumen. He was treated with the candy-plug technique, using an Excluder aortic extender of 32-45 mm was placed and a 16-mm Amplatzer Vascular Plug II. No technical complications were observed in the patient. Good aortic remodeling was observed after 6 months, CT showed complete thrombosis of the false lumen and reduction of the maximum perpendicular diameter of the descending aorta from 53 to 47 mm. The diameter of the other proximal zones of the descending aorta was 45-47 mm, and the Excluder aortic extender changed into an elliptical shape. This is the first report of good aortic remodeling with an elliptical shape by performing the candy-plug technique.
Discussion
The candy-plug technique using an Excluder aortic extender is an improved method for occluding the false lumen as it provides improved aortic remodeling. The 2 indications for this surgery are limited. A large entry point in the descending abdominal aorta that is more peripheral than the candy-plug position must be visible on contrast-enhanced CT and the false lumen is not too large. We consider candy-plug placement in the true lumen central to the TEVAR to avoid occluding the artery of Adamkiewicz, since we have to avoid the thrombosis of the peripheral false lumen where a candy-plug was placed. Since it is unclear whether long-term results are satisfactory, we must continue to study chronic aortic type B dissection.
Introduction
Thoracic endovascular aortic repair (TEVAR) is useful for closing the primary entry in patients with chronic type B aortic dissection. However, true lumen remodeling cannot be achieved in some patients, since retrograde blood flow from the distal persists, which may cause false lumen enlargement. Here, we report a patient with chronic type B dissection for whom the candy-plug technique provided good remodeling of the true lumen. Patient consent for publication of this report was obtained before submission.
Case Presentation
A 46-year-old man who presented with back pain was referred to our hospital. Computed tomography (CT) showed aortic dissection, ranging from the distal arch of the aorta to the common iliac artery and a patent false lumen. The location of re-entry was found to be in the right external iliac artery. The maximum perpendicular diameter of the distal arch was 43 mm (Figure 1A). The true lumen of the dissected aorta was narrow; however, the brachial index of the ankle was normal at 1.05. The patient was diagnosed with acute type B aortic dissection, and anti-hypertensive therapy was initiated accordingly. A CT performed 4 months later showed rapid expansion of the false lumen, with a maximum perpendicular diameter of 53 mm (Figure 1B and C). The treatment options were either descending aortic replacement or TEVAR. He had severe obesity (BMI 