
Abstract
Objective
We retrospectively investigated the association between the imaging features of spontaneous isolated superior mesenteric artery dissection (SISMAD) accompanied by total true lumen occlusion and the clinical symptoms to identify the patients at high risk and establish personalized therapeutic options.
Methods
Among 261 patients with SISMAD, we selected 37 with Yun’s type III dissection; 35 patients underwent successful conservative management and 2 patients underwent exploratory laparotomy. After discharge, all patients were periodically followed up on an outpatient basis. We recorded patients’ general condition, symptoms, time until symptom relief, imaging findings and follow-up results.
Results
All patients experienced acute abdominal pain prior to admission, with an onset time of 29.95 ± 24.66 hours. The mean time until relief of abdominal pain in patients who received conservative treatment was 42.17 ± 38.09 hours. Correlation analysis revealed no correlation between the length of dissection or of the occluded segment and abdominal pain intensity. Pain scores were lower and time until pain relief was shorter in patients with a definite arc of Riolan (AOR) on admission than in those without an AOR. No collateral circulation was observed in the two patients who underwent exploratory laparotomy, and distal intestinal perfusion was poor in these cases. Complete and partial remodeling of the superior mesenteric artery (SMA) was observed in 6 and 16 patients, respectively at the 12-month follow-up. Although the SMA remained occluded in 12 patients, abundant collateral circulation was detected. Three patients were lost to follow-up.
Conclusion
This study highlights that conservative treatment should be attempted as first-line therapy in most patients with Yun’s type III SISMAD. Complete AOR can contribute to remission of clinical symptoms during the acute stage. Poor distal blood flow of occluded vessels may serve as an important indicator for identification of patients at high risk of ischemic intestinal necrosis.
Keywords
Introduction
Spontaneous isolated superior mesenteric artery dissection (SISMAD), first reported by Bauersfeld in 1947, is a rare but potentially fatal condition.1,2 Following technological advances in imaging that have facilitated accurate detection, SISMAD represents the most common isolated visceral artery dissection. 3 SISMAD usually occurs in men in their fifties. 4 Long-term observation of patients with SISMAD has shown that most patients have a benign natural clinical course; therefore, conservative management is recommended as first-line treatment, regardless of imaging features. 5 However, clinicians should be mindful of the fact that SISMAD may be an important contributor to severe true lumen stenosis and even total occlusion of the superior mesenteric artery (SMA), which may precipitate severe intestinal ischemia. 6
SISMAD is categorized into various types based on imaging findings.4,7 Currently, convincing data or consistent conclusions regarding the association between clinical symptoms, radiographic findings, and prognosis of SISMAD are unavaliable. 8 It is commonly accepted that symptoms in patients with SISMAD are associated with the length of dissection and the degree of true lumen stenosis. 9 The aseptic inflammatory response in the area of the arterial dissection stimulates the visceral nerve plexus and is implicated as a contributor to abdominal pain. 10 This theory may explain the association between abdominal pain and the length of SMA dissection; dissections that are greater in length are shown to cause more significant inflammation. According to Poiseuille’s law of fluid dynamics, flow resistance is inversely proportional to the fourth power of the radius of a tube. Intestinal blood flow through the SMA is significantly reduced in patients with a stenotic or occluded true lumen. 11 Severe true lumen stenosis was previously considered as an important indication for endovascular intervention or open surgery.12-15 However, many authors have reported that conservative treatment alone led to successful recovery in patients accompanied by true lumen occlusion.4,16
Studies have reported conflicting follow-up results; therefore, the association between the imaging features and prognosis of SISMAD remains unclear, particularly in patients with Yun’s type III SISMAD (SISMAD accompanied by true lumen occlusion).5,8 In this study, we summarize our findings and results of long-term follow-up of patients admitted to our hospital for management of Yun’s type III SISMAD. We investigated the association between imaging findings and symptoms to identify high-risk patients, and to establish personalized therapeutic options in this patients population.
