
Abstract
This manuscript describes an endovascular repair of a symptomatic, large proximal left subclavian artery aneurysm in a patient with dextrocardia and right-sided aortic arch and absent bilateral internal carotid arteries. The patient had surgical reconstruction as an infant for congenital heart disease with Ventricular Septal Defect, bifid sternum . Given her previous surgical history, we declined an open operation and performed an endovascular repair with stent grafts to successfully repair the subclavian artery aneurysm. The patient had an uneventful postoperative course and follow-up ultrasonography demonstrated successful repair with preservation of flow through the left subclavian and vertebral arteries with resolution of her symptoms.
Keywords
Introduction
Dextrocardia is a congenital anomaly occurring in .01% of live births. 1 Patients with dextrocardia also have associated congenital anomalies with situs inversus totalis, 2 in which the positions of abdominal and thoracic viscera are inverted. While most patients remain asymptomatic, they occasionally present with symptoms due to the transposition of the great arteries, where the aorta and pulmonary artery have switched. These symptoms include cyanosis, shortness of breath, lack of appetite and poor weight gain. Patients can experience complications such as hypoxia, heart failure, and damage to the lungs. Anomalies of the aortic arch are rare and are usually the result of atypical segmental regression of the paired aortic arches at approximately the seventh embryonic week.
Aneurysm formation of the subclavian artery is rare, with an incidence of approximately .13%. 3 They are usually caused by trauma, atherosclerosis, or thoracic outlet syndrome. 4 Depending on the location of the aneurysm and associated pathology, either a direct open repair, endovascular repair, or a combination of both open and endovascular techniques are used for treatment. There are limited reports regarding the occurrence of both dextrocardia and an intrathoracic subclavian artery aneurysm occurring concurrently. We report an unusual case of symptomatic, large left subclavian artery aneurysm repair in a patient with dextrocardia and absence of bilateral internal carotid arteries.
The patient provides consent for publication of this report. The patient is a 45-year-old white female with a known history of dextrocardia and associated episodes of syncope and chest pain requiring multiple emergency room visits. The patient was born with a bifid sternum, right sided aortic arch, mild infundibular pulmonary stenosis, and a large ventricular septal defect with some right ventricular muscle bundles. The sternal defect was repaired 5 days after birth. The patient underwent repair of the ventricular septal defect and excision of muscular bands in the right ventricular outflow tract at 3 years of age. In addition to her dextrocardia, her CTA (Figure 1(A)) of the chest and neck demonstrated a right-sided aortic arch (Figure 1(B) and), bilateral innominate arteries with absent internal carotid branches. Her bilateral common carotid arteries and left subclavian artery originated from the left innominate trunk. Her anterior intracranial circulation was fed by the vertebrobasilar arterial system. She additionally had 2 mm and 3 mm intracerebral aneurysms. She did not undergo any procedures involving her subclavian arteries. She presented to us with an intrathoracic 2.1 cm saccular intrathoracic subclavian artery aneurysm with a proximal segment of stenosis. Noninvasive upper extremity arterial Doppler studies indicated that she had more than 40 mmhg difference in systolic blood pressure between arms. Given the complex anatomy in association with the stenosis, it was felt her neurologic symptoms were due to global cerebral ischemia. The origin of her aneurysm was just proximal to the origin of the left vertebral artery. The left subclavian artery originated from a left brachiocephalic trunk. She was offered an endovascular repair given her complex surgical history. With her cerebral blood flow provided by the vertebrobasilar system, it was crucial to try to maintain antegrade flow into her left vertebral artery. The left subclavian artery distal to the aneurysm appeared normal with a landing zone to preserve flow into the vertebral artery. A brachial artery cutdown was performed to obtain access for the procedure via a 7Fr sheath placed in a retrograde fashion. The subclavian artery was extremely tortuous (Figure 2), and it was challenging to track a wire to the distal aorta. Ultimately, we were able to track a floppy .035” hydrophilic wire, which was then exchanged for a Quick Cross catheter (Koninklijke Philips N.V.), using it to place a .035" Glide Advantage wire (Terumo, Japan) into the distal aorta. For precise placement, the saccular subclavian artery aneurysm was repaired using 8 mm × 39 mm telescoping into a 7 mm × 29 mm VBX balloon-expandable covered stents (W.L. Gore and Associates, Flagstaff, AZ). Completion arteriogram is shown in Figure 3 demonstrates resolution of the stenosis with exclusion of the aneurysm and preservation of flow into the left vertebral artery. The patient tolerated the procedure well and was discharged home on postoperative day #1 on dual antiplatelet therapy. She recovered well and presented for follow-up at 1, 3and 12 months post-procedure without complaints. Follow up -Ultrasonography demonstrated good flow through the left subclavian and vertebral arteries with no flow into the occluded saccular subclavian artery aneurysm (Figure 4).
