
Abstract
Spontaneous rupture of the iliac vein is a rare cause of retroperitoneal hematoma. A misdiagnosis may delay the treatment and consequently put the patient in a life-threatening emergency. We report the case of a 73-year-old woman who presented with hemorrhagic shock from bleeding caused by a large left retroperitoneal hematoma. She was successfully treated with an endovascular approach by using a double bare stent technique. An extensive review of the literature was conducted and a total 44 articles with 50 patients were identified. Among these patients, 88.2% were women, 94.1% presented with a left-sided rupture, and the mortality rate was 13.7%. Spontaneous iliac vein rupture was more likely to occur in the left side in female patients. Conservative treatment was an option in hemodynamically stable patients. Exploratory laparotomy and surgical iliac vein repair was necessitated in most patients. Endovascular treatment including placement of covered stent and coil embolization had been widely used to treat spontaneous vein rupture since 2003. Double bare stent technique was also an effective alternative if a suitable covered stent was unavailable.
Introduction
Spontaneous iliac vein rupture (SIVR) is a rare and under-recognized clinical emergency. Patients may present with a retroperitoneal hemorrhage that is often misdiagnosed. Urgent exploratory laparotomy was often performed in these patients, but with the growing experience in the fields of endovascular technique, more and more endovascular repair has been used in the past 2 decades. Covered stents were commonly deployed across the rupture site to seal the leakage. However, a suitable size is not always available, especially during an emergency setting.
In this study, we report an elderly woman who presented with a large retroperitoneal hematoma and hemorrhagic shock caused by SIVR. The presence of DVT proximal to the rupture was also identified. Our report details the successful treatment of SIVR with double bare stent technique. The patient has agreed with the publication of this case report and written consent has been obtained.
Case Report
A 73-year-old female was admitted to our emergency department due to severe abdominal pain persisted for 10 hours and accompanied with transient loss of consciousness. She was hemodynamically unstable upon arrival. Her vital signs were 59/32 mmHg blood pressure, and 139 beats/min pulse rate. The physical examination was significant for a tender, non-pulsatile abdominal mass (approximately 10-cm x 15-cm in size) at the left lower quadrant and a swollen left lower limb with increased tension. Her left dorsalis pedis and posterior tibial artery pulses were palpable. She has a past medical history of hypertension for 10 years which was poorly controlled. Biochemical results revealed an elevated white blood cell count (15.39 × 109/L), low platelet count (70 × 109/L), low hemoglobin level (64 g/L), elevated D-dimer (24.2 mg/L), and prolonged activated partial thromboplastin time (APTT) (53.20s). Her computed tomography (CT) report revealed a retroperitoneal hematoma measuring 14.8-cm × 6.3-cm, along with fluid accumulation in the abdominal cavity.
We immediately initiated resuscitation with crystalloid and blood transfusion to manage her hemorrhagic shock. She was transferred to the intensive care unit (ICU) once her blood pressure has reached 86/55 mmHg. A contrast-enhanced computed tomography was arranged, which revealed a large retroperitoneal hematoma measuring 4.6-cm × 11.1-cm × 19.2-cm and accumulation of blood and fluid in the abdominopelvic cavity. Suspected left iliac vein thrombosis was also noted on the CT scan (Figure 1). Abdominal CT revealed a retroperitoneal hematoma occupying the space from below the left kidney to the entire pelvic cavity.
An urgent angiogram and venogram were performed to identify the source of bleeding. Aortoiliac angiography was performed using left femoral access. No contrast extravasation was revealed. A small aneurysm was found on the distal end of a lumbar artery branch, no contrast leakage identified. It was embolized with 2 3-mm × 3.3-mm coils (VortX Diamond-18, Boston Scientific, USA).
