
Abstract
Background
Among tandem occlusions, atherosclerotic cervical internal carotid artery occlusion (ACICAO) can be technically challenging and associated with its unique complications. We evaluated our experience with endovascular treatment (EVT) of ACICAO in the setting of acute ischemic stroke.
Methods
In total, 154 consecutive patients who underwent EVT for acute anterior circulation stroke at our institute were retrospectively reviewed. Patients with tandem ACICAO were analyzed in this study. Procedures, recanalization rates, complications, and prognoses were evaluated.
Results
Ten patients (6%) of all 154 patients had ACICAO. In nine (90%) of the 10 patients, cervical lesions were successfully crossed and intervened upon. Four patients underwent stenting and five underwent angioplasty alone, followed by intracranial procedure. Eight patients (80%) achieved successful recanalization following mechanical thrombectomy for intracranial occlusion. However, one patient had massive subarachnoid hemorrhage during the procedure and another patient developed massive intracranial hemorrhage after EVT, both after stenting. Four of the five patients who initially underwent angioplasty alone subsequently underwent staged endarterectomy or stenting for residual stenosis on or after the next day. The single patient in whom the cervical lesion could not be crossed and another with reocclusion after EVT underwent a rescue bypass procedure due to persistent ischemic symptoms. After 90 days, four patients (40%) were functionally independent (modified Rankin scale score 0-2).
Conclusions
Our experience suggests that EVT for ACICAO is technically feasible; however, it involves the potential risk of several significant complications. To avoid serious hemorrhagic complications, cervical lesions may be better treated with angioplasty alone first.
Keywords
Introduction
Concurrent intracranial large vessel occlusion (LVO) and an extracranial carotid artery steno-occlusive lesion, termed “tandem occlusion”, is a complex stroke condition accounting for 10-20% of acute ischemic strokes due to LVO.1-4 As the natural history and effectiveness of intravenous thrombolysis are poor for tandem occlusion, endovascular treatment (EVT) and mechanical thrombectomy (MT) have been considered promising.5-7 However, the optimal treatment strategy for extracranial lesions remains controversial.8-10 Current guidelines briefly mention that EVT for tandem occlusion is reasonable when performing MT for LVO.11,12
Tandem occlusion is usually defined by the presence of severe stenosis or occlusion of the ipsilateral extracranial carotid artery in addition to the intracranial LVO; however, the degree of stenosis varies among studies (70-100% obstruction).1,3,4,6,7,13 The majority of occlusion in extracranial lesions occur due to atherosclerosis followed by arterial dissection (20%), and rarely include large thrombus and carotid web.10,14 Given this heterogeneity in lesion severity and etiologies, it may not be appropriate to apply a uniform treatment strategy for all tandem occlusions. In particular, atherosclerotic cervical internal carotid artery occlusion (ACICAO), in which blood flow to the distal artery is completely stopped due to an atherosclerotic plaque, can be technically challenging and associated with its unique complications. Recognizing this challenging occlusion type as a particular tandem occlusion group may contribute to our decision-making in clinical practice.
In this study, we describe our experience with EVT of ACICAO in the setting of acute ischemic stroke, focusing on treatment strategies, complications, and postoperative management.
Materials and Methods
Patient Selection
Consecutive patients who underwent EVT for acute anterior circulation LVO at our institution (Toyooka Hospital) between April 2015 and March 2018 were reviewed retrospectively. Those who had tandem ACICAO were analyzed in this study. The study term was selected as the period during which all interventional procedures were performed by the corresponding author as the lead operator. Our detailed protocol for acute ischemic stroke intervention has been previously reported.15-19 Based on angiography findings, ACICAO was defined as cervical internal carotid artery (ICA) occlusion due to an atherosclerotic plaque, in which blood flow to the distal artery was completely stopped. Our main EVT indications for tandem ACICAO were as follows: (1) <8 hours from symptom onset or <24 hours from the time the patient was last seen to be well in cases where the time of symptom onset was unknown; (2) presence of intracranial LVO; (3) lack of sufficient collateral blood flow; (4) mismatch between neurological symptoms on admission and findings on imaging; (5) a score of ≥6 on the Alberta Stroke Program Early Computed Tomography Score (ASPECTS) or ASPECTS-diffusion weighted imaging. Patients with mild symptoms (National Institutes of Health Stroke Scale (NIHSS) score ≤4) or severe comorbidities were excluded from the EVT indication for tandem ACICAO and were treated medically. Intravenous tissue plasminogen activator (tPA) was administered according to the Japanese Guidelines for the Management of Stroke. Informed consent was obtained from each patient or family member before performing the endovascular procedure. The study design was approved by our institutional review board (Toyooka Hospital ethics committee, reference number 122) and conducted in accordance with the Declaration of Helsinki.
