
Abstract
Pilon fractures of the distal tibia are usually the result of a high-energy trauma and can affect seriously the arterial vasculature carrying an increased risk of amputation at the malleolar level or higher. Such cases represent a challenge for the orthopedic surgeons and a multidisciplinary approach is mandatory in order to salvage the threatened limb. We present an unusual case of a closed pilon fracture with injury of all tibial vessels leading to acute limb threatening ischemia. The patient was treated successfully with external fixation and a short tibial-pedal bypass with use of an autologous reversed saphenous vein graft. This example dictates how a distal leg fracture can be dramatic and that awareness of vascular examination coupled with high suspicion of vascular damage can be limb-saving. Multidisciplinary approach is warranted since the topology and complexity of the ankle lesions necessitate staged orthopedic reconstructions with tibio-distal bypass and appropriate skin coverage of the distal anastomosis.
Introduction
Pilon fractures represent 1%-10% of all tibial fractures and <1% of all fractures to the lower extremity. 1 They are considered high-energy traumas caused by axial compression trauma where the talus collides with the distal surface of the tibial joint. 2 There are only scarce data regarding acute limb-threatening ischemia associated with ankle fractures, underscoring a delay in early diagnosis rather than a rare incidence. 3 Therefore, complicated pilon fractures comprise a surgical challenge necessitating immediate and well-conducted collaboration by orthopedics and vascular surgeons as well as prompt diagnosis of ischemia by the treating physicians on site. 4 Moreover, this type of distal arterial reconstruction is technically demanding since it comprises distal low-caliber vessels (ie, mid anterior tibial to dorsalis pedis artery) and a vein graft crossing a swollen area of damaged tissues.
We present a case of successful revascularization of acute limb ischemia due to arterial damage of all tibial vessels associated with a severe pilon fracture and we discuss the pitfalls and challenges of the management. Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Case Presentation