Methods
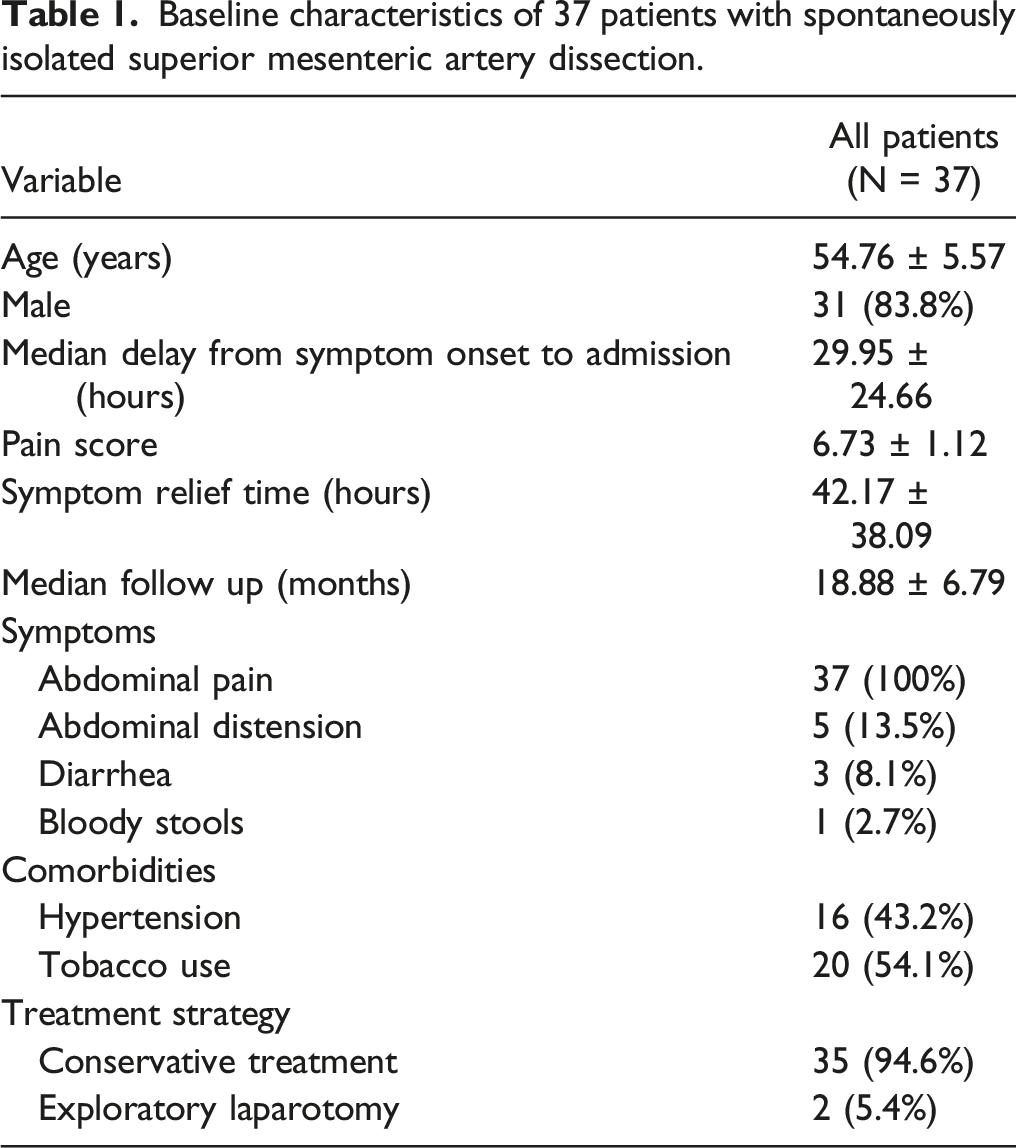
Baseline characteristics of 37 patients with spontaneously isolated superior mesenteric artery dissection.
