
Abstract
Background
Transcatheter embolization is a commonly used minimally invasive technique in the treatment of pulmonary arteriovenous malformation (PAVM) with a high probability of post-operative recurrence, and some recurrent cases of PAVM cannot be treated via pulmonary arterial re-embolization. Here, we report the first case, to our knowledge, a 55-year-old female undergoing percutaneous direct puncture embolization for recurrent PAVM with good short-term efficacy.
Case Presentation
The patient was a 55-year-old female presenting to the emergency department of our hospital with acute exacerbation of chest tightness and shortness of breath for 2 hours. The patient was diagnosed with PAVM and undergone embolization half a year ago. DSA-guided embolization was performed through percutaneous puncture approach. After embolization with four spring coils, the blood flow to the PAVMs was stopped and the surgery completed. The patient reported improvement of chest tightness and shortness of breath and was discharged from the hospital 3 days later.
Conclusion
Our case was unique as a portion of the PAVMs was closely attached to the chest wall and PVP was slightly increased, which made percutaneous puncture embolization possible. Our case can be helpful in the treatment of recurrent PAVM in patients who cannot undergo re-embolization through pulmonary artery.
Keywords
Introduction
As a rare lung condition with an incidence of around 3/10 000, pulmonary arteriovenous malformation (PAVM) is most commonly seen in adult women, and most cases are congenital. 1 Abnormal communications between pulmonary arteries and veins in patients with PAVM create right-to-left shunting, resulting in clinical manifestations associated with hypoxemia or ectopic embolism. 2 Transcatheter embolization is widely adopted as an effective treatment for PAVM, 3 but in some cases, PAVM recurrence after intervention cannot be treated via pulmonary arterial re-embolization. 4 Here, we report one such case that was successfully treated with re-embolization via a direct percutaneous puncture.
Case Presentation
The patient was a 55-year-old female presenting to the emergency department of our hospital with acute exacerbation of chest tightness and shortness of breath for 2 hours. She experienced sudden chest tightness and shortness of breath while sleeping and reported that her symptoms were slightly relieved by moving into a semi-recumbent position. Seven years prior, the patient had started to develop post-activity chest tightness and shortness of breath, which had progressively worsened. Four years before her presentation, the patient had been admitted into another hospital due to exacerbation of chest tightness and shortness of breath. Being diagnosed with “pulmonary arteriovenous fistula”, she had started to undergo domiciliary oxygen therapy. Three years prior, she had begun to receive continuous oxygen therapy for 24 hours/day with occasional out-of-bed activities, and significant chest tightness and shortness of breath had continued to appear on mild exertion. Half a year before her presentation to our hospital, she had undergone PAVM embolization.
The patient had undergone four pregnancies and given birth to four children via spontaneous labor. She reported having had repeated nosebleeds since childhood but no other previous medical history; the patient’s mother, however, was once diagnosed with PAVM.
The patient’s respiratory rate increased significantly upon arrival at the emergency department, reaching 27 times/min. Other measurements were as follows: blood pressure: 158/89 mmhg, heart rate: 91 times/min, body temperature: 36.2°C. The patient had cyanosis in the lips. Diastolic murmur was audible in the left upper pulmonary area in proximity to the sternum and pronounced during the inspiratory phase.
Arterial blood gas analysis on the day of hospital admission: delivered oxygen concentration (FiO2) 33.0%, partial pressure of oxygen (PaO2) 77.1 mmHg, partial pressure of carbon dioxide (PaCO2) 34.6 mmHg, oxygenation index (P/F): 233.64; hemoglobin (Hb): 155 g/L.