EVT Procedures
Endovascular procedures for LVO at our institute have been previously reported.15-19 The concept of our treatment strategy for tandem ACICAO is shown in Figure 1. Earlier in this cohort, percutaneous transluminal angioplasty (PTA) and carotid artery stenting (CAS) were performed before treating the intracranial lesion (CAS first-antegrade approach), while, towards the end, only PTA was performed before intracranial lesion treatment (PTA first-antegrade approach without emergent CAS). In the cases of ACICAO, the retrograde approach (direct MT) was not adopted because it was considered to have more disadvantages than advantages. Treatment strategy for tandem atherosclerotic cervical internal carotid artery occlusion.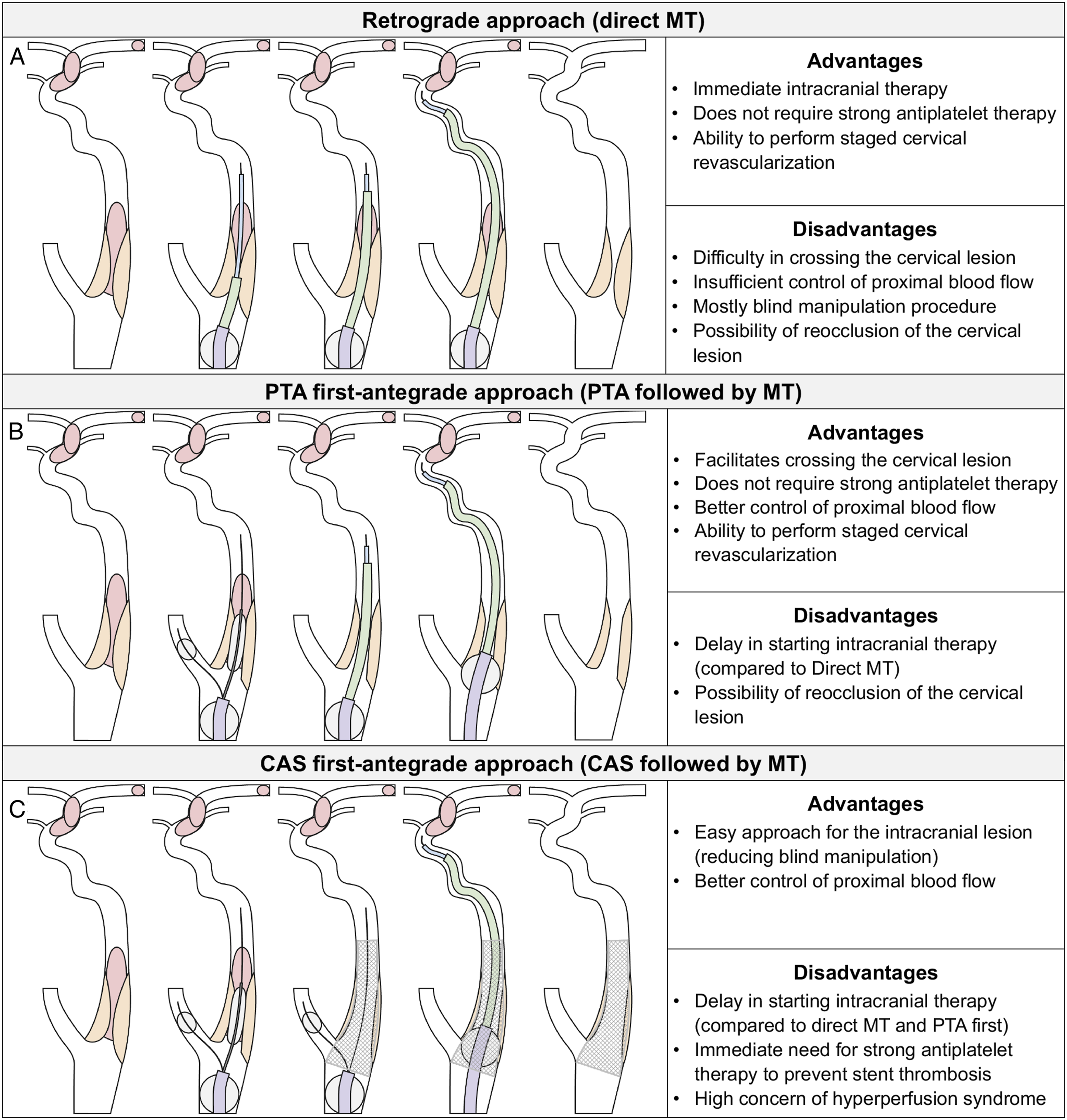
The ACIACAO lesion was crossed under proximal blood flow control using a balloon guide catheter placed in the common carotid artery. Blood flow in the external carotid artery was stopped by another balloon device whenever possible. The Carotid GuardWire Temporary Occlusion and Aspiration System (Medtronic, Minneapolis, MN, USA) was used as the first-choice device for external carotid artery occlusion. A stiff 14- or 18- micro guidewire was used to cross the cervical lesion. After lesion crossing, PTA was performed with a 3.0 mm or 3.5 mm balloon to provide passage for the treatment device through the cervical occlusion. In cases where CAS was performed, the Wallstent (Boston Scientific, Marlborough, MA) was subsequently placed. After the cervical lesion was dilated, a sufficient amount of blood was aspirated from the balloon guide catheter. Once the cervical ICA occlusion was recanalized, additional MT was performed for the remaining intracranial occlusion with the combined technique using the Penumbra aspiration catheter (Penumbra Inc., Alameda, CA), Trevo (Stryker, Kalamazoo, MI), and Solitaire stent retriever (Medtronic). In the case of the PTA first-antegrade approach, carotid angiography was repeated after MT, post-PTA was added if necessary, and acute CAS was avoided as much as possible.
Antiplatelet Therapy
If ACICAO was suggested, a loading dose of aspirin (300 mg) was administered through a nasogastric tube. Furthermore, when CAS was performed acutely, an additional loading dose of clopidogrel (300 mg) was administered. Transvenous antiplatelet agents such as GP IIb/IIIa Inhibitors were not used because they were not approved in our country. Patients receiving antiplatelet therapy before admission were administered with additional doses as needed. Antiplatelet agents were continued on the next day. Patients who underwent emergent CAS received dual antiplatelet therapy, and those who did not undergo emergent CAS continued with single-agent antiplatelet therapy.
Postprocedural Management
After the EVT procedure, all patients were monitored in the intensive care unit. Systolic blood pressure was maintained at <120 mmHg after revascularization. Computed tomography immediately after and within 24 hours of treatment were routinely performed to assess intracranial hemorrhage. Magnetic resonance imaging and neck echocardiography were also performed within 24 hours to evaluate the patency of the vessels. Additional staged revascularization was basically planned after a week or more, if possible, but the additional intervention was carried out promptly when the examination or symptoms warranted urgent treatment.
Outcome Assessment
The degree of recanalization after EVT was evaluated using the modified thrombolysis in cerebral infarction (TICI) score. Symptomatic intracranial hemorrhage (ICH) was considered in cases with subarachnoid hemorrhage (SAH) or intracerebral hemorrhage with an increase in the NIHSS score by ≥4 points from baseline within 24 hours of treatment. Clinical prognosis was assessed using the modified Rankin scale (mRS) score at 90 days. Other issues, such as complications and staged revascularization (additional treatment procedures), were also evaluated.
Statistical Analysis
The relationship between the time from onset and outcome was evaluated using Pearson’s correlation coefficient and regression analysis. Statistical analysis was performed with free open-source software (R4.1.3; R Foundation for Statistical Computing; http://www.r-project.org).
Results
Patient Characteristics
Summary of Patients.