After admission, patients without acute peritonitis or hematochezia received conservative treatment, which included close observation for development of bowel ischemia, a fasting status, intravenous fluid therapy, or total parenteral nutrition therapy until resumption of oral intake. Following resolution of abdominal pain, patients were gradually transitioned from sips of water to regular food. Low-molecular-weight heparin was routinely administered twice daily as anticoagulation therapy. Additionally, alprostadil (10 μg) was administered intravenously daily to dilate compensatory collateral vessels and inhibit platelet aggregation. Repeat CTA was performed a week later to evaluate intestinal blood flow in patients with persistent symptoms or in those with symptom aggravation during conservative treatment. Conservative management was continued in patients in whom distal blood flow into the SMA was clearly visualized on imaging studies and in those who showed no evidence of acute peritonitis.
We performed exploratory laparotomy in patients with acute peritonitis or hematochezia to evaluate the extent of bowel viability and perform bowel resection, if deemed necessary. These patients alone were administered perioperative antibiotics (prophylactic antibiotics were not administered to other patients). After discharge, the patient who underwent stent implantation was recommended antiplatelet therapy for one year, and the other patients did not receive anticoagulant or antiplatelet therapy. All of the patients underwent periodic follow-up at 6-12 month intervals on an outpatient basis to monitor the recurrent of abdominal symptoms and morphological changes in the SMA lesion. Patients who presented with abdominal distention or pain after eating during follow-up were recommended to undergo CTA examination to evaluate the intestinal blood supply.
Follow-up CTA findings were categorized into the following types: complete remodeling of the SMA (Figure 1A, B), partial remodeling of the true lumen (Figure 1C, D), and occluded SMA with compensatory collateral circulation (Figure 1E, F). Aneurysmal dilatation of the false lumen, defined as diameter of the false lumen measuring >50% of the SMA, was documented in patients with partial remodeling of the true lumen. A, B: Image showing complete recanalization of the