
Abstract
Objectives
Endovenous Radio-frequency Ablation (RFA) has become a common treatment for chronic venous insufficiency. The Medtronic® Closurefast catheter was previously the only RFA catheter approved for use in this procedure. In 2018 VenClose® Company’s new device was approved. As there has been little literature on this new device, we examined our results with this new alternative.
Methods
Patients with symptomatic venous insufficiency had their lower extremities mapped via ultrasound. If superficial reflux (>.5 s) was found the patients were recommended a 6-week conservative course of compression stockings, elevation, and NSAIDs. If conservative treatment failed, the patient was scheduled for an RFA. The procedure was done at the outpatient clinic, instructions were given to return for follow-up in 3-5 days, and every 3 months thereafter for the first year. 1032 procedures were performed over 14 months.
Results
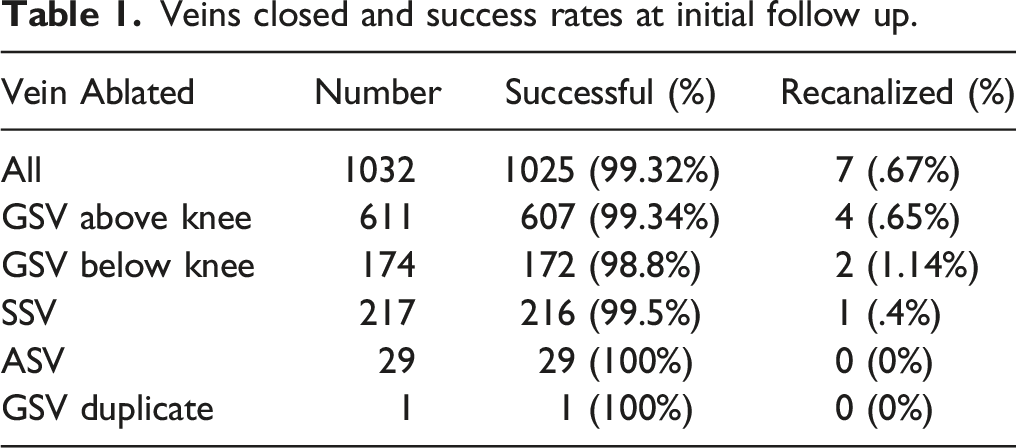
We had 503 patients, 69% female, mean age 54 ± 12. Under the CEAP system, clinical manifestation portion, the majority of our limbs were class C3 and class C4. The majority of veins closed were GSV above knee and SSV. Follow-up duration ranged from 1 to 276 days (Mean (M) = 10 SD: 20 days). Our success rate was 99.32% at initial follow-up. We observed EHITs in 12 cases (1.16%), 8 of which were class I, 2 of which were class II, and 2 of which were class III. We noted SVTs of proximal varicose veins in 40 cases (3.88%) and SVT of distal GSV in 4 cases (.38%). There were 4 (.38%) cases of DVT, 3 in calf muscular veins (.29%), and one in a perforator vein (.09%). We observed two cases of puncture abscess (.193%), 8 cases of infection at the puncture site (.77%), with 8 infections occurring at locations other than the puncture site and not as a result of the procedure.
Conclusion
These preliminary results indicate that this new machine and catheter are promising with low rates of EHIT, recanalizations, and other complications. It is important to research this catheter and further studies should continue to follow up to examine recanalization rates over a more long-term follow-up.
Introduction
Chronic Venous Insufficiency (CVI) affects up to 25% of women and 15% of men in Western countries. 1 In the last 20+ years, endovenous ablation of the superficial veins has become a standard treatment for CVI, especially after it was demonstrated to be comparable with stripping and ligation of incompetent veins. 2 The two main varieties of ablation being either Endovenous Laser Ablation (EVLA) or Radio-Frequency ablation (RFA).
In the United States, the only RFA catheter approved for use was the Medtronics ClosureFast system, up until 2018. At that time, the Venclose RFA catheter was approved for use. The Venclose catheter delivers thermal energy, and a single catheter has both a 10 cm and a 2.5 cm treatment option. In our experience, this catheter is notably cheaper than the ClosureFast system.
As there has been little literature on the Venclose catheter, we decided to examine our results with this new system. Our study reviewed the charts of patients who had a RFA procedure and evaluated for the success rate of the procedure (whether the vein was obliterated), and adverse outcomes such as deep and superficial venous thrombosis (DVT & SVT), endovenous heat-induced thrombosis (EHIT), and infection.
Methods
Upon presentation to the outpatient clinic, symptomatic patients had their lower extremity veins mapped via ultrasound, assessing for DVT, SVT, and superficial venous insufficiency (defined as reflux >.5 s). If patients were found to have reflux, they were recommended conservative therapy for 6 weeks, consisting of graded compression stockings to be worn daily, elevation of the affected limb above the level of the heart, and non-steroidal anti-inflammatory drugs used to manage pain. After 6 weeks of conservative therapy, patients were reevaluated at the clinic, and if symptoms persisted, and the superficial vein was larger than 4 mm, they were scheduled for an endovenous ablation. Patients who presented with venous stasis ulcers were scheduled for endovenous ablation at their initial visit.