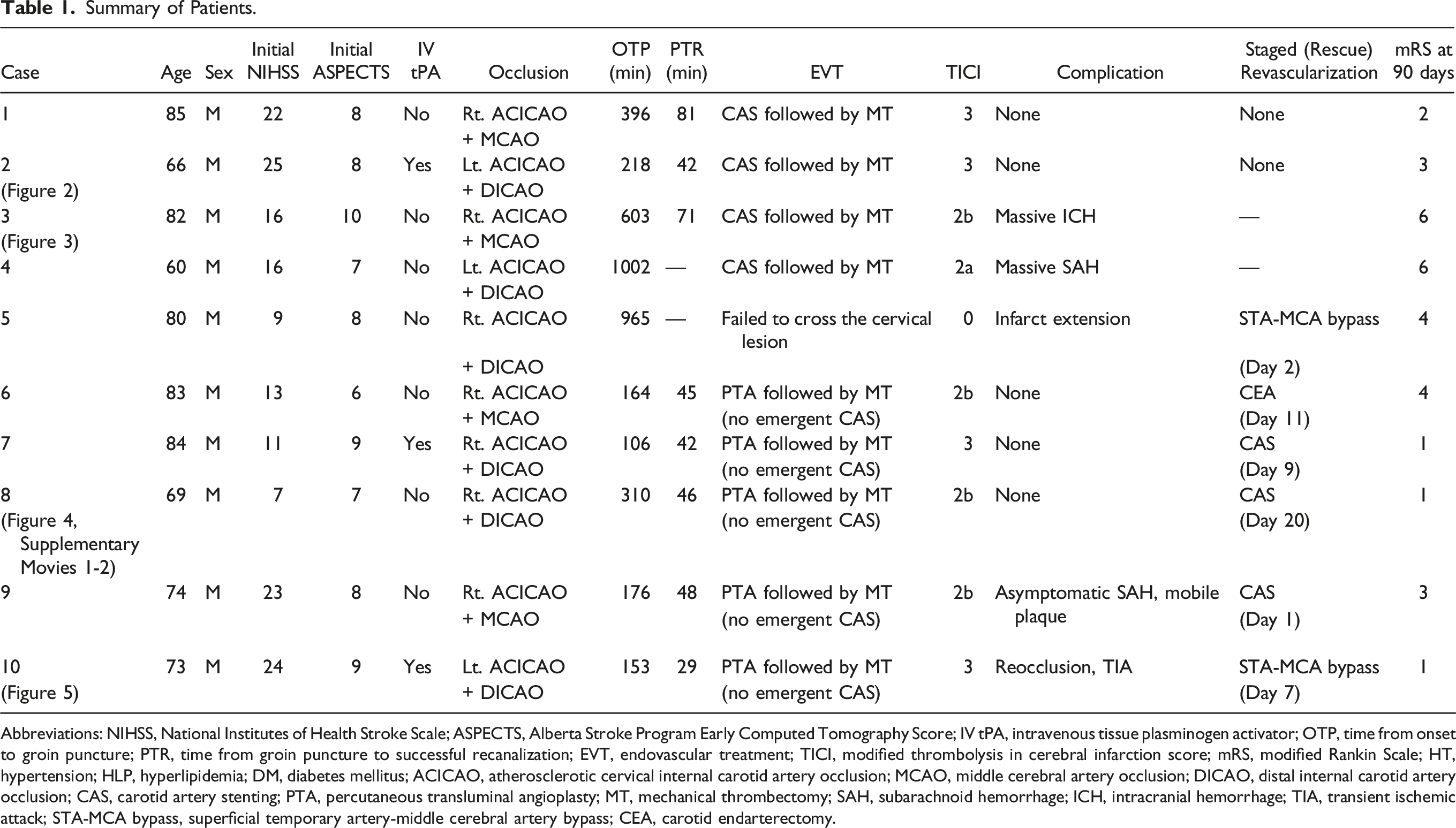
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; ASPECTS, Alberta Stroke Program Early Computed Tomography Score; IV tPA, intravenous tissue plasminogen activator; OTP, time from onset to groin puncture; PTR, time from groin puncture to successful recanalization; EVT, endovascular treatment; TICI, modified thrombolysis in cerebral infarction score; mRS, modified Rankin Scale; HT, hypertension; HLP, hyperlipidemia; DM, diabetes mellitus; ACICAO, atherosclerotic cervical internal carotid artery occlusion; MCAO, middle cerebral artery occlusion; DICAO, distal internal carotid artery occlusion; CAS, carotid artery stenting; PTA, percutaneous transluminal angioplasty; MT, mechanical thrombectomy; SAH, subarachnoid hemorrhage; ICH, intracranial hemorrhage; TIA, transient ischemic attack; STA-MCA bypass, superficial temporary artery-middle cerebral artery bypass; CEA, carotid endarterectomy.
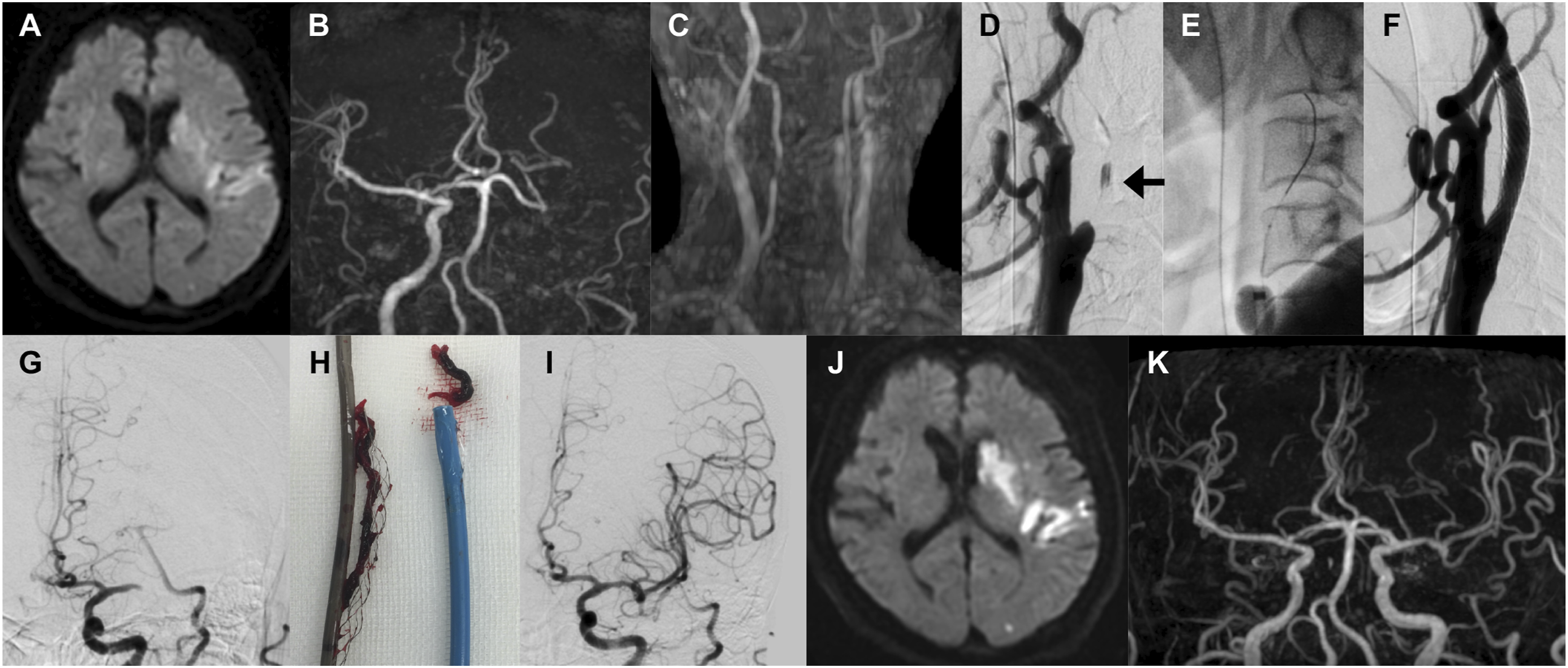