33); therefore, performing descending aortic replacement involves a higher risk. Hence, TEVAR was performed using the candy-plug technique to close the entry site, maintain the diameter of the true lumen, and occlude the false lumen. Preoperative contrast CT (A) At onset of aortic dissection: maximum perpendicular diameter was 43 mm (B) four months after the onset: maximum perpendicular diameter was 53 mm (C) 3D CT four months after the onset.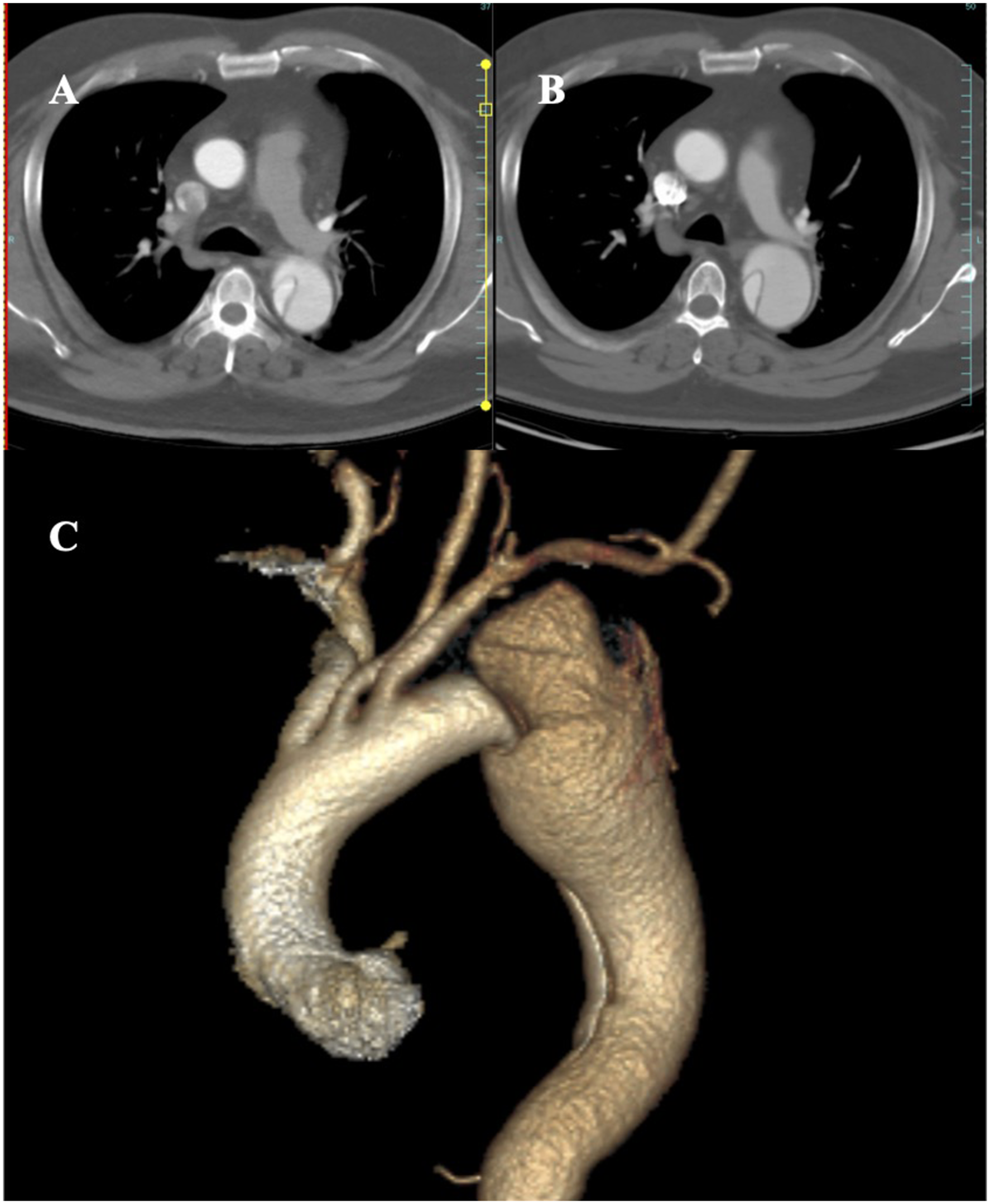
Surgical Procedure
The patient was placed in the supine position under general anesthesia. First, we used the Excluder aortic extender to create the candy-plug, as described by Ogawa et al.
1
Ogawa created the candy-plug by using an Excluder aortic extender. The candy-plug is created as follows: A durable polyester suture is inserted through the center of the Excluder aortic extender and then drawn around the extender to form a diameter-reducing tie, followed by complete ligation with ∼10 mm of clearance.
1
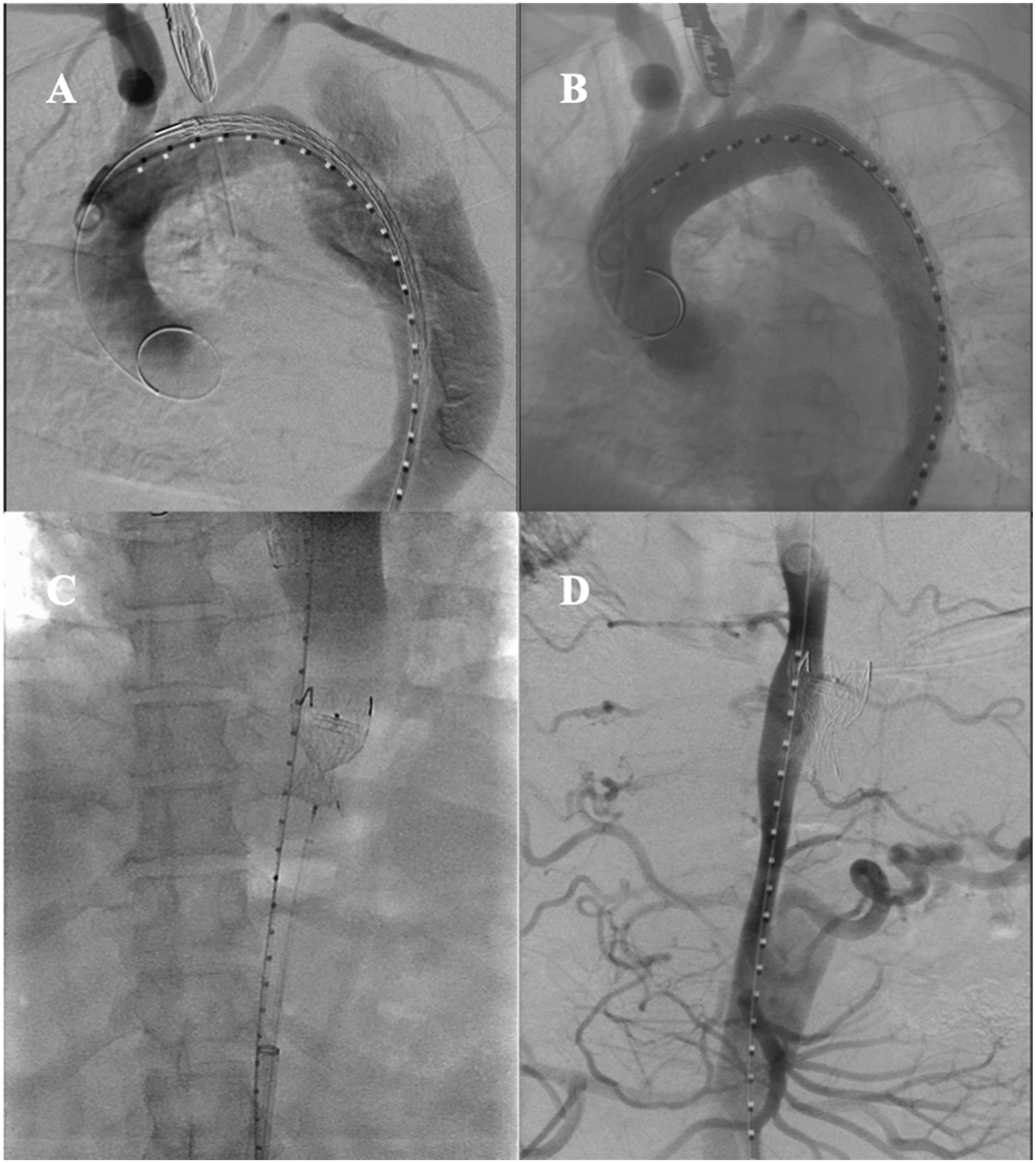
Briefly, an Excluder aortic extender of 32-45 mm (W.L. Gore & Associates, Flagstaff, AZ, USA) was narrowed by ligating it with a 2-0 Ethibond (ETHICON, NJ, USA) suture at the center of the body of the inner cylinder of a 20-Fr Dryseal Flex Introducer Sheath (W.L Gore & Associates Flagstaff, AZ, USA) to create an hourglass-shaped stent extender, the candy-plug. (Figure 