Venogram using right femoral access was performed. A .035″ guidewire was advanced to the left iliac vein with the support of a 5F Cobra catheter (Cordis, USA), thrombosis of the left common iliac and external iliac veins was visualized, and significant contrast extravasation was found within the left external iliac vein (Figure 2(a)). Left external iliac vein rupture was confirmed. The external iliac vein was measured 10 mm in diameter, there was no suitable covered stent available. Therefore, we attempted to place 2 overlapped bare stent to cover the rupture. Angiography revealed significant contrast extravasation from the left external iliac vein (A). Angiography performed after covering the rupture site with double bare stent technique revealed a patent left common iliac vein without contrast extravasation (B).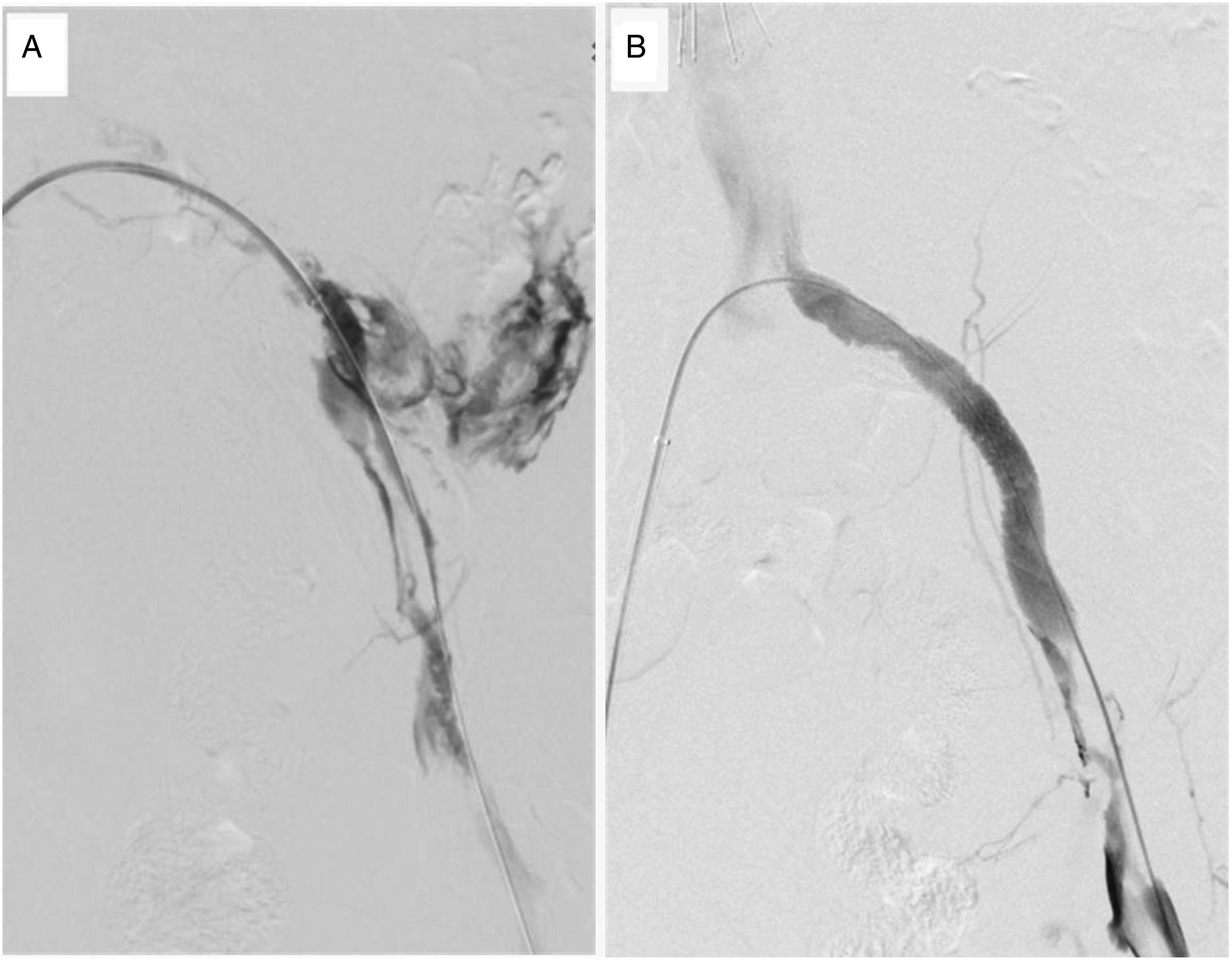
Left iliac vein compression syndrome (VCS) was also suspected since resistance was met during advance of the guidewire and catheter. Venoplasty of the left common iliac vein was performed using a 10-mm x 80-mm balloon (Ultraverse, Bard, USA), stenosis was seen on fluoroscopy during venoplasty which was consistent with VCS. A 12-mm × 90-mm stent (Wallstent, Boston Scientific, USA) was placed at the proximal segment of the left iliac vein to cover the rupture site. Another 12-mm × 60-mm stent (Wallstent, Boston Scientific, USA) was placed to overlap the rupture site. The length of overlap coverage was approximately 5-cm. There was no contrast extravasation from the left iliac vein on venogram (Figure 2(b)). After placement of an inferior vena cava filter (Option Elite, Argon, USA), pharmacomechanical thrombectomy (PMT) was then performed using a 6F catheter (AngioJet, Boston Scientific, USA) Completion venography results showed the left iliac vein was patent without filling defect or contrast extravasation.