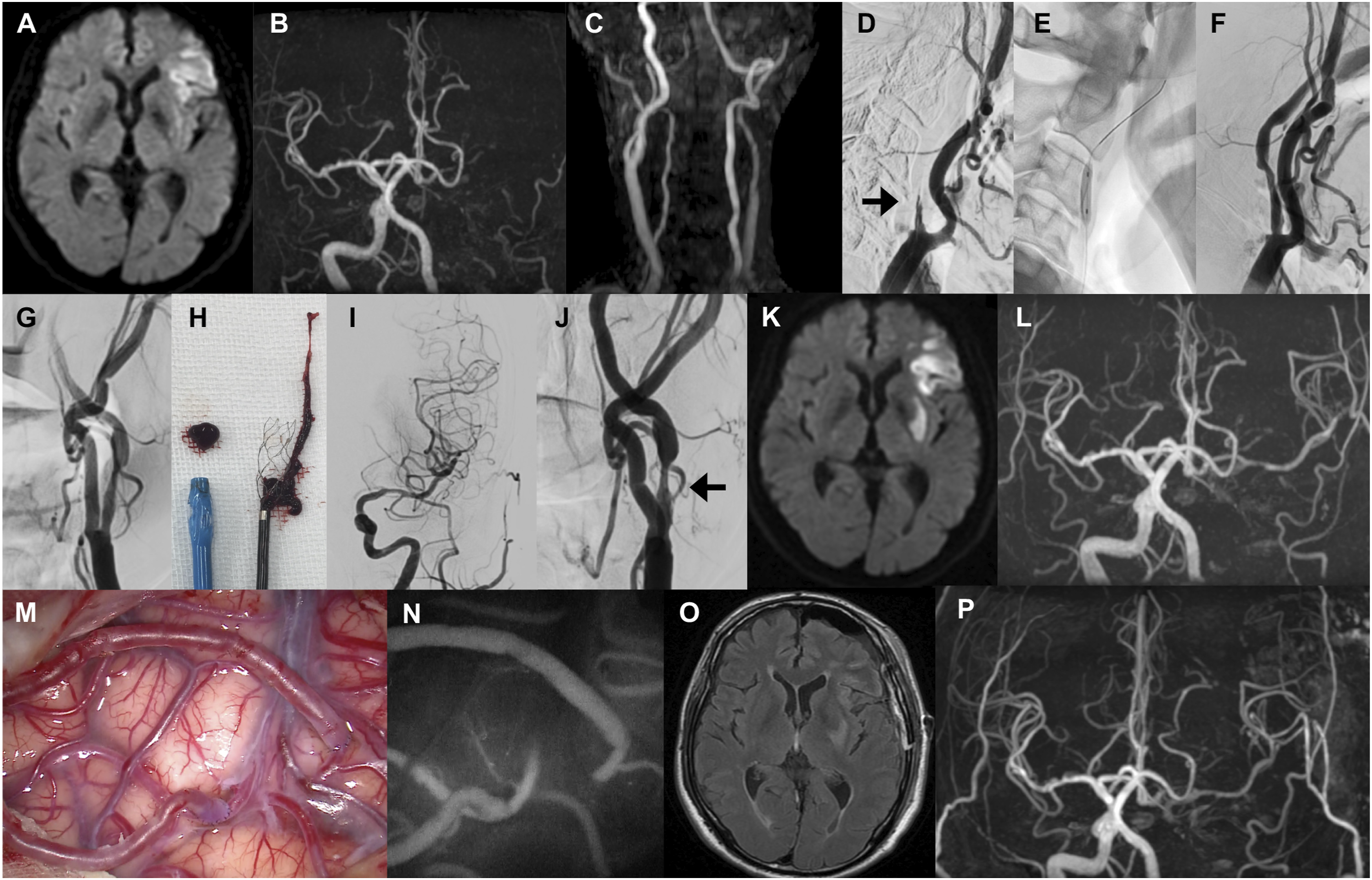
Illustrative case of a patient who underwent CAS followed by MT (Case 2). (A, B, C) Emergency MRI showing an acute ischemic lesion with occlusion of the left cervical and distal internal carotid artery. (D) Initial angiography showing occlusion of the left cervical internal carotid artery with a calcified atherosclerotic lesion and stagnation of a small amount of contrast medium (arrow). (E, F) The cervical lesion was crossed, and CAS was successfully performed. (G) Angiography showing residual occlusion of the left middle cerebral artery. (H) MT was performed with the combined use of a stent retriever and an aspiration catheter. (I) Postprocedural angiography showing complete recanalization. (J, K) MRI on the day after the procedure showing successful recanalization without any significant infarct extension. Abbreviations: CAS, carotid artery stenting; MT, mechanical thrombectomy; MRI, magnetic resonance imaging.