true lumen of the SMA without residual arterial dissection. C, D: Image showing partial recanalization of the true lumen of the SMA accompanied by luminal narrowing or residual dissection. E, F: True lumen of the SMA showing no obvious change compared with the former, but collateral circulation had developed. G: SMA occlusion is observed; however, CTA showing definite compensatory collateral pathway development ( white arrows indicate the arch of Riolan). H: Image showing SMA was occlusion without distinct collateral circulation and poor distal perfusion of the intestine.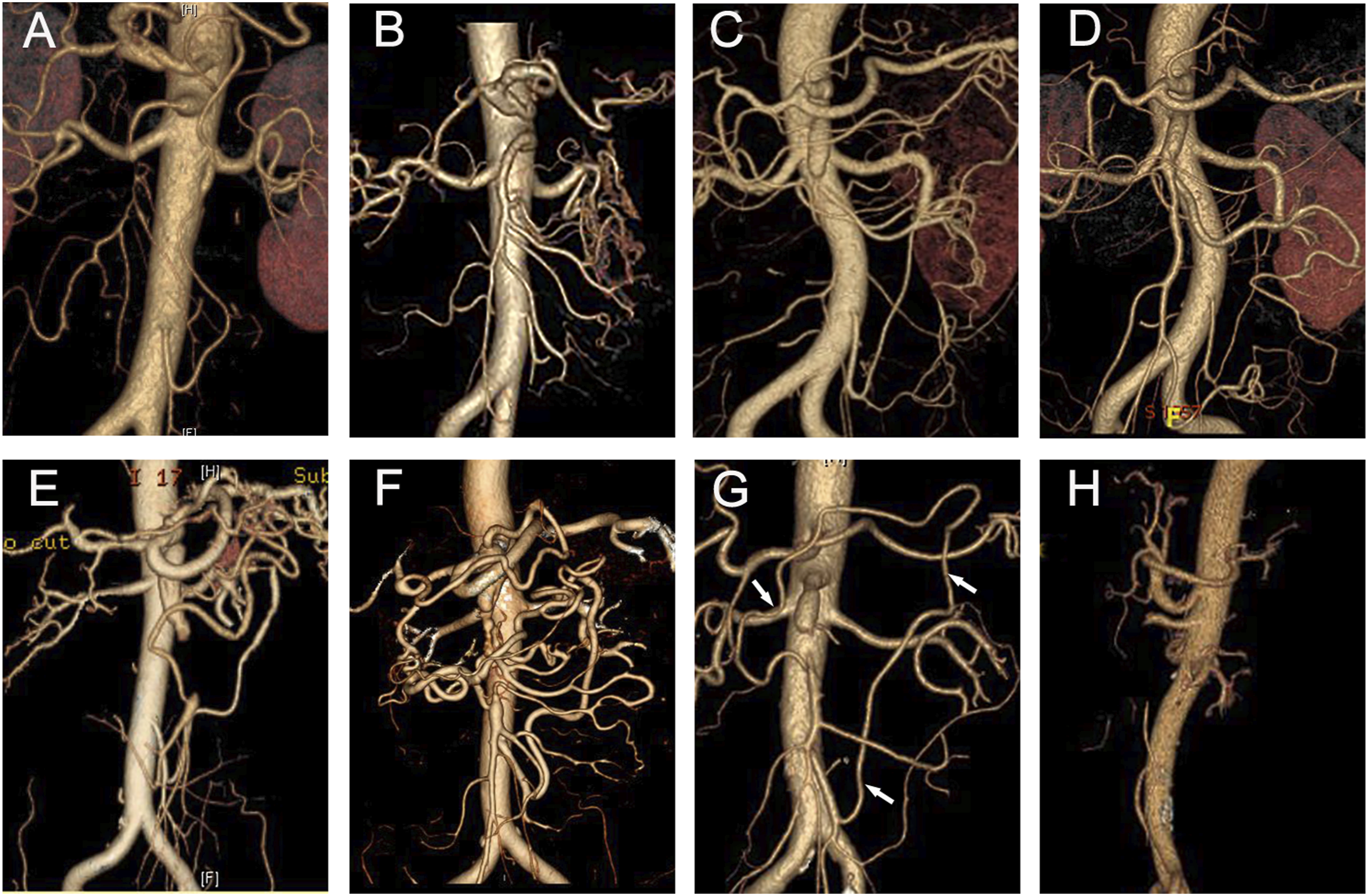
All procedures performed in this study were in accordance with the principles of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Ethic Committee of Yangzhou University Affiliated Northern Jiangsu People’s Hospital. Informed consent was obtained from all patients included in the study.
Statistical Analysis
All statistical analyses were performed using the SPSS software Windows version 25.0 (SPSS Inc., Chicago, IL, USA). Values are expressed as mean ± standard deviation. Spearman correlation coefficient was used for correlation analysis. The Mann-Whitney U test was used for comparison of intergroup differences in ordinal variables. Continuous variables are expressed as means and standard deviations for parametric distributions and were compared using the independent t-test. P-value < 0.05 was considered statistically significant.
Results
Clinical Outcomes
In this study, of the 261 patients with SISMAD, we selected 37 patients (34 men and 3 women, mean age 54.76 ± 5.57 years) with Yun’s type III dissection. No concomitant mesenteric vein disease was detected. All patients experienced acute abdominal pain prior to admission, with an symptom onset time of 29.95 ± 24.66 hours. The mean abdominal pain score was 6.73 ± 1.12. Accompanying symptoms included abdominal distention, nausea, diarrhea, and bloody mucopurulent stools. Two patients underwent emergency exploratory laparotomy and the others were successfully treated using conservative management. The mean time until abdominal pain relief among the patients who received conservative treatment was 42.17 ± 38.09 hours. Symptoms were alleviated within 2-3 days in most patients, except in one patient in whom symptoms resolved only after 9 days.