2) Before the operation, we checked the diameter of the false lumen and selected an appropriate size of 32-45 mm. The bilateral inguinal regions were obliquely incised to expose the femoral arteries. A guidewire was inserted into the left femoral artery, followed by a 20-Fr introducer sheath. A 28-mm C-TAG stent graft (W. L. Gore & Associates) was placed into the distal side of the left subclavian artery to cover the primary entry of the distal aortic arch. The guide wire for the candy-plug was inserted into the right femoral artery via the re-entry of the right external iliac artery, and the candy-plug was placed in the false lumen at the 10th lumbar vertebra level, where the proximal side at the large re-entry of the 8th lumbar vertebra level did not close the artery of Adamkiewicz. A 16-mm Amplatzer Vascular Plug II (Abbott Laboratories, NY, USA) was deployed in the center of the candy-plug through a 6-Fr, 90-cm Destination guiding sheath (Terumo Medical, Shibuya, Tokyo). Aortography confirmed that no blood flow occurred between the primary entry site and the candy-plug of the false lumen, which indicated successful positioning of the thoracic stent graft and prevention of retrograde blood flow by the candy-plug into the false lumen of the aneurysm (Figure 3A-D). Candy-plug using the Excluder aortic extender. Digital subtraction angiography during the operation (A) Initial