Anticoagulation (Nadroparin 4000U q12H) and blood transfusion were administered postoperatively. Her postoperative blood pressure was within the normal range. On the third postoperative day, her hemoglobin level has raised to 91 g/L. Physical examination found an obvious reduction of tension in her left lower limb. The circumferences of her thigh (15-cm above the knee) and calf (10-cm below the knee) have reduced by 4.1-cm and 2.0-cm respectively. Postoperative duplex ultrasound showed her left iliac, femoral, and popliteal veins were patent. She was discharged and prescribed with oral rivaroxaban 20 mg QD.
Follow up CT at 1 and 3 months after the procedure showed gradual size reduction of the retroperitoneal hematoma (Figure 3). USG of the lower limb showed patency of the stent and venous system of the left lower limb. She had successful IVC filter retrieved 3 months after the operation. CT scan results from the same segments performed upon admission (A), 1-month (B), and 3-month (C) post operation reveals gradual size reduction of the retroperitoneal hematoma.
Discussion
Summary of characteristics of the included studies on spontaneous iliac vein rupture.
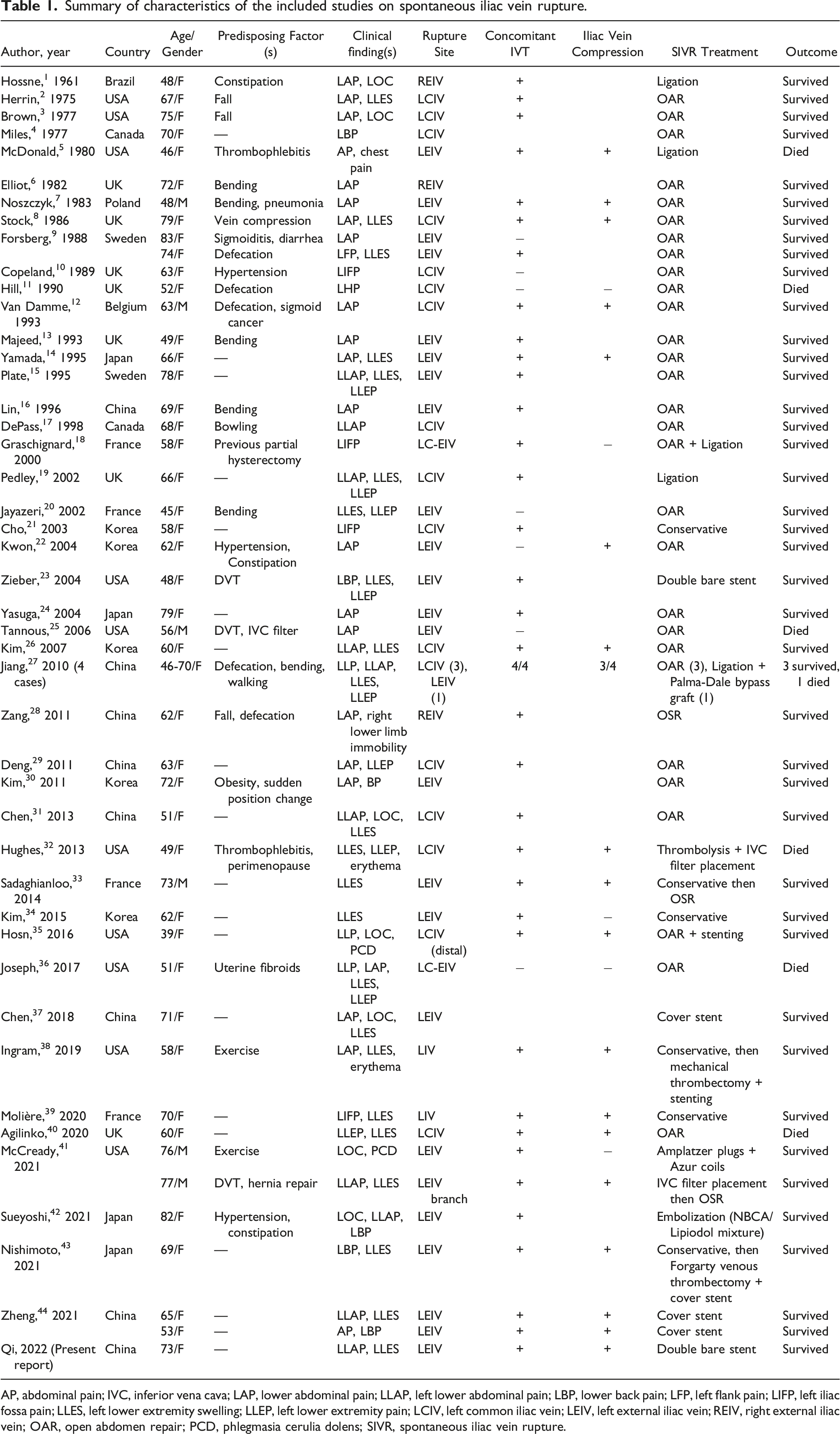
AP, abdominal pain; IVC, inferior vena cava; LAP, lower abdominal pain; LLAP, left lower abdominal pain; LBP, lower back pain; LFP, left flank pain; LIFP, left iliac fossa pain; LLES, left lower extremity swelling; LLEP, left lower extremity pain; LCIV, left common iliac vein; LEIV, left external iliac vein; REIV, right external iliac vein; OAR, open abdomen repair; PCD, phlegmasia cerulia dolens; SIVR, spontaneous iliac vein rupture.