Both patients who underwent surgery presented with severe abdominal pain upon admission; one patient showed typical signs of peritonitis and the other had clear evidence of abdominal distention and hematochezia. Intraoperatively, the intestines appeared pale and paralytic, and the true lumen of the SMA was completely occluded by the thrombotic false lumen in both patients. The small intestine showed necrotic segment measuring approximately 1 m in length in the first patient. Both patients underwent proximal thrombectomy and endarterectomy, with excision of the necrotic bowel in the first patient. The patient who underwent enterectomy recovered well and was discharged 2 weeks postoperatively. Unfortunately, he was lost to follow-up after 3 months. The patient without transmural intestinal necrosis showed significant reduction in abdominal pain and distention postoperatively, although he developed severe diarrhea and hypoproteinemia. Postoperative CTA showed persistent occlusion of a short segment of the SMA trunk. However, a collateral pathway was detected around the occluded segment. A balloon-expandable stent was implanted subsequently into the occluded SMA segment, and the patient recovered uneventfully, without recurrent diarrhea or abdominal pain after stent implantation. Follow-up CTA confirmed stent and SMA patency 12 months later. 18
Correlation Analysis of Imaging Features and Clinical Manifestations
Mean lengths of dissection and the completely occluded segments were 59.22 ± 13.75 mm and 20.77 ± 8.5 mm, respectively. No significant correlation was observed between the length of dissection and abdominal pain intensity (rs = 0.206, P = .22). Similarly, no positive correlation was observed between the length of the occluded segment and abdominal pain intensity (rs = 0.018, P = .82) (Figure 2A, B). A, B: Neither the length of the occluded or dissected segment showing a correlation with abdominal pain scores. C, D: The group with definite collateral circulation development showing significantly lower abdominal pain scores and shorter time until pain relief (P < .05).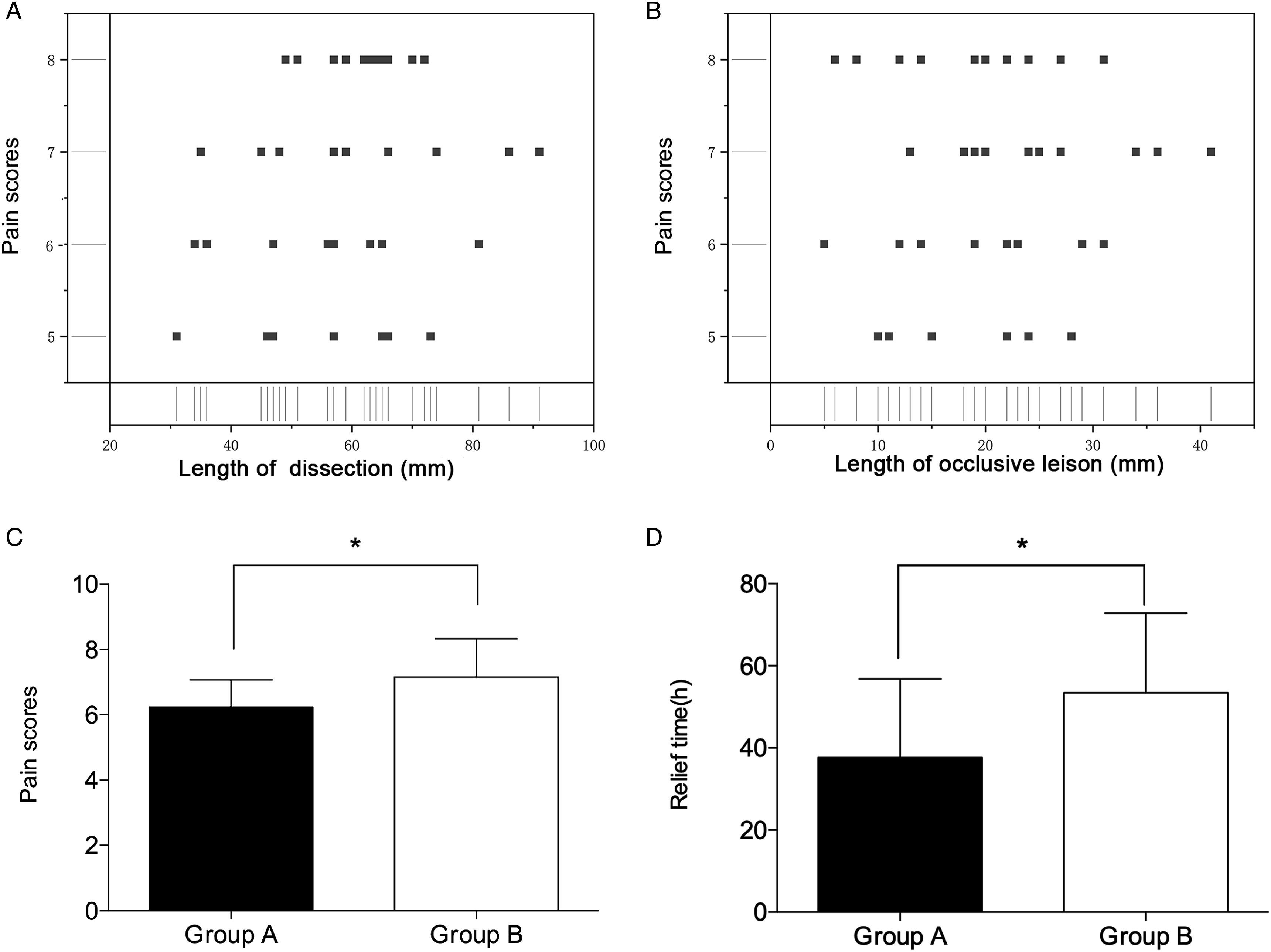