image. The false lumen has been contrasted from entry. (B) After TEVAR, the entry has been occluded. (C) Candy-plug was placed in the false lumen (D) After the candy-plug was placed, the false lumen was occluded by the candy-plug, and there was no retrograde flow in the false lumen.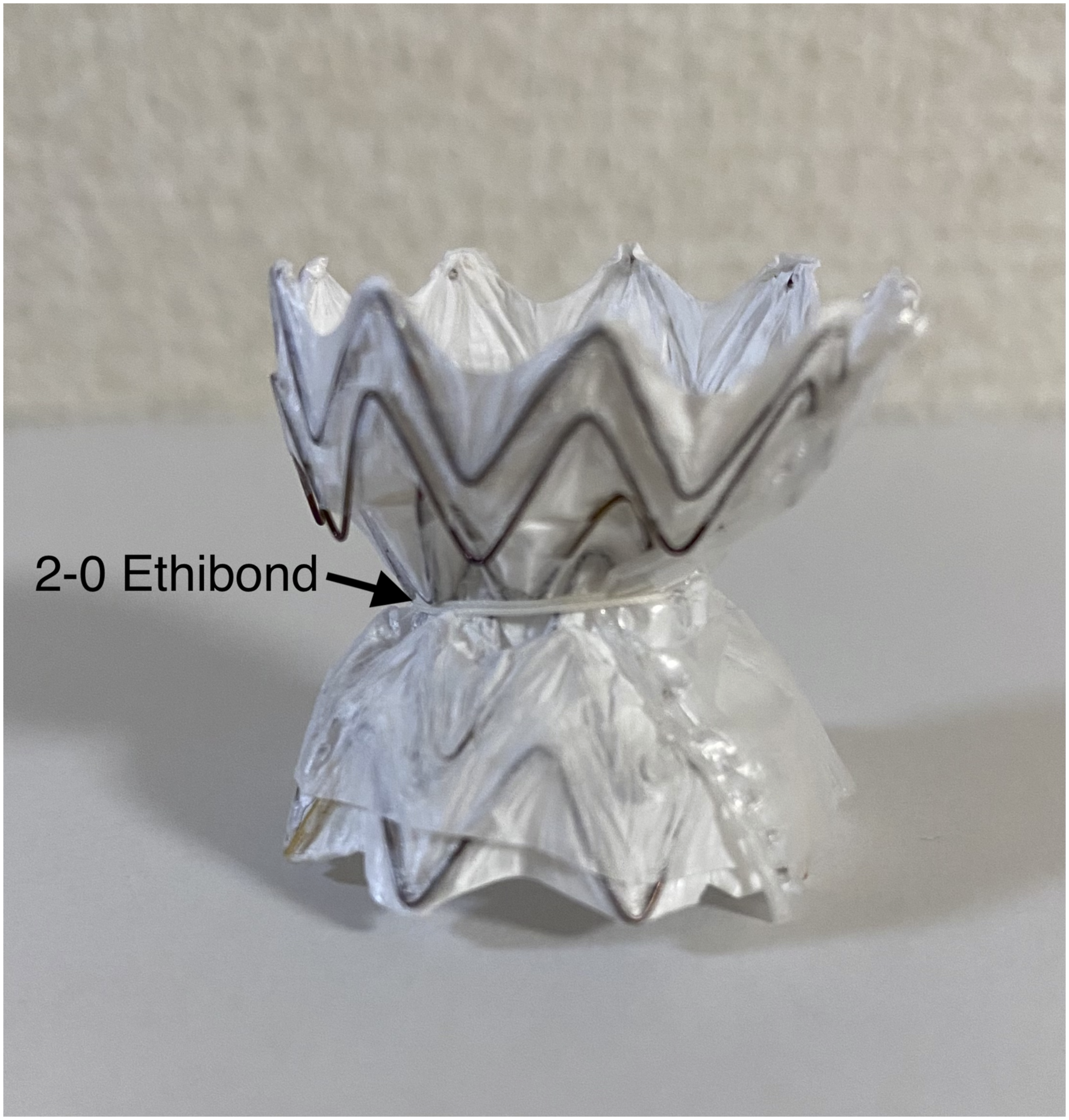
Postoperative Course
The postoperative course of the patient was good, without complications, and he was discharged 6 days after the procedure. Six months later, CT showed complete thrombosis of the false lumen and reduction of the maximum perpendicular diameter of the descending aorta from 53 to 47 mm (Figure 4A and B). The diameter of the other proximal zones of the descending aorta was 45-47 mm, and none of them had expanded. Postoperative contrast CT (A) CT at 3 days after surgery showed false lumen thrombosis at the proximal side of thoracic aorta (B) CT on 6 months after surgery showed reduced aortic diameter and enlarged stent graft.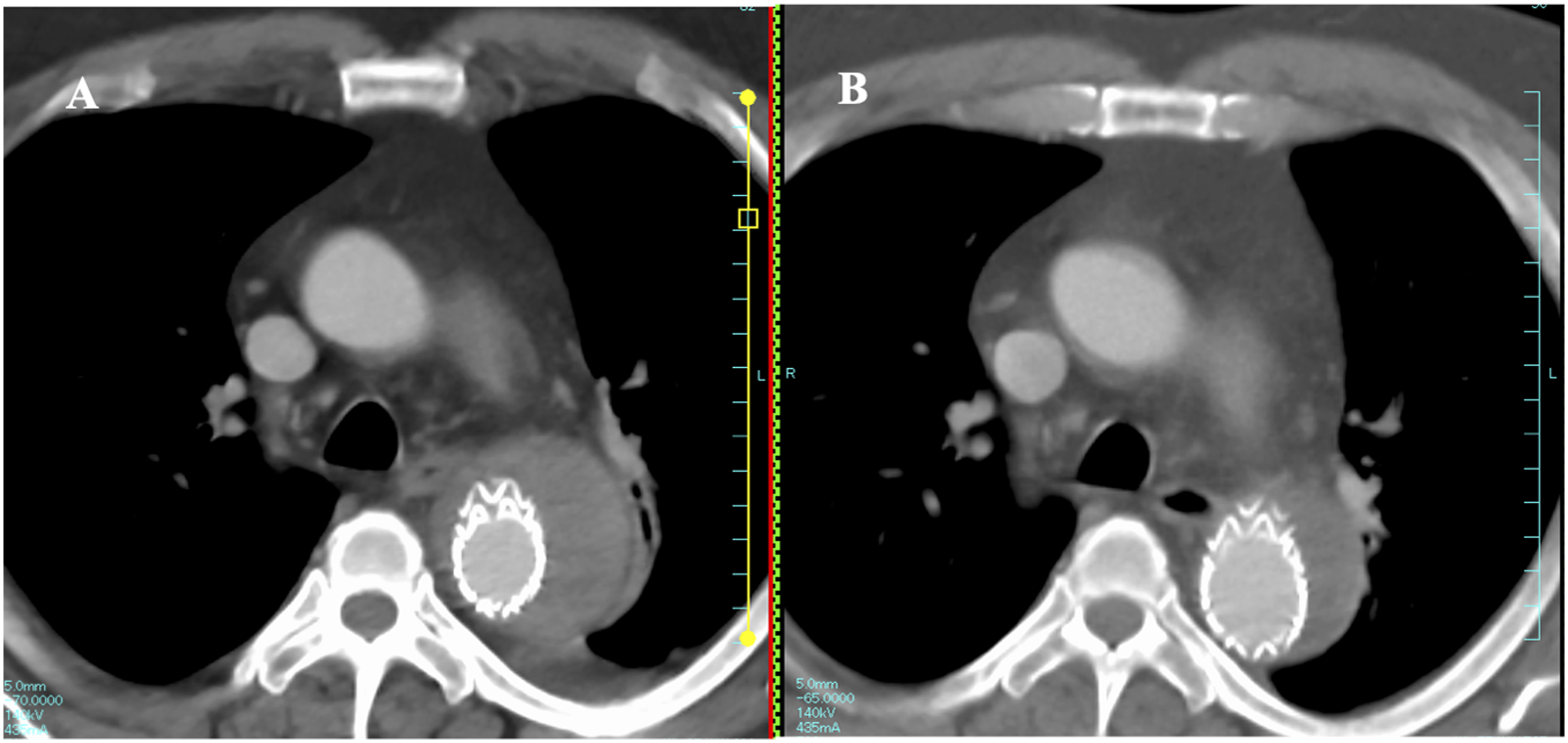
The false lumen on the central side of the location where the candy-plug was placed was completely thrombosed. At the 10th lumbar vertebra level, the shape of the candy-plug was deformed from a circular to an elliptical shape, with a corresponding circular change in the cross-sectional shape of the true lumen. The result was considered as good remodeling. (Figure 5A-C). Contrast CT (A) 3 days after surgery. The candy-plug is excluding the true lumen (B) 6 months after surgery. The true lumen is widened, and the candy-plug is excluded (C) 6 months after surgery 3D CT.