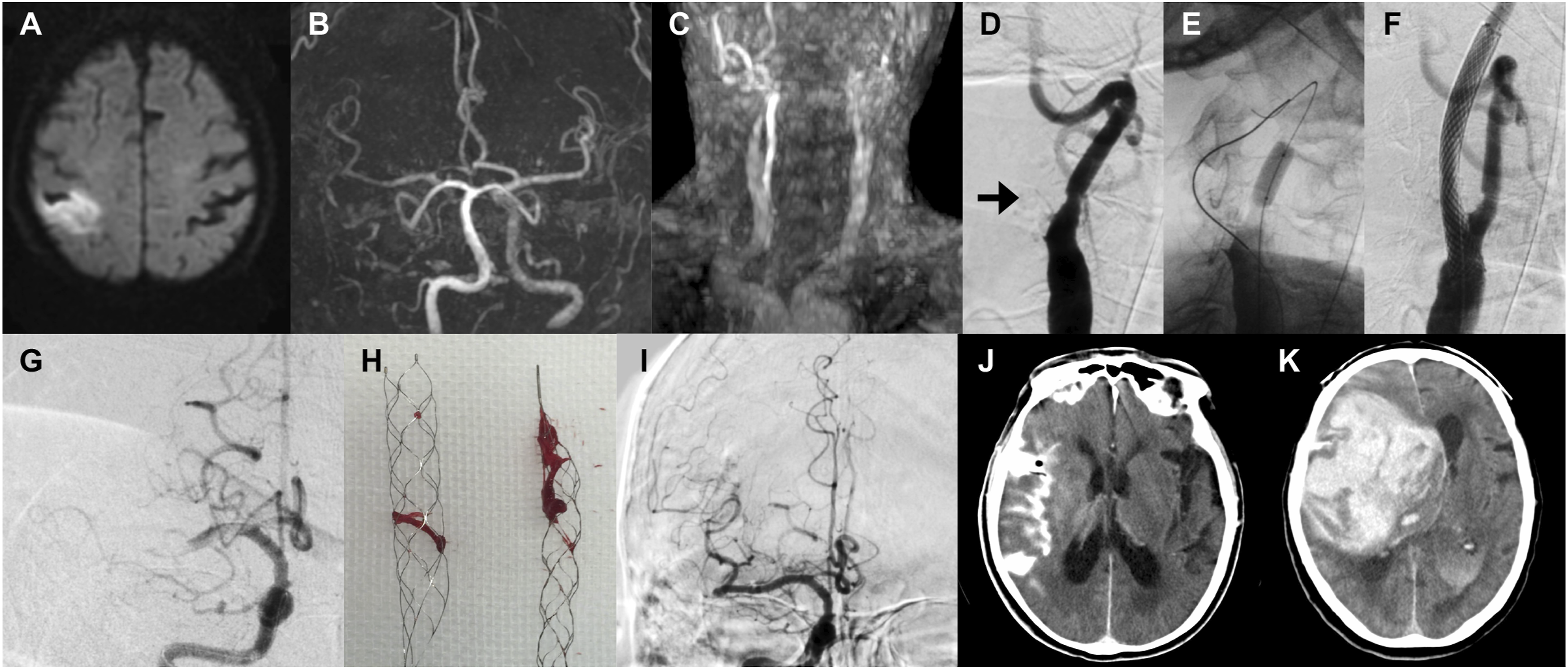
Illustrative case of a patient who underwent CAS followed by MT and subsequently developed intracranial hemorrhage (Case 3). (A, B, C) Emergency MRI showing an acute ischemic lesion and occlusion of the right cervical internal carotid and distal middle cerebral arteries. Note that the contralateral cervical carotid artery is also poorly visualized. (D) Initial angiography showing occlusion of the right cervical internal carotid artery with a calcified atherosclerotic lesion (arrow). (E, F) The cervical lesion was crossed, and CAS was successfully performed. (G) Angiography showing residual occlusion of the right middle cerebral artery. (H) MT was performed with the combined use of a stent retriever and an aspiration catheter. (I) Postprocedural angiography showing successful recanalization. (J) Computed tomography immediately after the procedure showing subarachnoid hemorrhage. (K) Computed tomography 2 hours after the procedure showing massive intracerebral hemorrhage. Abbreviations: CAS, carotid artery stenting; MT, mechanical thrombectomy; MRI, magnetic resonance imaging.
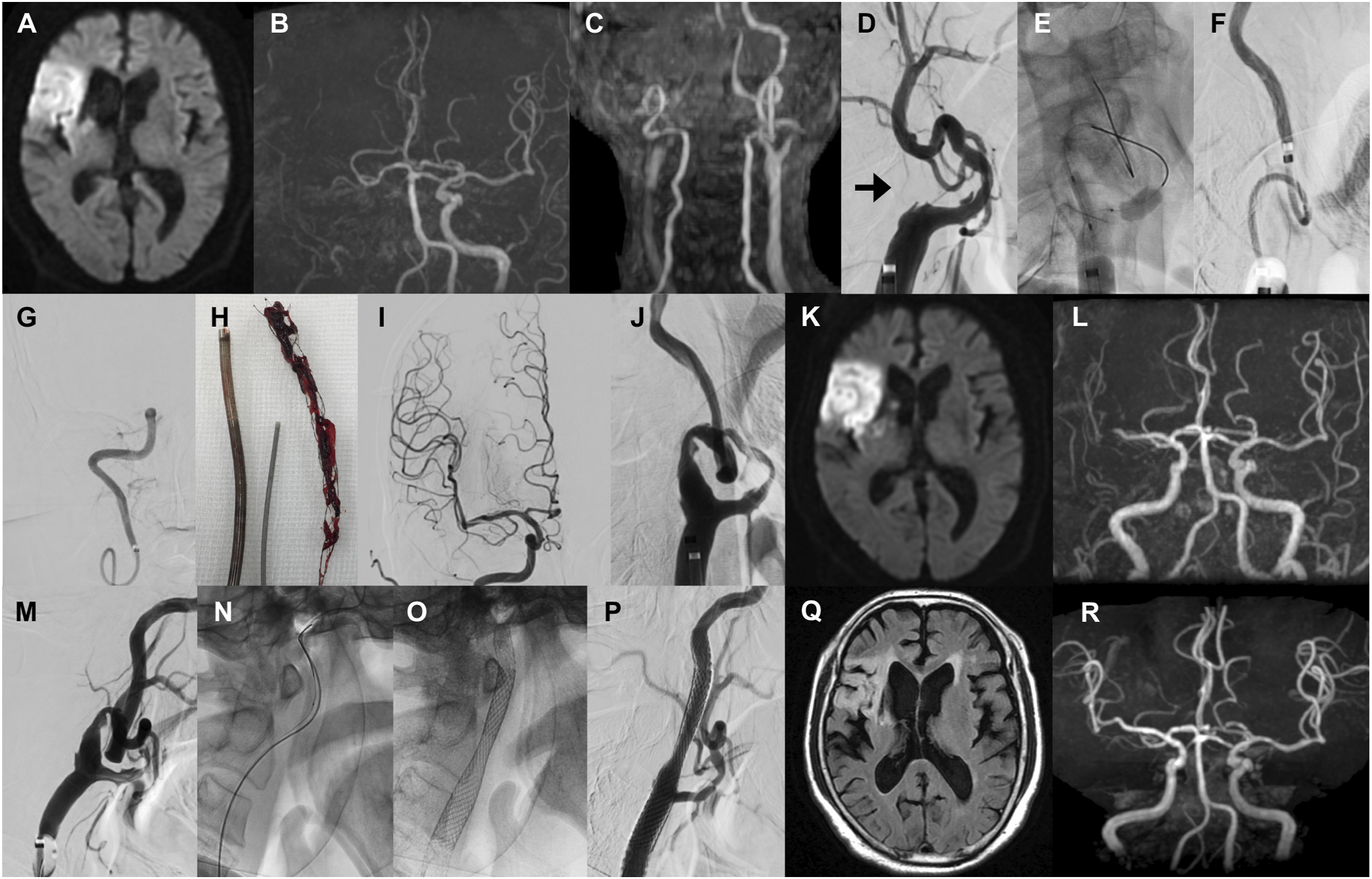
Illustrative case of a patient who underwent PTA followed by MT and CAS after the acute phase (Case 8). (A, B, C) Emergency MRI showing an acute ischemic lesion and occlusion of the right cervical and distal internal carotid artery. (D) Initial angiography showing occlusion of the right cervical internal carotid artery with a calcified atherosclerotic lesion (arrow). (E, F) The cervical lesion was crossed, and PTA was performed. (G) Angiography showing residual occlusion of the right distal internal carotid artery. (H) MT was performed with the combined use of a stent retriever and an aspiration catheter. (I) Postprocedural angiography showing successful recanalization. (J) Final angiography after additional PTA showing residual stenosis. (K, L) MRI on the day after the procedure showing recanalization, though slightly poor opacification of the distal middle cerebral artery, without any significant infarct extension. (M, N, O, P) CAS was successfully performed 20 days after the initial procedure. (Q, R) MRI on the day after the CAS procedure showing no significant infarct extension compared to that on initial MRI on admission, with successful revascularization. Abbreviations: CAS, carotid artery stenting; MT, mechanical thrombectomy; MRI, magnetic resonance imaging; PTA, percutaneous angioplasty.
Illustrative case of a patient who underwent PTA and MT and subsequently developed reocclusion and was treated by bypass surgery (Case 10). (A, B, C) Emergency MRI showing an acute ischemic lesion and occlusion of the left cervical and distal internal carotid artery. (D) Initial angiography showing occlusion of the left cervical internal carotid artery with a calcified atherosclerotic lesion (arrow). (E, F) The occluded lesion was crossed, and