A 57-year-old male suffered a right femur fracture and bilateral pilon-type ankle fractures (Figure 1A) due to fall from height (third floor) and was admitted to our Hospital with accompanying acute limb ischemia (pain, pallor, numbness and impaired mobility of the toes, complete absence of arterial Doppler signal) of the left foot. Both the preoperative computed tomography angiography (Figure 1B) and the intraoperative on-table angiography confirmed complete cut-off of all tibial vessels at the malleolar level. The reduction with external fixation medially did not restore audible Doppler sign. A. Bilateral pilon fractures of the tibiae. Note the severe damage of the left ankle. B. The preoperative computed tomography angiography (posterior view). The abrupt transection of the tibial vessels at the level of the left maleolar injury is depicted. The distal run-off of the tibial vessels on the right is also visualized. Note the right distal femoral fracture along with the pilon fractures.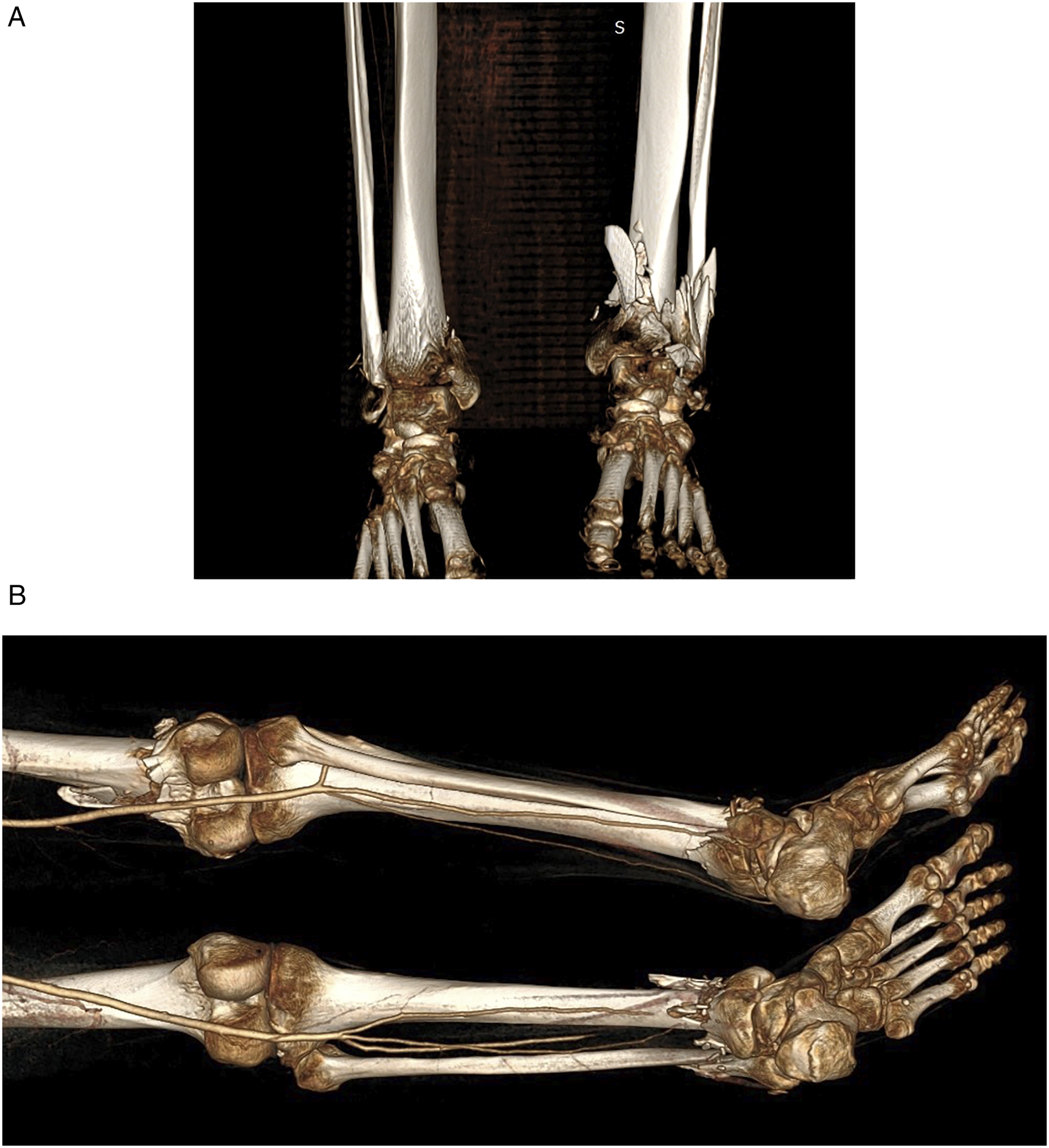
Since the placement of external fixation precluded any manipulations, surgical exploration and intervention on the posterior tibial artery (ie, exposure of the artery, placement of the vein graft and construction of the anastomosis), we chose to perform a bypass from the anterior tibial to the dorsalis pedis artery which was much easier to explore, manipulate and anastomose, using a short reversed segment of the ipsilateral greater saphenous vein placed subcutaneously (Figure 2A). The proximal and distal anastomoses were performed in a end-to-side manner, using continuous suture technique with 6-0 and 7-0 monofilament suture, respectively. The anterior tibial artery was occluded with soft bulldog clamps while the dorsalis pedis artery was secured with a double encircled vessel loop. The bypass led to successful reperfusion with immediate hemodynamic and clinical improvement. A. The short vein bypass from the middle segment of the anterior tibial artery (arrowhead) to the dorsalis pedis artery (arrow), following the external fixation medially. B. The distal anastomotic exposure has been covered with skin graft (arrow).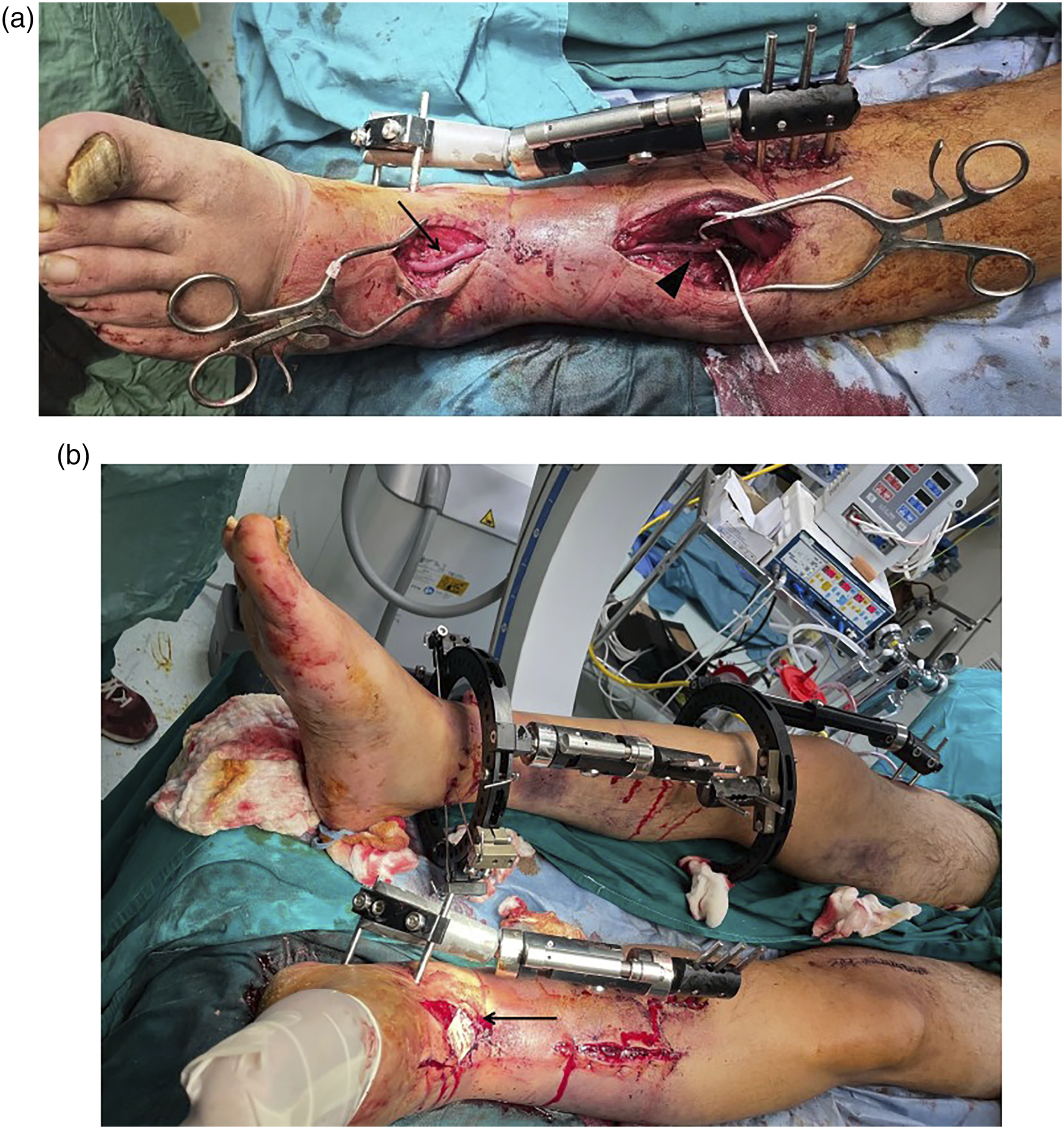