A computed tomography pulmonary angiogram (CTPA) on admission revealed tortuous and dilated blood vessels in the left upper lobe anterior segment of the lung originating from the left pulmonary artery (Figure 1A). Spring coils used in the previous embolization were seen at the site of origin and vascular malformations drained into the left pulmonary vein; a portion of the malformed vascular clusters in PAVM was exposed under the chest wall (Figure 1B). Similarly, digital subtraction angiography (DSA) showed vascular malformations in the left upper lobe of the lung originating from the location of the spring coils used in the previous embolization. The contrast agent passed through the malformed vascular clusters smoothly (Figure 1C). Simultaneously, systolic pulmonary artery pressure (sPAP, 42 mmHg) and wedge pressure (PWP, 15 mmHg) were measured with a Swan–Ganz catheter. Patient images before and after initial treatment, before surgery in our hospital, during intervention surgery, and at post-operative follow-up visit (A): The patient provided CTPA images obtained before her first PAVM embolization (oblique sagittal MIP reconstruction) revealing the arterial end (white arrow), the venous end (black arrow) and fistula (asterisk) of PAVM in the left upper lobe of the lung. (B and C): CTPA (oblique sagittal MIP reconstruction) and pulmonary arterial angiogram performed for the patient at our hospital revealed PAVM in the left upper lobe of the lung, malformed blood vessels filled with contrast agents, and the originally implanted spring coils in place (white arrow). (D): CT-guided percutaneous PAVM puncture with a fine needle and delivery of a microguide wire to the PAVM feeding arteries. (E): Angiogram of the percutaneous puncture approach. (F): Angiography through the vascular sheath shows blood retention in PAVM after embolization with 3 coils. (G): Follow-up examination at 6 months after surgery suggested the absence of contrast agents in PAVM and complete occlusion of the PAVM.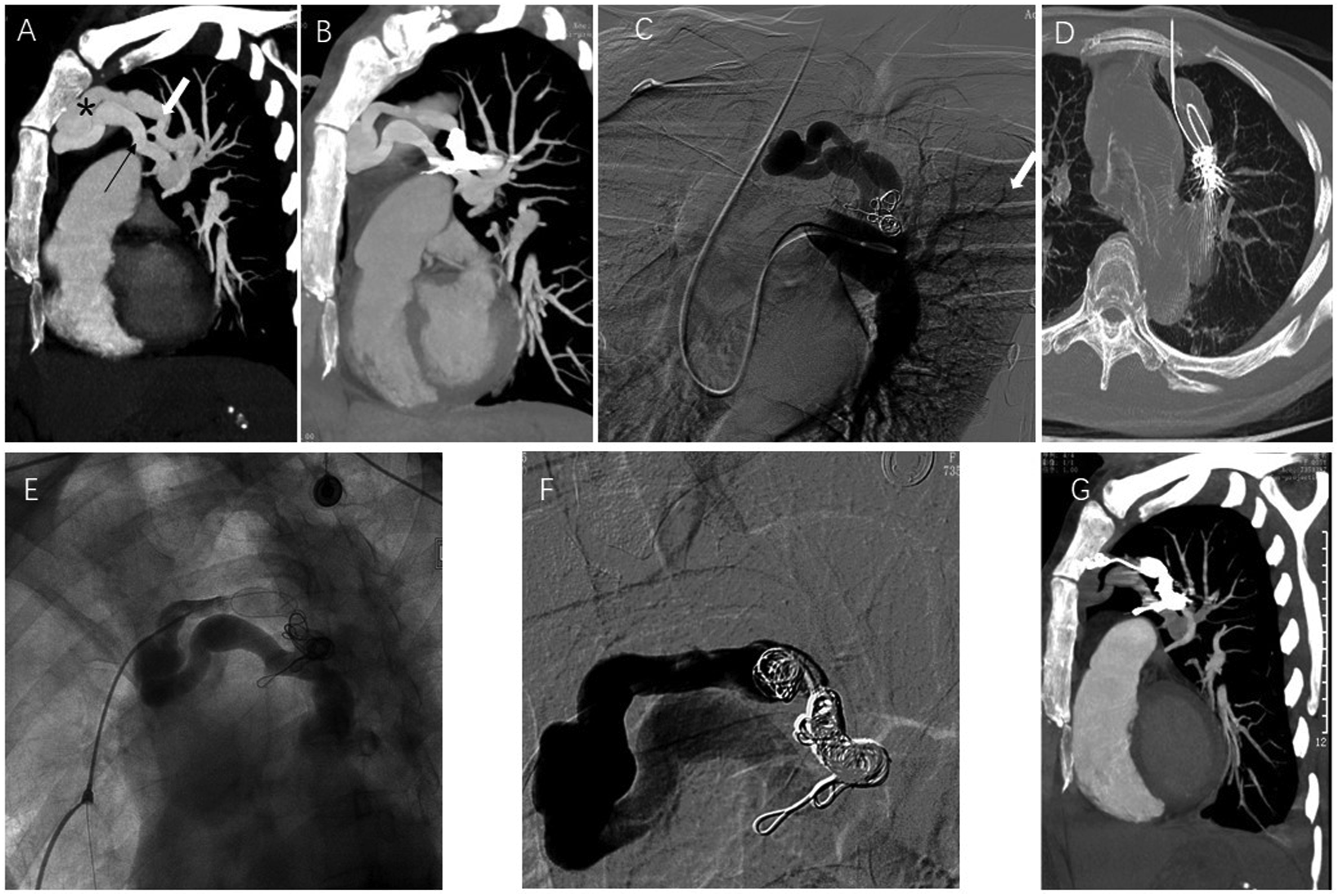
The patient was diagnosed with PAVM and concurrently diagnosed with hereditary hemorrhagic telangiectasia (HHT) based on her past medical history and family history.