We observed the inferior mesenteric artery (IMA) and the arc of Riolan (AOR) served as collateral pathways in some patients and investigated the possible association between symptoms and collateral circulation. Based on radiologically documented evidence of AOR on admission, patients who received conservative treatment were categorized into two groups as follows: patients with a clearly visible complete AOR were classified into Group A (n = 17), and those without a clearly visible AOR into Group B (n = 18). We performed intergroup comparison of abdominal pain scores and symptom relief times. Pain scores were lower in Group A than in Group B (P < .05), and time until pain relief was also shorter in Group A (P < .05) (Figure 2C, D). Neither patient who underwent surgery showed any clearly visible collateral vessels. Notably, the vessel distal to the occluded segment did not show contrast filling (Figure 1H).
Follow-up Results
Patients who received conservative treatment did not show complete revascularization of the true lumen before discharge. Partial revascularization of the true lumen was observed in 14 patients; the true lumen remained occluded in the others. All patients underwent follow-up (mean follow-up duration 14.83 ± 8.90 months).
Most patients din not show symptom recurrence during one-year follow-up, except for one patient who had recurrent abdominal pain one month after discharge. CTA revealed re-occlusion of the partially recanalized SMA; however, collateral vessels were visualized in this patient, who received conservative treatment for a week until complete resolution of the abdominal pain. Three patients, including the patient who underwent enterectomy, were lost to follow-up after one year. These patients underwent telephonic follow-up 6 months after discharge and did not report any discomfort. However, they were not available for follow-up thereafter. CTA performed at one-year follow-up revealed completely revascularized SMA in 6 patients, including in the patient who underwent stent implantation. The collateral circulation became inconspicuous in some