Our center performs both RFA and EVLA. Based on our observations, we preferentially perform RFA on patients younger than 65 due to lower pain scores for that population, however, factors such as insurance approval or denial could affect which variety of ablation the patient received. We perform ablations of the great saphenous vein (GSV), separately for the above and below knee segments, small saphenous vein, accessory saphenous vein, and duplicate great saphenous vein. We treat the above knee segment of the GSV first preferentially, as in our experience this had led to lower rates of nerve injury, and if the patient continues to have reflux and symptoms, we then treat the below knee segment of the GSV. We treat each segment and the left and right side in separate, staged, procedures.
During the radiofrequency ablation procedure, the catheter is heated to 120°C for a treatment cycle of 20 s. After positioning the catheter 2-3 cm away from the junction with the deep vein, our patients had the cephalad portion of their superficial veins treated twice with the RFA energy, with the remaining portions treated once. The 10 cm treatment length was used for the majority of the vein, with the 2.5 cm treatment length being used to treat the terminal portion. After the procedure, an ace wrap was applied to the limb for 2 days, and instructions were given to follow up in 3-5 days for duplex, and every 3 months thereafter for one year. Data were collected by reviewing the charts and duplexes of patients who received an RFA procedure. We performed 1032 procedures on 503 patients from March 2020 to May 2021.
Data collection included age, gender, vein ablated, duplex date & results, adverse outcomes, and presenting symptoms based on CEAP score. The collection and interpretation of data conformed to the principles set by the Declaration of Helsinki and HIPAA. Institutional Review Board approval was obtained 4/1/2020, and consent by each patient was waived by Total Vascular Care IRB as the data are blinded, retrospective, and of minimal risk.
Results
Veins closed and success rates at initial follow up.
We noted adverse outcomes of Endovenous Heat-Induced Thrombosis in 12 (1.16%) cases. Using the American Venous Forum EHIT classification system, 4 we had eight cases (.78%) of class I, two cases (.19%) of class II, two cases (.19%) of class III, and no cases of class IV EHIT.
Other negative outcomes of the procedure included Superficial Venous Thrombosis, which occurred in varicose veins in 40 instances (3.88% of all cases), and in distal segments of the GSV in 4 (.38% of all cases). We observed 4 (.38%) cases of DVT, 3 in calf muscular veins and one in a perforator vein. Combining EHIT, SVT, and DVT results in an overall thrombotic complication rate of 5.62% (58 cases). There were 2 cases of puncture abscess (.19%). There were 16 cases of infection/cellulitis following the procedure, however, only 8 of these instances were located at or near the puncture site. The remaining eight were ulcer infections or at other locations on the limb, which we determined to be cellulitis due to venous stasis. This results in an infection rate of .77% when excluding cellulitis not at the puncture site, and 1.54% when including those found outside the puncture area. We did not track incidences of paresthesia, nerve damage, or sensory changes.
Discussion
This is among the first and largest datasets on Venclose, and these preliminary results indicate that the system is safe and effective, with low rates of EHIT and recanalization at initial follow-up. Our percentage of EHIT (1.16%) is below the 5.9% overall EHIT rate found by Aurshina A, Ascher E, Victory et al 5 , and is about the same as the 1.78% rate of EHIT due to RFA in Chait, Kirbrik, Alsheekh et al.‘s 2020 study. 6 Our overall thrombotic complication rates are similar to past studies exploring complications of the Closurefast system.5,7,8 Our puncture site infection rate of .77% was found to be lower than the Closurefast system, with previous studies finding 1.5%.6,7
These are early results, and our study was a single-center retrospective chart review with no control arm. Our follow-up was only for an initial duplex, intended 3-5 days post-procedure, some patients did not return to follow up for an extensive period of time (hence our wide range), however the majority did return within the average of 10 days. Our population was somewhat older, and our results may not apply to younger demographics. Another weakness of our dataset is that we did not collect quality of life data.
Further studies should examine different variations of the procedure. For example, observing if complication rates change when performing ablations in staged vs simultaneous procedures, and in simultaneous procedures if different combinations of veins treated (ie, GSV and SSV or SSV and ASV) result in higher EHIT rates. Another possible direction for future study can examine whether certain factors can help reduce EHIT/DVT rates, such as different post-operative management strategies, surgeon and technician experience, length of procedure, etc.
The Venclose™ catheter can be used to treat both a 10 cm segment and a 2.5 cm segment in one catheter, this 2-in-1 functionality is not only versatile but can help save cost as the Medtronics™ system only offers 7 cm and 3 cm options in individual catheters. The longer Venclose catheter can also lead to a shorter procedure. The 2.5 cm treatment length was used in our clinic to treat the terminal portion of the vein, as this reduced the need to overlap treated areas. As this new catheter and machine become widely used, this can change the face of the RFA market, as there is now an alternative to the Medtronics ClosureFast® system, which is cheaper and has comparable early results. In our experience Venclose was approximately 25% cheaper, although prices can vary with use and quantity purchased.
This can have important implications, especially on a worldwide stage, as many countries that do not have private or public health insurance rely on individuals to pay for their healthcare. A cheaper alternative to ClosureFast® may make the RFA procedure more accessible worldwide. It is critical to continue to examine this new alternative for success rates, adverse outcomes, and long-term recanalization, as our ability to provide options and accessible treatment for superficial venous insufficiency evolves further.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.