PTA was performed. (G) Angiography showing residual occlusion of the left distal internal carotid artery. (H) MT was performed with the combined use of a stent retriever and an aspiration catheter. (I) Postprocedural angiography showing complete recanalization. (J) Final angiography showing residual stenosis (arrow). (K, L) MRI on the day after the procedure showing recanalization of the middle cerebral artery but reocclusion of the cervical internal carotid artery, without significant infarct extension. (M, N) Because of frequent transient ischemic attack, superficial temporal artery to middle cerebral artery bypass was performed 7 days after the initial procedure. (O, P) MRI on the day after the bypass procedure showing no significant infarct extension compared to that on initial imaging on admission, with successful revascularization. Abbreviations: MT, mechanical thrombectomy; MRI, magnetic resonance imaging; PTA, percutaneous angioplasty.
All patients with ACICAO were male, with a median age of 77 years. The median NIHSS score ASPECTS were 16 and 8, respectively, with intravenous tPA use in three patients (30%). In all 10 patients, the intracranial arteries, as well as the cervical carotid arteries were not visualized on preprocedural vascular imaging; six patients (60%) had defects peripheral to the distal ICA, and the remaining four patients (40%) had defects peripheral to middle cerebral artery M1 segment.
EVT Procedures
In one patient, the cervical lesion could not be crossed through successfully; however, in the remaining nine patients the lesion was crossed successfully. In all cases, the lesions were very hard and required PTA to allow passage of devices. Four patients underwent CAS acutely (Figures 2 and 3), while the other five underwent cervical PTA alone (Figures 4 and 5, Supplementary Movie 1). After MT for the remaining intracranial LVO, eight patients (80%) achieved successful recanalization (TICI 2b or 3). However, one patient developed massive SAH due to vessel injury during EVT and another patient developed massive ICH due to hyperperfusion syndrome within hours after EVT, both after stenting (Figure 3). Thus, symptomatic ICH occurred in these two patients (20%) who underwent emergent CAS, and both died within 24 hours. Three patients who received intravenous tPA had no any hemorrhagic complications after the treatment.
Staged Revascularization Procedure
Four of the five patients who initially underwent PTA alone subsequently underwent endarterectomy or stenting for residual stenosis within 3 weeks (Figure 4, Supplementary Movie 2). One patient underwent urgent CAS on the day after the initial EVT because a mobile plaque was found on neck ultrasound examination. The patient in whom the cervical lesion could not be crossed and one patient who developed reocclusion after EVT underwent a rescue bypass procedure due to persistent ischemic symptoms (Figure 5).