patients following progressive vascular remodeling. Partial remodeling of the SMA occurred in 16 patients, who did not show any aneurysmal dilatation of the false lumen. The SMA remained occluded in 12 patients; however, distinct collateral circulation was observed in these cases. (Figure 3) Summary of clinical profiles.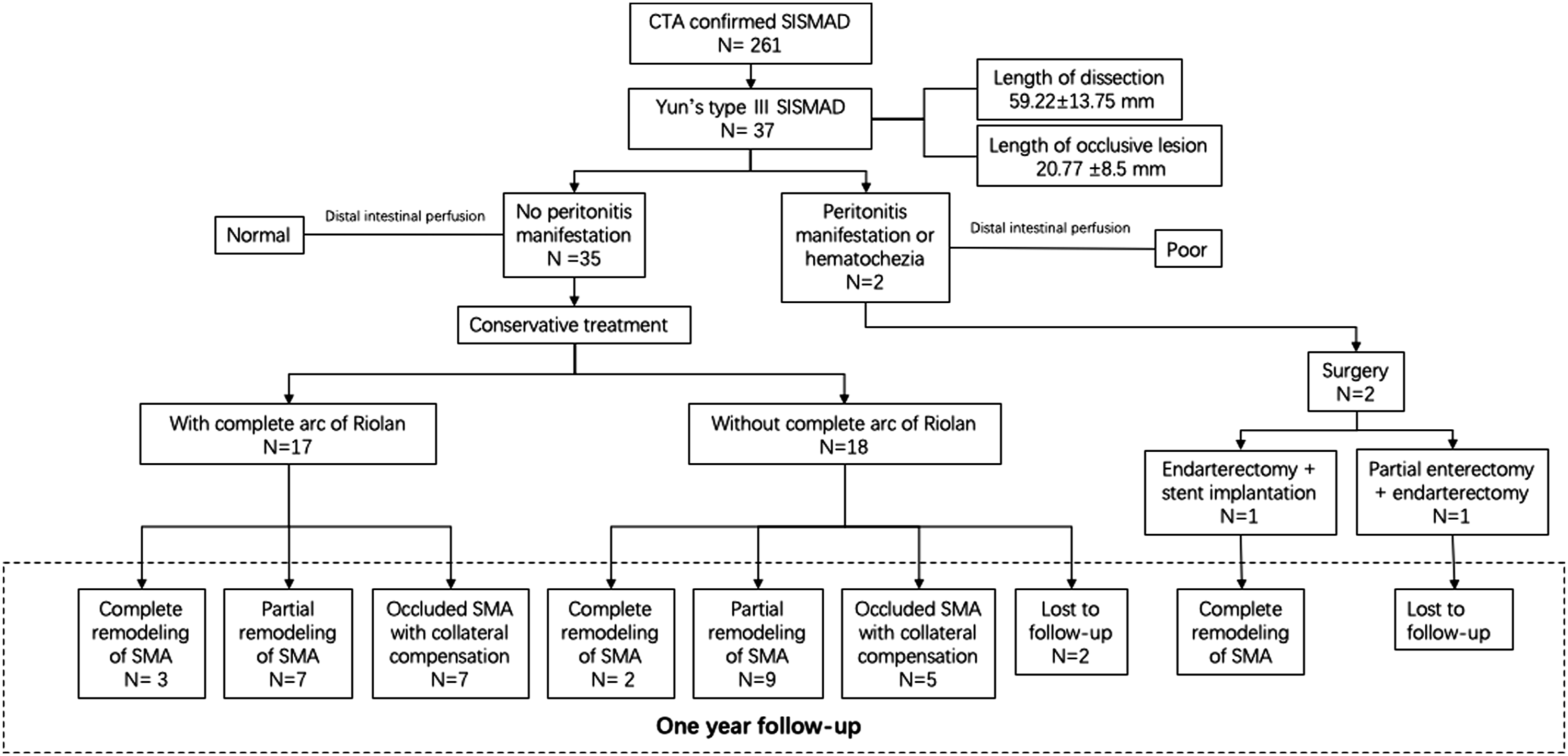
Discussion
In this study, most patients with Yun’s type III SISMAD (94.6%) showed satisfactory outcomes following conservative management except two patients who presented with severe intestinal ischemia on admission. Yun’s type III SISMAD may occasionally be misdiagnosed as SMA embolism or thrombosis, which are well-known catastrophic conditions that occur secondary to reduction in intestinal blood flow. Researchers have attempted to determine why SISMAD with total true lumen occlusion is relatively more benign than other causes of acute mesenteric ischemia. Yun et al. attributed the benign nature of this condition to the development of collateral circulation during gradual thrombotic occlusion of the SMA. 4 The vascular supply of the SMA includes collateral flow from the celiac artery, IMA, marginal arteries. In this study, some patients showed clearly visible collateral vessels on admission. Most collateral pathways originate from the IMA through the AOR. The AOR is an inconsistent artery that connects the middle colic branch of the SMA to the left colic branch of the IMA and forms a short loop that runs close to the root of the mesentery. Usually, the AOR is difficult to detect on CTA because it contains a small volume of blood or may even contain no blood. Insufficient blood flow through the SMA triggers gradual compensatory expansion of the AOR, which function as the major collateral vessel. In addition to the AOR, the celiac artery may also supply blood via the pancreaticoduodenal arc. Unlike acute the onset of SMA embolism, the true lumen of Yun’s type III SISMAD undergoes compression following gradual enlargement of the false lumen and thrombosis, which provides adequate time for the establishment of collateral circulation.
