
Abstract
Purpose: Here, we report our experience treating a patient with Maffucci syndrome and evaluate the outcomes resulting from surgical management combined with sclerotherapy in the treatment of head and neck venous malformations (VMs). A 19-years-old woman with multiple enchondromas and heterauxesis complained of masses in the oral cavity that had gradually increased in size and eventually affected her daily life. A tracheotomy was performed followed by traditional sclerotherapy to treat the oropharyngeal VMs. Next, we surgically excised the VMs of the oral cavity and maxillofacial skin. Results: Magnetic resonance imaging indicated that the oral VMs were nearly eradicated and the oropharyngeal VMs had stabilized. The patient’s appearance and normal maxillofacial region function were restored. Conclusion: In summary, local resection combined with sclerotherapy facilitated timely and efficient VMs removal from the head and neck region of a patient with Maffucci syndrome.
Introduction
Maffucci syndrome is a rare syndrome involving vascular anomalies. The main clinical manifestations are venous malformations (VMs), multiple enchondromas, and spindle cell hemangioma. 1 Currently, somatic mutation of the isocitrate dehydrogenase 1/2 (IDH1/2) gene is widely regarded as the pathogenesis of Maffucci syndrome. 2
Cutaneous and subcutaneous lesions are common in venous disorders such as Maffucci syndrome. These lesions have a sporadic nature, and VMs can occur in the mucosa of the oral and maxillofacial region. Although sclerotherapy using several types of media, such as polidocanol and ethanol, has obtained promising results for common types of VMs,3,4 few studies have been conducted on the endovascular treatment of VMs in patients with Maffucci syndrome specifically. However, multiple reports have been published regarding sclerotherapy treatment for VMs similar to those associated with Maffucci syndrome. 5
We admitted and treated a patient with Maffucci syndrome with multiple and extensive VMs in the oral cavity and oropharynx. Local resection was performed to improve the patient’s oral function, and traditional sclerotherapy was conducted simultaneously to treat the region that was difficult to approach surgically. The patient was followed up for 1.5 months, and we assessed the outcomes resulting from this combination treatment strategy for VMs in the head and neck region.