Attention should be paid to avoid tension over the venous conduit especially upon wound closure in the swollen foot. Therefore, the skin defect was managed with release skin incision and coverage with a full thickness skin graft (Figure 2B). Accordingly, external fixations were also accomplished with respect to the ankle and femur fractures of the right lower limb. The patient recovered well and was subjected to other orthopedic surgeries during the following period. At 6 months follow-up the wounds have been healed, the graft is patent with peripheral palpable pulses and the patient is mobilized, yet still with support under physiotherapy supervision due to orthopedic-related difficulties.
Discussion
The present case represents an immense surgical challenge as it combines two rare cases; a pilon fracture with complete traumatic transection of all tibial vessels leading to acute limb-threatening ischemia. In order to perform the bypass procedure, the unstable pilon fracture has to be stabilized firstly, yet limiting the operational field from the medial side and, consequently, the facility to harvest as bypass conduit the tibial segment of the great saphenous vein.
Short tibio-tibial bypasses represent only a minor percentage (1.7%) of all extremity bypass procedures.5-7 Davidson and Callis reviewed retrospectively their experience with arterial reconstruction in the foot and ankle, confirming that the anterior tibial artery was the inflow vessel in only 1% of cases. 6 Lyon et al 7 have reported their 11-year experience with tibio-tibial bypasses in patients with limb-threatening ischemia and occlusive lesions limited to the distal tibial and peroneal arteries. They documented a primary patency rate of 77% and 62% at 1 and 5 years year for these interventions. Moreover, the limb salvage rate after 5 years was 74%. Furthermore, the authors reported a comparable primary graft patency at 4 years between these short bypasses and those originating from the popliteal artery.