Previous studies have reported a correlation between abdominal pain and the length of dissection. 4 However, in this study, we did not observe a correlation between abdominal pain and the length of the dissection or occluded segments. We speculated that intestinal ischemia may be the main contributor to abdominal pain in patients with Yun’s type III SISMAD. Early development of collateral circulation and recanalization of the true lumen led to resolution of abdominal pain and prevented catastrophic intestinal ischemic necrosis in our patient.
Therapy is aimed at provision of adequate time to establish collateral circulation, promote true lumen remodeling, and minimize the demand for mesenteric blood supply. Most patients with Yun’s type III SISMAD respond favorably to optimal conservative treatment with close follow-up, and show good prognosis. 19 Both anticoagulant and antiplatelet therapies are considered to have adverse effects on false lumen thrombosis and vascular remodeling. 20 However, the false lumen tends to be completely thrombotic with a completely occluded true lumen in patients with Yun’s type III SISMAD. In this study, we routinely used anticoagulation therapy to prevent thrombosis of collateral vessels and of the potential true lumen. Alprostadil, a vasodilator, that inhibits platelet aggregation also prevents formation of thromboxane A2 and protects vascular endothelial cells; therefore, we administered this drug during the early stages to prevent bowel ischemia. Although evidence-based medicine does not conclusively establish its beneficial effects, patients did not show adverse reactions and were effectively cured.
Previous studies have reported instances of fail conservative treatment for SISMAD. In our opinion, the failure rate of conservative treatment may have been overestimated, which may be attributable to premature discontinuation of conservative treatment. The relatively short period of treatment may be inadequate for complete symptom resolution or dissection remodeling. Dong et al. reported that five patents who failed endovascular treatment were successfully cured after subsequent conservative therapy. 21 Based on our experience, conservative treatment may be continued prudently in patients without evidence of bowel necrosis. However, patients who receive conservative treatment may be at risk for complications associated with acute bowel ischemia, particularly among those with Yun’s type III SISMAD. Timely identification of these patients and early revascularization before progression of ischemia are lifesaving measures. 22 Evaluation of distal blood flow may be more important than estimation of the length of dissection and degree of true lumen stenosis.
Owing to the low incidence of adverse effects and high success rate associated with this approach, endovascular stent placement is increasingly preferred as minimally invasive treatment for patients with SISMAD, who are unresponsive to conservative management. However, technical failure is not uncommon during cannulation of the true lumen in type III SISMAD. 23 Dong et al. 24 reported that among 16 patients who underwent stent implantation, the procedure failed in three patients with Yun’s type III SISMAD in whom the guide-wires could not be advanced into the completely thrombosed true lumens. Stent implantation is challenging in patients with a long dissection segment without a healthy distal landing zone. Moreover, false lumen thrombosis may result in distal SMA embolism. Exploratory laparotomy is preferred over endovascular treatment for patients with severe bowel ischemia and even bowel necrosis. We recommend that the SMA should be dissected longitudinally to confirm the true lumen. A Fogarty catheter can easily remove the partial proximal intimal flap with the thrombus in the false lumen. Notably, the distal intimal flap should be carefully sutured to the adventitia. In this study, the occlusion of a short segment of the SMA in the patient who underwent endarterectomy may be attributable to unsuccessful fixation of the distal intimal flap. Collateral vessels should be preserved to the greatest extent intraoperatively. Stent implantation may be useful for patients with obstructed blood flow secondary to a post-laparotomy intimal flap.
Limitations
Following are the limitations of this study: (a) The single-center retrospective design and the relatively small sample size are drawbacks of the study. (b) Whether the distal arterial blood flow is useful as an indicator to screen high-risk patients needs to be further validated, because this study included only two patients who underwent surgery.
Conclusion
This study highlights that conservative treatment is useful as the first-line therapy in most patients with Yun’s type III SISMAD, except in those with signs of peritonitis. Patients’ symptoms are not correlated with the length of dissection or occluded segments, and complete AOR contributes to symptoms relief. Poor distal blood flow may be an important indicator for identification of patients at a high risk of intestinal necrosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.