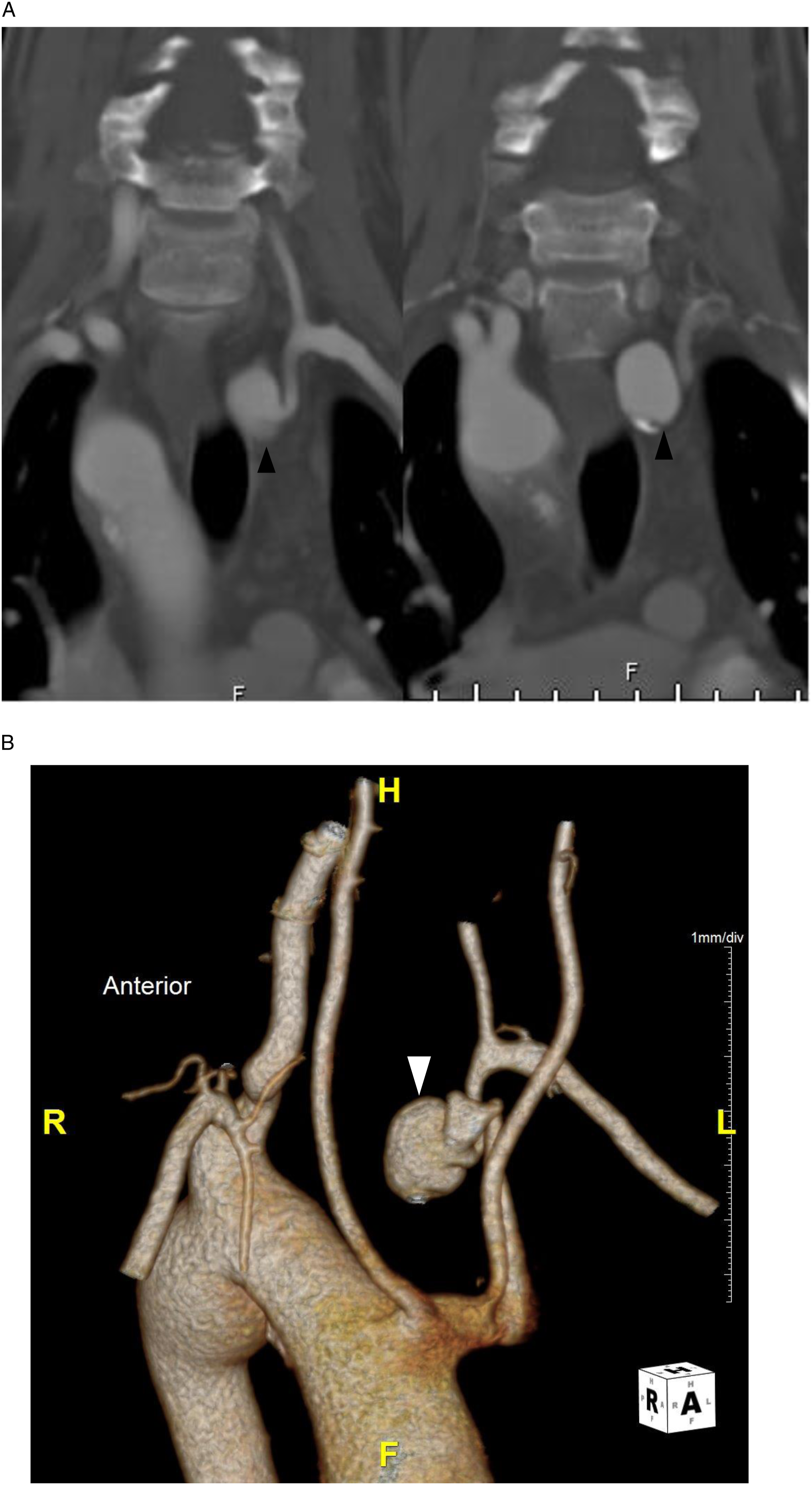
Pre Procedure CT Angiography (A) with a 3-D reconstruction (B) showing subclavian artery aneurysm (arrow heads), right-sided aortic arch prior to repair.