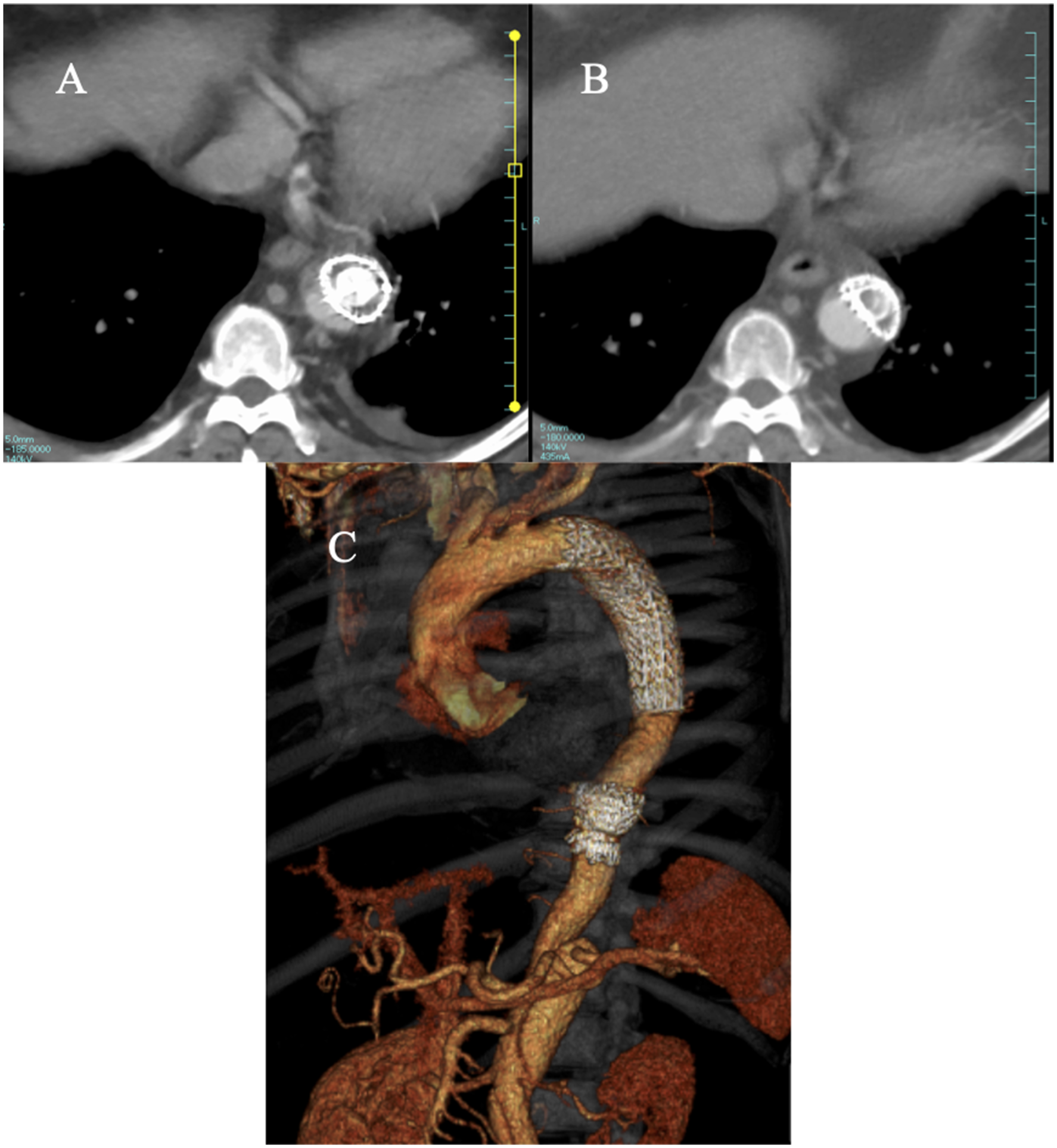
Discussion
Although the strategy for treatment of chronic type B aortic dissection is controversial, intermediate use of TEVAR is effective for preventing aortic diameter expansion. 2 However, residual retrograde blood flow to the false lumen after TEVAR leads to the risk of enlargement of the false lumen and inhibits aortic remodeling. As described by Kölbel et al., TEVAR in chronic type B aortic dissection for covering the proximal entry-tear alone was insufficient because it encouraged further false-lumen growth and high mortality risk at 3 years. 3 Thus, several techniques for preventing distal false-lumen back-flow were invented and have obtained good results. 4 Kölbel et al. described the KnickerBocker technique, in which a large-diameter stent graft was placed in the true lumen to promote thrombosis of the false lumen. 5
The original candy-plug technique reported by Kölbel et al. in 2013 used the Zenith TX2® TAA Endovascular Graft (Cook Medical, Bloomington, USA) to make the candy-plug. 6 The Candy-plug generation II,CP II (Cook Medical, Bloomington, US) can also be used in some cases. 7 Unfortunately, the CP II device is not available in Japan.