The exact etiology of the disease is still unknown, but various theories have been suggested, namely the increased fragility of vessel walls and increased venous pressure in the iliac veins. Estrogen is known to promote vessel compliance, and postmenopausal women deplete in them, consequently resulting in a loss of such protective effect, and causing the weakening of the venous wall. 25 Chronic inflammation and venous thrombophlebitis can potentially cause the venous wall to lose its elasticity. 45 In our literature review, we found that 75% of patients had a concomitant venous thromboembolism. Many of the patients without concomitant DVT might have proximal venous obstruction. Absent venous hypertension, it seems highly unlikely that such rupture could occur, as intra-abdominal pressure usually approximates or exceeds normal venous pressures and would therefore tamponade any tendency for bleeding or hematoma expansion. Currently, we are una ble to determine whether the thrombus or rupture existed first. However, thrombophlebitis remains 1 of the potential causative factors that cannot be ignored. Zhang et al. 46 reported that 62.5% of patients have displayed such histopathological evidence. Some studies described that the iliac vein was already too weak and beyond repair when surgeons found its defect during exploratory laparotomy.18,19 May-Thurner syndrome is a condition leading to venous outflow obstruction due to extrinsic venous compression in the iliocaval venous territory. This makes it 1 of the common causes of venous hypertension. 38 The syndrome was especially recognized and identified in the case studies published in the recent 10 years (2010-2021). In this group, 75% (18/24) were reported to have concomitant iliac vein compression. Additionally, certain actions that may suddenly increase venous pressure, such as hurdling, squatting, strenuous exercise, and defecation, are common triggers of iliac vein rupture.