Case Description
Patient
A 19-year-old woman whose main complaint was that her right leg became shorter than her left leg at the age of 4 presented to our hospital. The patient underwent a mass biopsy of the right thigh at a local hospital, which indicated multiple enchondromas. In addition to multiple masses in the extremities, bluish violet nodules could be observed in the oral and maxillofacial region on physical examination. Furthermore, this patient had severe heterauxesis (Figure 1A). Plain film of the Maffucci patient. (A) Full-body picture. (B) X-ray image of the right shoulder and thorax. (C) X-ray image of the right elbow. (D) X-ray image of the right wrist. (E) X-ray image of the right hip joint. (F) X-ray image of the right knee. (G) X-ray image of the right ankle. Arrows: multiple enchondromas.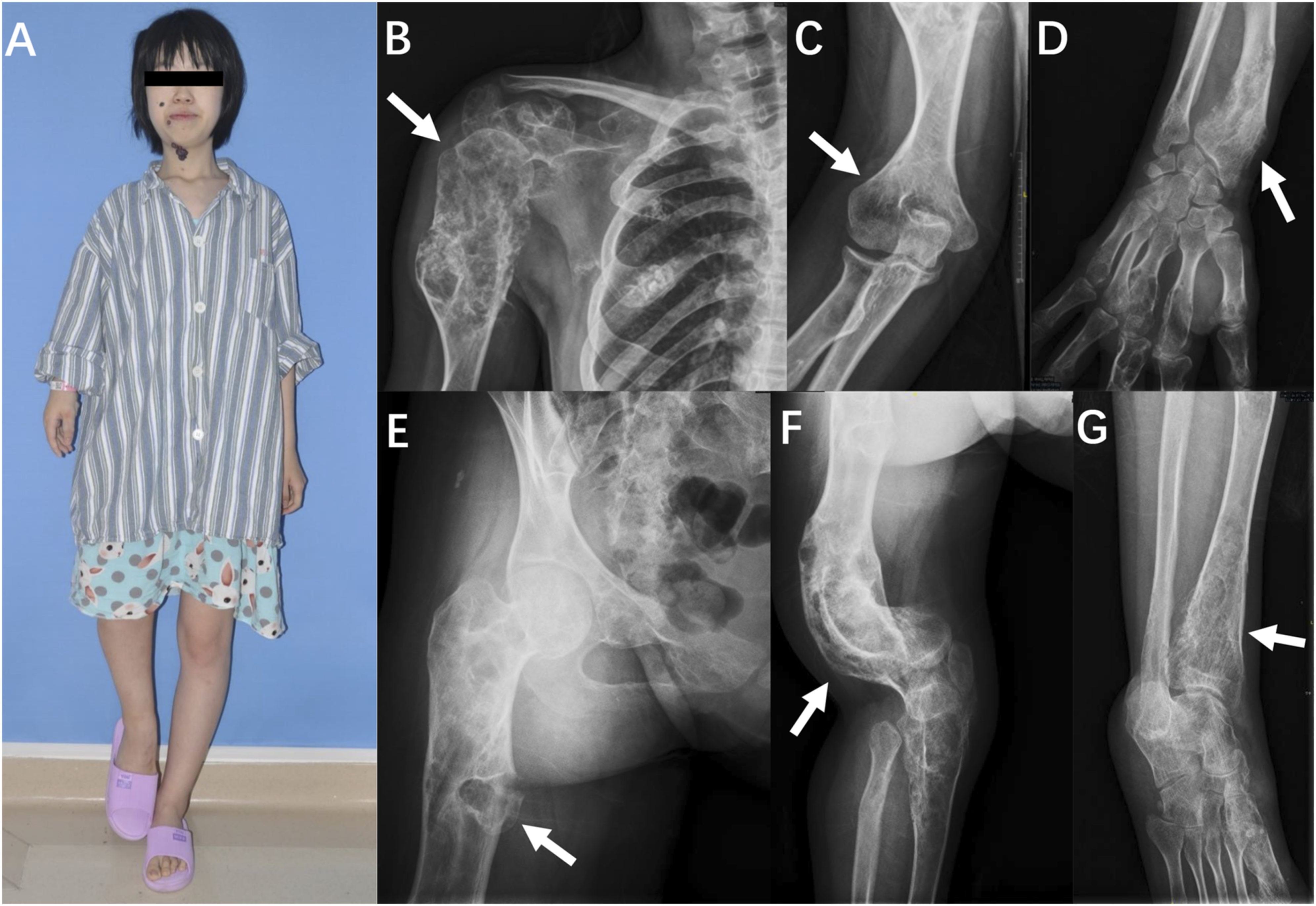
Because of the gradual enlargement of the intraoral masses, the patient’s mastication and deglutition functions were seriously impaired, accompanied by occasional ulceration and hemorrhage of the oral lesions (Figure 2A). This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the Ninth People’s Hospital at the Shanghai Jiao Tong University School of Medicine (approval number: SH9H-2019-T309-2). Informed consent was obtained from the patient for inclusion this study and for publication of this case report and the accompanying images. Pre-operation pictures of the Maffucci patient. (A) VMs of the oral and maxillofacial region. (B) MRI image of oral level (arrow: oral venous malformation). (C) MRI image of submandibular level (arrow: oropharyngeal venous malformation).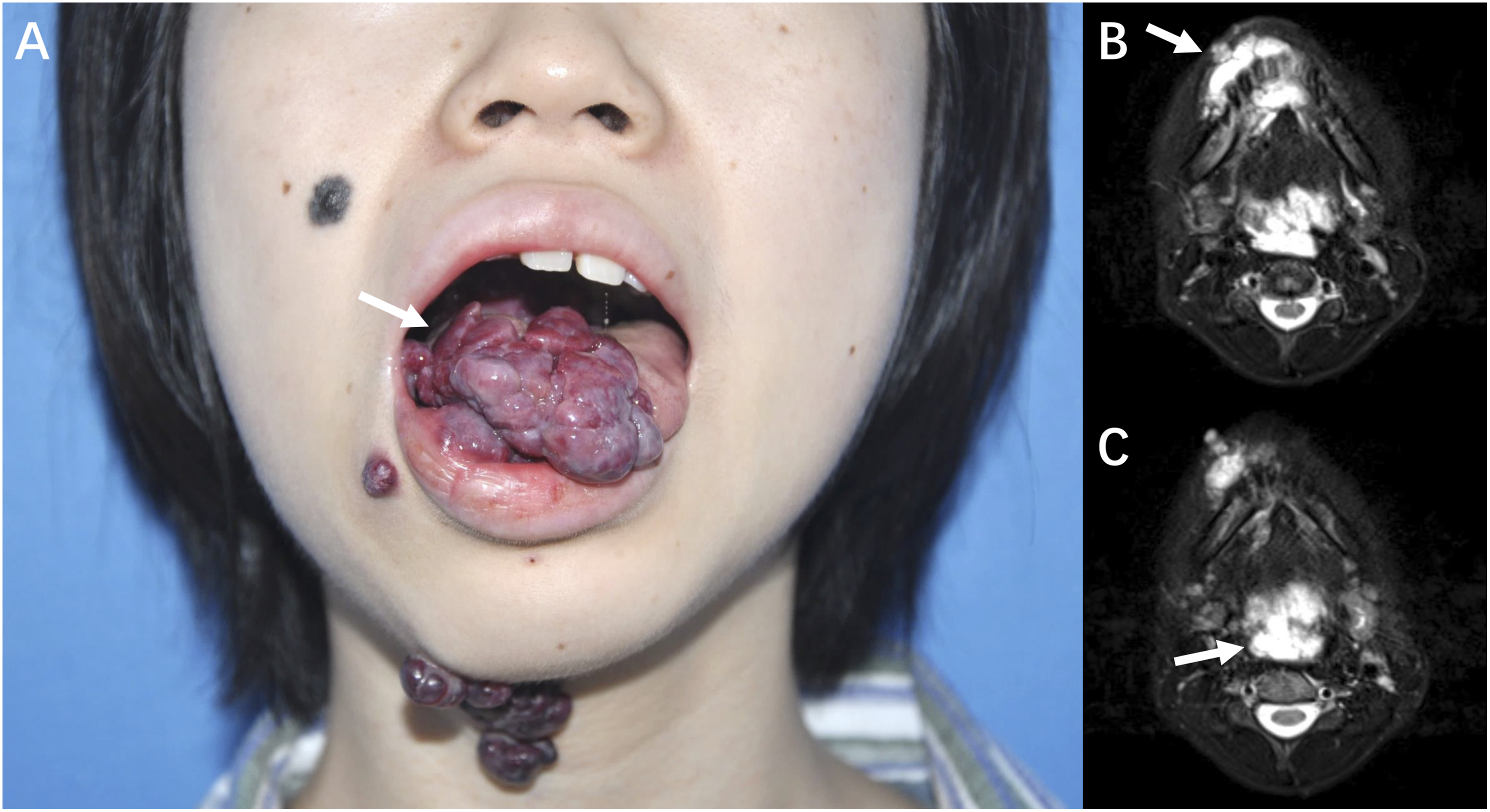
Clinical Examinations
Plain film x-ray revealed multiple enchondromas in the patient’s right shoulder and thorax (Figure 1B) and elbow (Figure 1C), wrist (Figure 1D), hip (Figure 1E), knee (Figure 1F), and ankle joints (Figure 1G), along with underdevelopment in all affected long bones.
Magnetic resonance imaging (MRI) showed multiple prolonged T2-weighted signals in the oral and maxillofacial region, indicating extensive VMs (Figures 2B and 2C, Video 1).