In our patient, we performed the candy-plug method and created a candy-plug from the Excluder aortic extender. Our patient’s abdominal aortic diameter was too small to achieve effective intervention. Further, as the treatment length increases, the risk of paraplegia also increases; therefore, we decided to perform the candy-plug technique. The surgery was performed according to the procedure described by Ogawa et al. 1 They used the Excluder aortic extender since it can be easily modified and delivered to the false lumen. Six months after the procedure, follow-up CT showed that the proximal false lumen was completely thrombosed, and that the morphology of the candy-plug had changed. The true lumen was remodeled and became nearly circular; thus, good aortic remodeling was observed in the patient. This is the first report of nearly circular aortic remodeling using the candy-plug technique.
The indications for this surgery are limited. First, a large entry point in the descending abdominal aorta that is more peripheral than the candy-plug position must be visible on contrast-enhanced CT. If there is no re-entry point in the descending abdominal aorta, it is impossible to position a candy-plug in the false lumen. Second, too large a false lumen size is not a indication for this operation because all Excluder Aortic Extender Prosthesis products available in Japan are smaller than 36 mm. We believe that the size of the false lumen should be approximately equal to the Aortic Extender diameter. If it is too large, there is a risk of aortic rupture, whereas if it is too small, the candy-plug will not be fixed. Size selection must be studied in more cases in the future.
We consider candy-plug placement in the true lumen central to the TEVAR to avoid occluding the AKA. We performed the operation in cases in which it was possible to place the candy-plug central to the celiac artery. We experienced no cases of thrombosis of the peripheral false lumen where a candy-plug was placed, although it is possible to place it more centrally than the celiac artery.
We performed TEVAR using the candy-plug technique in our previous six patients using the Zenith TX2® TAA Endovascular Graft and obtained complete thrombus formation in the false lumen and remodeling of the true lumen; however, the size of the false lumen was not reduced. The frame of the Zenith TX2® TAA Endovascular Graft is stainless steel, whereas that of the Excluder Aortic Extender is nitinol. Nitinol is softer than stainless steel, 7 and it is assumed that the Excluder aortic extender might be more deformable than the Zenith TX2® TAA Endovascular Graft. The Excluder aortic extender may easily deform in response to blood pressure changes associated with the progression of thrombus formation in the false lumen during the remote period, which may change the morphology of the Excluder aortic extender. With such a change in morphology, an excessive increase in the pressure of the false lumen can be prevented, and we believe that complications associated with the expansion of the false lumen in the remote period can thus be reduced. A candy-plug created from the Excluder aortic extender by a surgeon, which can change its morphology when placed in a false lumen, should lead to optimal long-term results and improved aortic remodeling. Idrees et al. reported that for 29% (6/25) of patients who underwent embolization of a false lumen by an iliac occluder of ZIP (Cook medical, Bloomington, US) or Talent™ Occluder with Occluder Delivery System (Medtronic, Santa Rosa, US), a covered stent graft was insufficient, and additional treatment had to be administered. 8 Since there have not been many reports on long-term results after the candy-plug technique or appropriate indications for performing the candy-plug technique, it is necessary to further research on performing TEVAR with the candy-plug technique.
Conclusion
We performed TEVAR using the candy-plug technique with the Excluder aortic extender and found that the morphology of the candy-plug changed within the false lumen, and the true lumen was successfully remodeled. We believe that the candy-plug technique along with the use of the Excluder aortic extender is a useful method for occluding the false lumen and improving aortic remodeling.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.