Spontaneous iliac vein rupture often presents as persistent pain in the lower left abdomen, accompanied with hypotension. Patients who experience massive bleeding may present with syncope first. In most cases, patients have an underlying deep vein thrombosis (DVT) that causes swelling of the lower limbs. In our review, we found that 50% (25/50) of the patients presented with left lower limb swelling. Tannous et al. 25 found in their review of 33 cases, 79% had a concomitant venous thromboembolism. CT scan and MRI are useful imaging modalities in the diagnosis of iliac vein rupture. In most of the cases, retroperitoneal hematoma could be identified on CT scan or MRI. Contrast extravasation can be seen on CT scan if there is active bleeding. However, it is difficult to differentiate venous rupture from arterial bleeding. Duplex ultrasound has a low sensitivity in diagnosis of iliac vein rupture. Venogram is the golden standard for diagnosis of iliac vein rupture. However, it is invasive and may not be immediate available in the emergent setting.
Conservative treatment is an option that is only applicable to hemodynamically stable patients.21,34,38,39 Traditional laparotomy and surgical iliac vein repair is the most commonly used open surgical approach. Endovascular treatment of SIVR was first reported in 2003. Since then, a large variety of devices including covered stent, with or without embolization coils and glue have been used. The bare stent technique for treatment of SVIR has been reported by Zieber et al. 23 previously. It is effective to stop bleeding by cover the rupture site, decreasing venous pressure, restoration of venous blood flow and allowing the hematoma surrounding the vein to tamponade further bleeding. In this patient, we used 2 overlapped bare stents instead of a covered stent beacause a 13-mm diameter covered stent was not immediately available. According to a multi-institutional international practice pattern survey, most common stent diameters that used for endovascular iliocaval reconstruction were 14-mm in the common iliac vein, and 12-mm in the external iliac vein. 47 We used 2 12-mm diameter overlapped Wallstents in this case, landing from common iliac vein to external iliac vein. The size was suitable for external iliac vein. However, a 12 mm diameter stent might be a little undersized for common iliac vein. In this patient, there was suspected left iliac vein compression during venoplasty. Therefore, we chose to use 2 12-mm diameter stents. The first Wallstent was deployed at left common iliac vein through left femoral vein access. The proximal end of the second Wallstent was 2-3 cm proximal to the rupture site. There were overlapped stents covering the rupture site at least 2 cm proximally and 2 cm distally. We deployed 2 overlapped stents to cover the rupture and subsequently performed PMT to remove the thrombosis. As there was still contrast extravasation on venogram, control of the bleeding was the first priority in the emergency setting. PMT would increase the risk of bleeding if it was done before iliac vein stenting. The stent was patent after thrombectomy in this patient.
Conclusion
Spontaneous rupture of the iliac vein is a rare but life-threatening condition. Prompt diagnosis and early resuscitation are essential. Traditional laparotomy and surgical iliac vein repair is the most commonly used open surgical approach. Minimally invasive endovascular treatment has gained popularity in the past 2 decades with a satisfactory outcome. In selected cases, endovascular approach with double bare stent placement is an effective treatment option.
Footnotes
Author Contribution
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient has agreed with and consented for the publication of their case.