In our case the external fixation preceded the vascular reconstruction. In a recent study by Shahien et al 8 in 199 patients with combined orthopedic and vascular injuries 62% of these patients had their definitive vascular repair before the bony reconstruction. Interestingly, 13 of the 15 documented vascular complications, had the definitive vascular repair performed before the definitive osseous repair. This series documented a high percentage of acute and late amputations, with the highest rate (62%) associated with tibial fractures. Even if revascularization is restored, bone infections and nerve lesions can be dramatic leading to late amputation. These confirm the surgical challenge and complexity of the tibial/pilon fractures and underscore the high suspicion of vascular injury that the physician should have, since the ischemia time affects significantly the successful salvage while some vascular injuries can go undetected in closed pilon fractures leading to irreversible damage.8,9
Autogenous greater saphenous vein is the graft material of choice for bypass operations, especially when it comes to vessels below the knee as inflow or outflow vessels. Ideally, the diameter mismatch between the reversed vein and the target artery should be minimal to avoid flow disturbances and facilitate long-term patency. Although an anticipated mismatch is usually evident between the upper end of a reversed venous segment and the target vessels below the knee, we chose the most distal part of the harvested greater saphenous vein to accommodate better to the anterior tibial artery (Figure 3), which was documented patent, non-atherosclerotic with pulpable pulse immediately above the site of the proximal anastomosis and a proximal stenotic disease was excluded with the pre- and intraoperative angiographies. Generally, harvesting the contralateral vein as a bypass conduit is preferred in trauma cases, in order to preserve venous outflow tracks when deep venous injury is anticipated in the ipsilateral injured limb. Yet, the very distal site of the injury in our case as well as the distal femoral fracture on the right, led us harvest the ipsilateral saphenous vein with no consequences. A matter of concern in distal traumas is the skin cover of the distal part of this bypass, since most of the time the need for debridement of the infected tissue, skin defects and the swollen ankle and forefoot near the fracture preclude a tension-free closure of the skin over the distal anastomosis. In our case, a release incision along with skin graft coverage was performed to cover the anastomosis. A 4 × 4 cm skin segment was harvested along the anterolateral surface of the left thigh by the orthopedic surgeon and placed as a full-thickness skin graft. While, in general, various modalities and techniques have been suggested to manage post-fasciotomy wounds and skin defects, the presence of vascular grafts and anastomoses on site poses an additional challenge, reflecting not only the advanced surgical skills that should be recruited in such complex traumas but also the vascular awareness of the physicians when confronting orthopedic traumas.10-12 Completion angiography documenting patency of the vein graft and the proximal anastomosis to the anterior tibial artery.
The issue of primary intravascular shunting in combined orthopedic and vascular extremity trauma is a matter of debate.13,14 Admittedly, there is a lack of comparative data in the literature regaring the use of temporal intravascular shunt and no consistency in applied reporting standards, retaining controversies regarding the efficacy of these shunts.