Outcome
After 90 days, four patients (40%) were functionally independent (mRS 0-2). This favorable outcome was achieved in one of the four patients (25%) who underwent urgent CAS and in three of the five patients (60%) who underwent PTA alone (Figure 6A). Both patients with mRS 6 died immediately after CAS. Regarding the concomitant intracranial occlusion site, the patients with distal ICA occlusion had a favorable outcome more frequently than those with middle cerebral artery occlusion (Figure 6B). The relationship between the time from onset and outcome is shown in Figure 6C and D. Although there were considerable differences in treatment in individual cases, there was a correlation between time and outcome. Relationship between outcome and treatment technique, occlusion site, and time from onset. (A) mRS at 90 days by EVT procedure. (B) mRS at 90 days by occlusion site. (C) The association between the time from onset to groin puncture and mRS at 90 days. The solid line indicates the regression line. (D) The association between the time from onset to recanalization and mRS at 90 days. In the two cases without recanalization, the time was represented as the time from onset to groin puncture. The solid line indicates the regression line. Abbreviations: mRS, modified Rankin Scale; EVT, endovascular treatment; CAS, carotid artery stenting; MT, mechanical thrombectomy; PTA, percutaneous transluminal angioplasty; ACICAO, atherosclerotic cervical internal carotid artery occlusion; MCAO, middle cerebral artery occlusion; DICAO, distal internal carotid artery occlusion.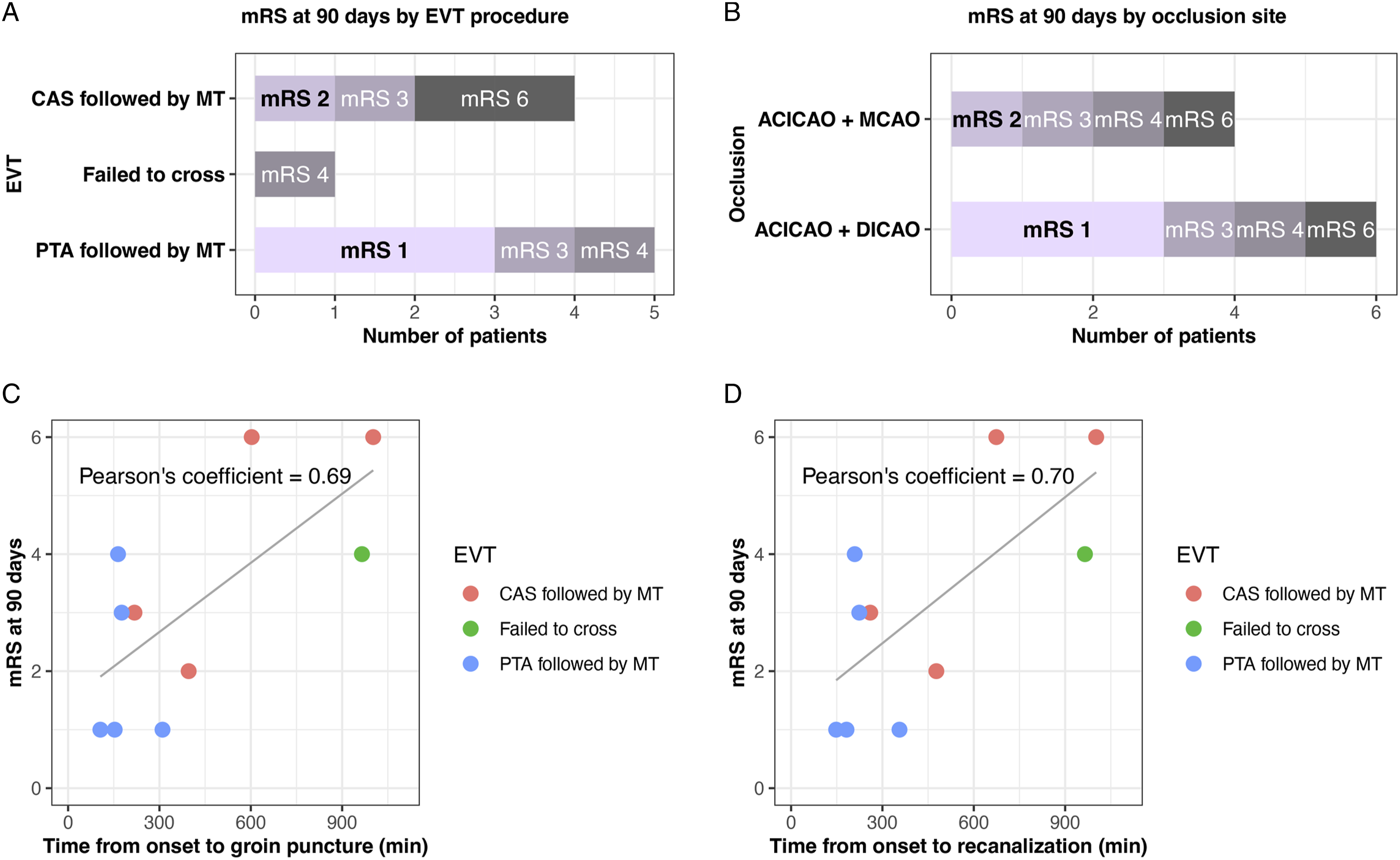
Discussion
In this study, we reported our experience in performing EVT for tandem ACICAO. EVT for ACICAO was technically feasible, although it was difficult to cross through the atherosclerotic plaque due to the lesion hardness. As a consequence, there were several characteristic complications, such as hyperperfusion syndrome and reocclusion. These features should be fully recognized for successful treatment when performing EVT for tandem occlusion. The PTA first-antegrade approach may reduce the risk of complications.
ACICAO as a Challenging Subgroup of Tandem Occlusion
Comparison of results with other studies.