Hematological test results indicated normal coagulation function as follows: platelet count, 180 × 109/L (reference: [100-300] × 109/L); fibrinogen level, 2.08 g/L (reference: 2-4 g/L); D-dimer level, .24 mg/L (reference: < .5 mg/L); prothrombin time, 11.9 seconds (reference: 11-14 seconds); activated partial thromboplastin time, 32.2 seconds (reference: 25-37 seconds); international normalized ratio, 1.10 (reference: .8-1.2); and thrombin time, 15.9 seconds (reference: 14-21) seconds).
Therapeutic Procedures
Tracheotomy and anesthesia
The patient was positioned with the neck moderately extended. A tracheotomy was performed with a tracheotomy tube (Covidien, Chihuahua, Mexico) under local anesthesia after performing awake intubation with an inner cannula. Blood pressure, electrocardiogram, oxygen saturation, and end-tidal carbon dioxide levels were continuously monitored. General anesthesia was induced after successful tracheotomy.
Sclerotherapy
Lesions located in the oropharynx region were first punctured with an 18-gauge needle (Cook Medical, Inc, Bloomington, IN, USA). Once venous blood was observed, Ultravist® (Bayer AG, Leverkusen, Germany) was injected to perform dynamic venography based on digital subtraction angiography (DSA). The location of the needle tip and lesion extent were detected. As VMs have limited blood flow, the contrast usually stagnates within the VMs lesion. Subsequently, ethanol was injected into the VMs under the guidance of DSA. The total amount of ethanol was less than 1 mL/kg of body weight. 3
Surgical management
Subsequently, we performed surgical resections for the mucosal VMs in the oral cavity and perioral region aiming to promptly remove the obstruction and restore oral function. The cutaneous lesions of the right corner of the mouth and submandibular region were excised by fusiform incision and sutured with 6-0 Vicryl® sutures (Johnson and Johnson, New Brunswick, NJ, USA). The mucosal lesions of the tongue, lower lip, and soft palate were incised around the base of the lesion, and an adjacent tissue flap was transferred to repair the soft tissue defects in the oral cavity. Finally, absorbable sutures were used for wound closure.