Subclavian artery arteriogram showing aneurysm prior to repair with left common carotid artery (arrow head).

Post repair angiography showing excluded subclavian artery aneurysm with preserved flow in left vertebral artery (arrow head) following repair with stent grafts.
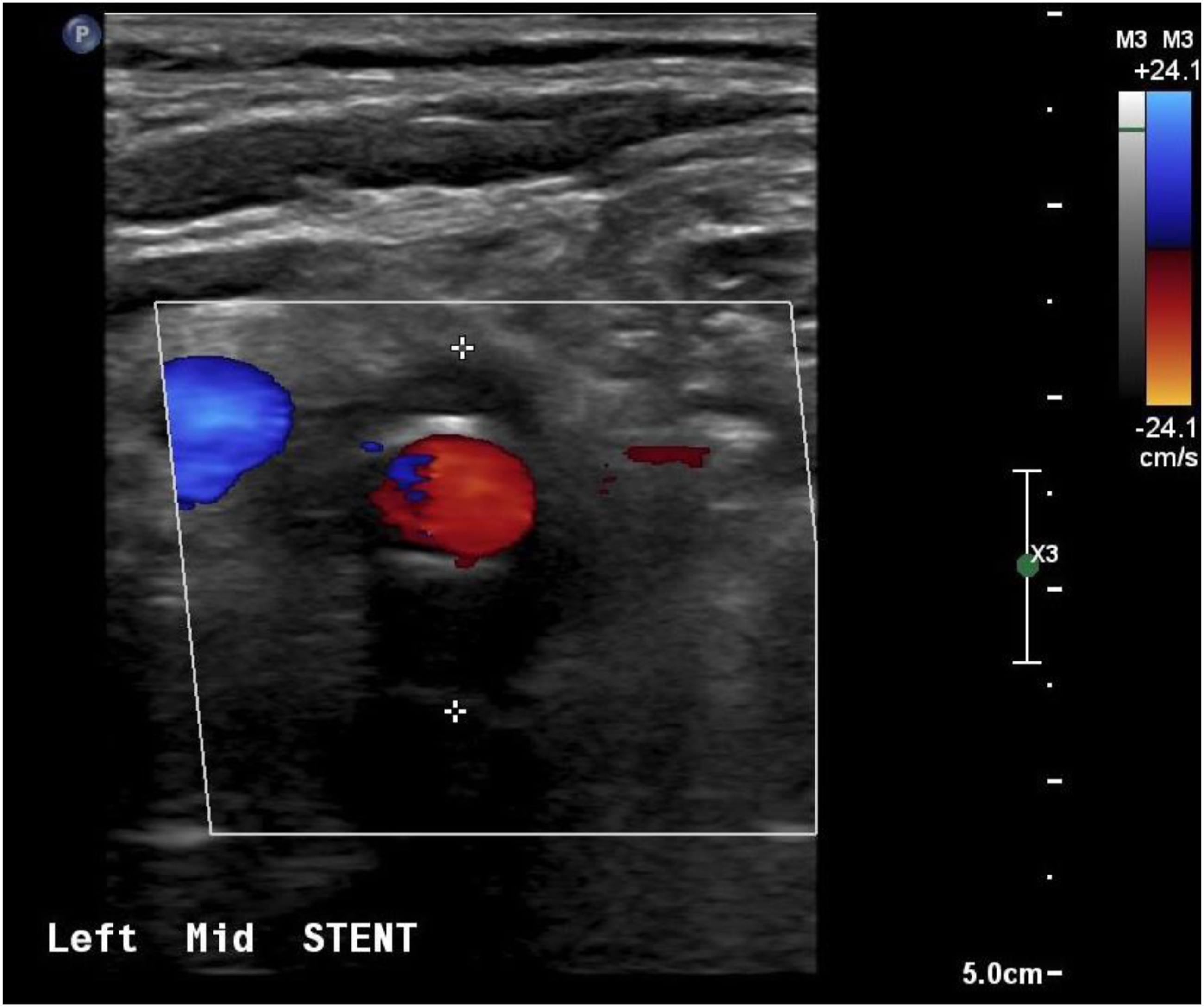
Follow up ultrasonography of the subclavian stents with patency with absence of flow in aneurysm (between * markers).