15
Polcz et al
16
conducted recently the first multicenter, matched-cohort study to characterize early limb salvage as a function of temporal intravascular shunt in the setting of extremity vascular injury and documented lower rates of amputation during the early phase of care. Generally, it is our practice to use a Pruitt-Inahara shunt (LeMaitre Vascular Inc, Burlington, MA, USA) to bridge the popliteal artery above and below the knee in combined orthopedic and vascular lesions to restore perfusion temporarily prior to orthopedic interventions (Figure 4). Yet, in the particular case described here we did not use it, as the external fixation was conducted in 30′ and the dorsalis pedis artery was small enough; rather, we inserted the18G vein cannula in the latter to facilitate the distal anastomosis, facilitating visualization and widening of the anastomotic line and enabling simultaneous infusion of heparinized saline or vasodilating agents.17,18 Use a Pruitt-Inahara shunt (LeMaitre Vascular Inc, Burlington, MA, USA) to bridge the popliteal artery above and below the knee (arrows) preceding essential orthopedic interventions in combined musculoskeletal and vascular lesions (archive of Dr. Georgakarakos).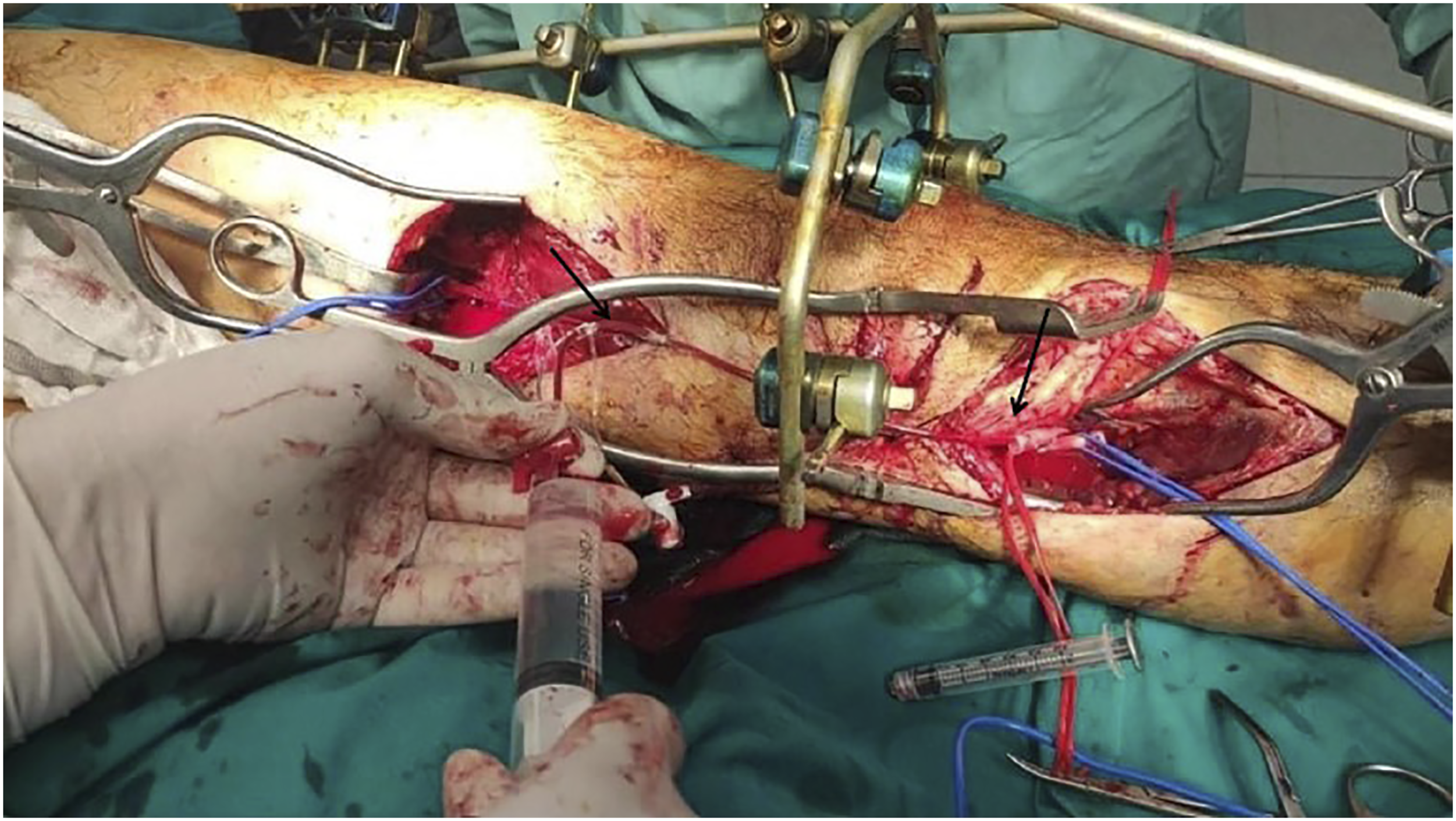
Conclusion
The prompt recognition and immediate treatment in this complicated Pilon fracture are the key elements to successful limb salvage. Multidisciplinary approach was warranted in the presented case since the topology and complexity of the ankle lesion necessitated staged orthopedic reconstructions with tibio-distal bypass and appropriate skin coverage of the distal anastomosis.
Footnotes
Author’s Note
Informed consent has been obtained from the patient and patient’s family for publication of the case report and accompanying images.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.