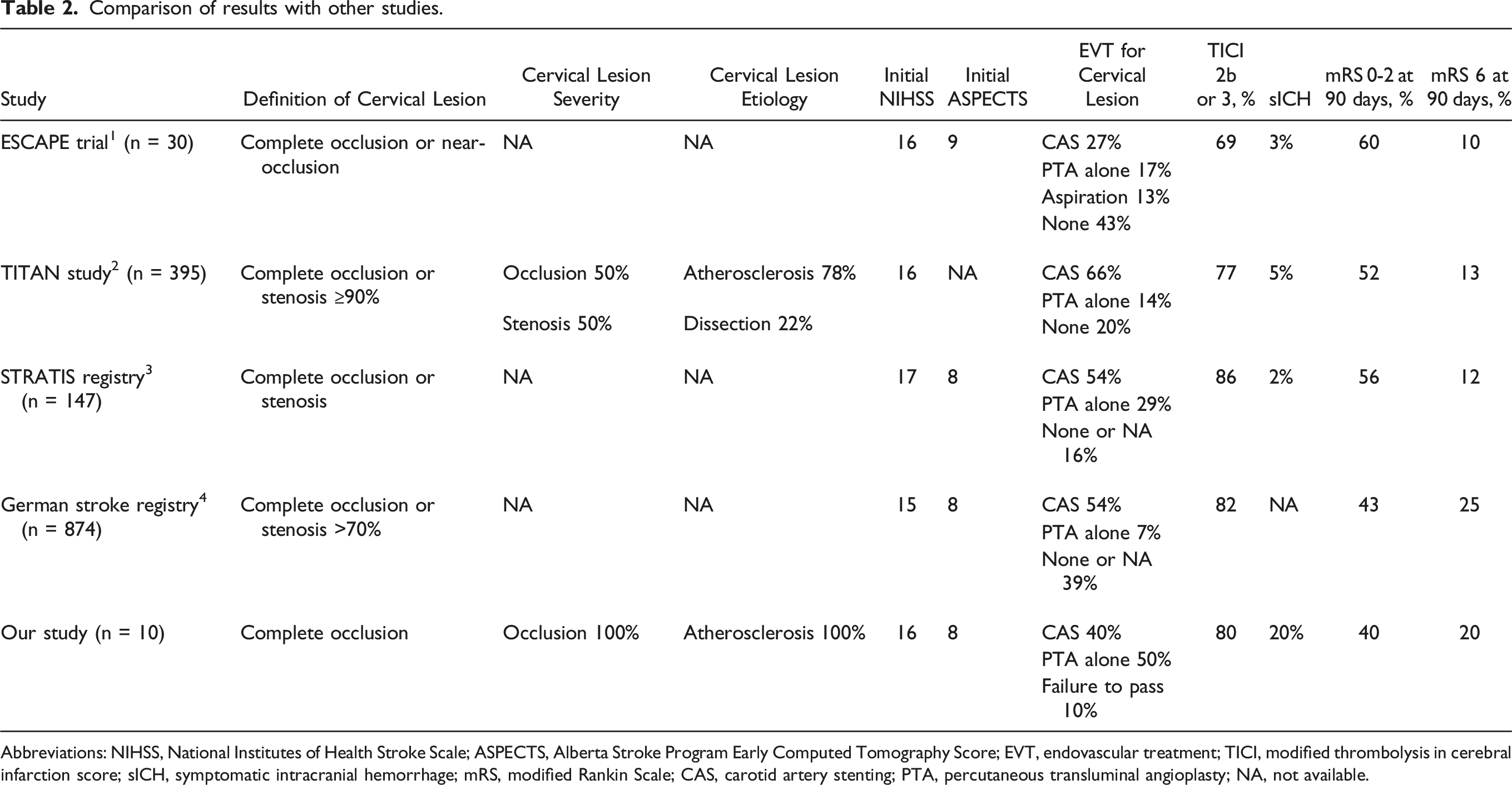
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; ASPECTS, Alberta Stroke Program Early Computed Tomography Score; EVT, endovascular treatment; TICI, modified thrombolysis in cerebral infarction score; sICH, symptomatic intracranial hemorrhage; mRS, modified Rankin Scale; CAS, carotid artery stenting; PTA, percutaneous transluminal angioplasty; NA, not available.
EVT Strategy for ACICAO
For tandem occlusions, there are two EVT approaches: the retrograde approach (direct MT), in which EVT of the intracranial lesion is performed first, and the antegrade approach (PTA first or CAS first), in which EVT of the cervical lesion is performed first. 8 Although the retrograde approach generally results in a shorter recanalization time, no difference in the rate of favorable outcomes between the two approaches has been reported in previous studies for tandem occlusions. 8 The ACICAO cases in our study were characterized by complete atherosclerotic occlusion of the cervical lesion, which requires more careful consideration of the treatment strategy.
The advantages and disadvantages of the EVT strategies for ACICAO are shown in Figure 1. The direct MT strategy involves the possible difficulty in crossing hard cervical lesions, the risk of distal embolization due to insufficient proximal flow control, and the risk of vascular injury due to blind manipulation.20,21 The CAS first strategy, which is reliable as a revascularization technique, has the problem of delayed recanalization and requires aggressive antiplatelet therapy.22,23 The PTA first strategy, which can be considered as a strategy that lies between the two aforementioned approaches, mitigates the advantages and disadvantages of both.24,25 Therefore, we selected the PTA first approach as our first choice strategy in the middle of our series because we experienced critical complications with the CAS-first approach.
EVT Results for ACICAO
EVT for tandem occlusion has unique complications that require attention, and in ACICAO, the possibility of these complications may be high. Our results showed that there is a correlation between the time from onset and outcome. However, treatment complications were found to have a significant impact on the outcome. In our series, 40% of patients had an mRS 0-2 at 3 months, while 20% of patients died immediately after the procedure. Hemorrhagic complications can lead to serious consequences, as seen in the fatal cases in our series. In the two patients who died immediately after CAS, the administration of dual antiplatelet agents may have contributed to the spread of intracranial hemorrhage. In addition, since ACICAO is considered to have a high degree of stenosis, the risk of reocclusion and hyperperfusion syndrome should be higher than non-complete occlusive tandem occlusions.
The PTA first strategy has the potential to reduce these hemorrhagic complications. One reason for this is that aggressive antiplatelet therapy is not immediately required. Another is that it allows for staged revascularization, which may reduce the risk of hyperperfusion syndrome. 26 However, there are risks such as reocclusion and mobile plaques, as we have seen in our series. 27 In order to deal with these complications, it is necessary to perform appropriate examination at the follow-up and determine the requirement for additional treatment. Recognizing the possibility of such complications may contribute to better management in clinical practice.
Differentiation From Other Conditions
One important point to note is that while it is relatively easy to differentiate ACICAO from dissection, it is often difficult to differentiate ACICAO from chronic carotid artery occlusion.28-30 EVT for chronic carotid artery occlusion is considered technically feasible; however, the risks are fairly high.31-33 In patients with mild symptoms, the possibility of chronic occlusion should be considered and the risks and benefits of intervention with EVT should be carefully assessed.
Study Limitations
This study was limited by the small sample size, retrospective nature, and modification of the EVT strategy during the study period. Further large-scale studies are needed to clarify the distinctiveness of ACICAO as a challenging subgroup of tandem occlusions and to determine the optimal treatment strategy.
Conclusions
Our experience suggests that EVT for ACICAO is technically feasible; however, it involves the potential risk of several significant complications. These features should be fully recognized for successful treatment. The PTA-first antegrade approach may reduce the risk of complications.
Supplemental Material
Supplemental Material
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japanese Society for the Promotion of Science Grants-in-Aid for Scientific Research (JSPS KAKENHI) [grant numbers JP20K17968, JP21KK0289]; and the Medical Research Fund of Hyogo Medical Association [grant number MRF-R-2-20].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.