Discussion
Dextrocardia and subclavian artery aneurysms are both rare conditions. A review of the literature does not indicate that these conditions have been reported concurrently. Dextrocardia occurs in approximately .01% of live births. 1 Even among a large series of 3698 adults followed with a history of congenital heart disease, only 19 (.5%) had dextrocardia. 5 A few large artery anomalies have been reported with dextrocardia including an aberrant origin of the right subclavian artery from the pulmonary artery, 6 nonconfluent pulmonary arteries,2,7 aortic stenosis 8 and coronary artery anomalies.9,10 A review of the literature did not disclose any reports of concurrent dextrocardia and a subclavian artery aneurysm. There have been reports of a congenital atrial appendage aneurysm 11 and a ventricular aneurysm, 12 and cerebral artery aneurysm. 13
Subclavian artery aneurysms are also extremely rare. 14 1 series of 1488 cases of atherosclerotic aneurysms reported an incidence of .13%. 3 Reports indicate that the most frequent location of subclavian artery aneurysm is at the thoracic outlet.15,16 Another type of aneurysm involving the subclavian artery is Kommerell’s diverticulum, which is a developmental error with a remnant of the fourth dorsal aortic arch. 17 There may be cystic medial necrosis of the adjacent aortic wall and an aberrant subclavian artery may arise from the contralateral side. 17 This has been reported with a right-sided aortic arch with an aberrant left subclavian artery without dextrocardia.18,19 Kommerell’s diverticulum can be repaired with both open and endovascular approaches. 16 In this case, the left subclavian artery and left common carotid artery originated from a common left innominate trunk
There have been a few reports of repair of intrathoracic subclavian artery aneurysms in patients without dextrocardia reported in the literature. In 1 of the largest series of 19 patients with at least an intrathoracic portion of the subclavian artery aneurysm, Thoracic Endovascular Aneurysm repair (TEVAR) was used in sixty four percent of the patients in their cohort . The remainder of the 36% of patients underwent an open repair. 20 Twenty one percent of these patients had a connective tissue disorder. One case report related a hybrid repair with a polytetrafluoroethylene conduit and coil embolization. 21 Another author reported doing a transposition of the vertebral artery to the common carotid artery followed by placement of a covered stent across the subclavian artery aneurysm. 22 Stent grafts alone have also been used alone to repair this type of aneurysm with 6 of these reported in a single center study.21-23
In this patient, bilateral absence of the internal carotid arteries mandated the preservation of the vertebral arteries. The patient also had the complexity of dextrocardia and right sided aortic arch. We used an endovascular approach for repair using a balloon-mounted covered stent in the setting of previous congenital heart surgery. Alternatives like coil embolization and bare metal stent supported coil embolization are additional treatment options. In addition, our patient also had a combination of proximal stenosis with aneurysmal degeneration and hence coiling alone would not have been an ideal treatment option. Even though one one can consider left carotid to left subclavian bypass with ligation of the subclavian artery proximal to the vertebral artery as a treatment option, given the unusual anatomy with complex history of this patient we used an endovascular approach. Further we felt it is important to establish inline flow that allowed us to address both stenosis as well as aneurysmal degeneration simultaneously. At 12 months postoperatively, the patient reported resolution of symptoms and flow preservation through her subclavian and vertebral artery. The saccular subclavian artery aneurysm was thrombosed with no evidence of an endoleak. Besides the rarity of the case, pre operative imaging, understanding variations in anatomy, and treatment planning are critical to the success of these complex endovascular repairs.
Conclusion
Intrathoracic subclavian artery aneurysms are a rare occurrence and even more so with an associated dextrocardia and congenital heart anomaly. This case documents the only reported case of an intrathoracic subclavian artery aneurysm repair in a patient with dextrocardia utilizing covered stents, with preservation of flow through subclavian and vertebral arteries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent Statement
Written informed consent was obtained prior to the preparation and submission of this manuscript and is available upon request.