DSA-guided embolization was performed. Due to blockade by the previously used spring coils, re-intubation of the PAVM feeding arteries via pulmonary arteries failed. Given that a portion of the patient’s malformed vascular clusters was exposed under the chest wall, we punctured the malformed vascular clusters with a fine needle under CT guidance (Figure 1D) and inserted a 4F vascular access sheath. The spring coils were subsequently implanted through the sheath under DSA guidance for embolization (Figures 1E and 1F). After embolization with four spring coils (InterlockTM Fibered IDCTM Occlusion System, Bosten Scientific, USA), the blood flow to the PAVMs was stopped and the surgery completed. In order to avoid coils migration, we selected interlocking detachable coils with a diameter of 12 mm (slightly larger than the diameter of the target vessel by 10 mm) for embolization. The later-placed spring coil was closely bound with the previously-placed spring coil. When the spring coil was nearly released, the coil was observed whether it was vibrating with blood flow, and then completely released after confirming that the coil was stable.
The patient reported improvement of chest tightness and shortness of breath during the operation and was discharged from the hospital 3 days later. Follow-up examination at 6 months after surgery suggested complete occlusion due to the absence of contrast agents in the PAVMs (Figure 1G). At 6 months after surgery, the patient no longer required domiciliary oxygen therapy, and was able to walk freely and engage in light physical labor.
Discussion and Conclusion
PAVM is most commonly seen in adult women and most cases are congenital. 1 Most congenital cases of PAVM are associated with HHT. 5 Although intervention therapies were considered in the past when the PAVMs had a feeding artery diameter >3 mm or were accompanied by corresponding symptoms, many researchers now believe that any PAVM visible on enhanced CT should be treated.6-8 Enhanced CT is considered the preferred imaging modality for diagnosing PAVM, and a pulmonary arterial angiogram can clearly show the structure of PAVM for further embolization. Transcatheter embolization is widely adopted as an effective treatment for PAVM and is considered the preferred choice of treatment due to the relatively minor damage it inflicts. 9 Surgical treatment is considered only when hospitals are not capable of performing embolization in emergency settings. 3
The treatment of recurrent PAVM is more challenging than initial treatment for PAVM. It has been reported that up to 25% of PAVMs relapse after initial embolization and only less than half of these recurrent PAVM cases are successfully treated with embolization resulting in complete occlusion.4,10 PAVM recurrence following intervention therapies mostly manifests in reperfusion of the embolized blood vessels associated with factors such as an excessively small or improper size of the spring coils for embolization or an overly proximal coil placement from the arteriovenous connection. 4 Re-embolization can only be performed for recurrent PAVM if (1) a microcatheter can be advanced through the original spring coils until the distal end or (2) the space proximal to the original spring coils is large enough to permit implantation of additional embolic materials. The case reported herein did not satisfy the above conditions, and hence could not be treated via routine pulmonary arterial re-embolization.
After careful analysis of the patient’s CT images, we found that a portion of the PAVMs was exposed under the chest wall and puncture of this exposed portion could be considered to allow access into the malformed blood vessels without the risk of pulmonary hemorrhage. Meanwhile, sPVP and PWP of the patient were slightly increased, which meant the blood pressure in PAVMs was not high enough to cause severe hemothorax in interventional operation. Taking these into account, we decided to puncture the PAVMs percutaneously. Furthermore, the operation room and thoracic surgeons were ready when we started the punction in case unexpected bleeding happened. After direct puncture and embolization of the PAVM, we achieved complete occlusion of the PAVM and good short-term efficacy. Further observation and evaluation of the long-term efficacy of the procedure are, without doubt, required.
Transseptal and pulmonary venous approach is another way to access the pulmonary malformed blood vessels. 11 However, complications including pericardial effusion, iatrogenic cardiac injury may occur during the operation.12,13 This approach should be considered by a multidisciplinary team. If cardiologists skilled at transseptal puncture are available, transseptal and pulmonary venous approach offers an alternative way for PAVMs closure.
The uniqueness of this case lies in the fact that a portion of the PAVMs was closely attached to the chest wall and PVP was slightly increased, which made percutaneous puncture embolization possible. However, further validation is required in order to confirm whether this approach leads to severe intrapulmonary hemorrhage or hemothorax when applied in the treatment of other intrapulmonary lesions with or without high PVP. Our attempt at treating this case can offer new directions for the treatment of recurrent PAVM in patients who cannot undergo re-embolization through pulmonary artery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
Informed consent has been obtained from the patient for publication of the case report and accompanying images.