Clinical Outcomes
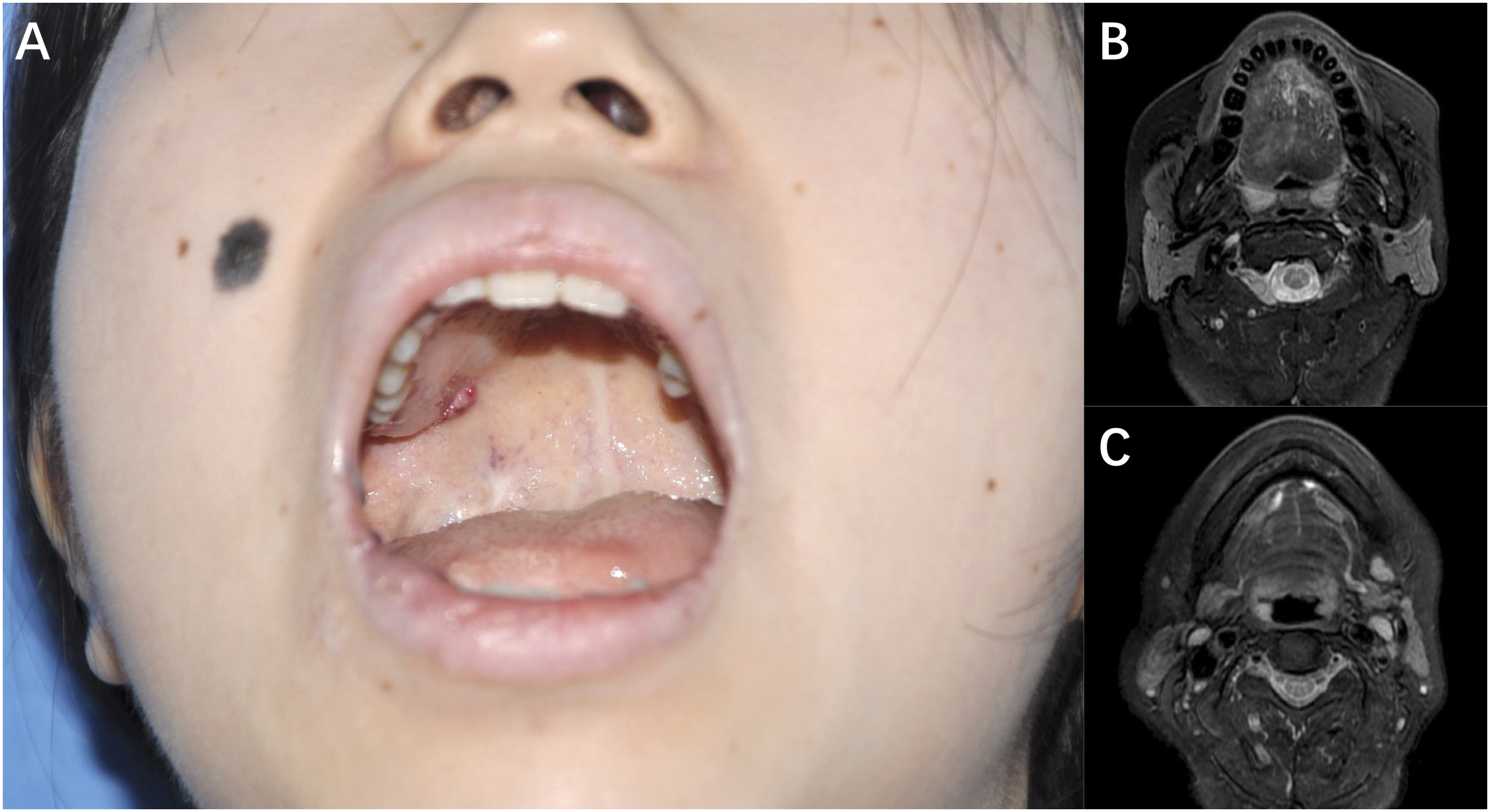
Pathological examinations indicated the venous nature of the oral and maxillofacial masses. The patient underwent a follow-up examination 1.5 months later. As Figure 3A shows, the oral VMs were nearly eliminated. No prolonged T2-weighted signals were observed in the oral cavity and neck (Figures 3B and 3C, Video 2). Residual venous lesions still existed in the oropharyngeal region; however, the overall size of the VMs was reduced (Figures 2C and 3C). During the follow-up period, the patient regained lingual shape and functions. Moreover, the patient’s appearance was restored. In the most recent follow-up (1 year after surgery), no recrudescence of VMs was observed in the patient’s oral cavity (Figure 4A). Meanwhile, Figures 4B and 4C show that sclerotherapy eliminated the primary VMs lesion in the oropharynx (Video 3). Post-operation pictures of the Maffucci patient (1 and half months after therapy). (A) Post-operation image of the oral and maxillofacial region. (B) Post-operation MRI image of oral level. (C) Post-operation MRI image of submandibular level. Arrows: residual venous lesions of oropharynx. One-year follow-up pictures of the Maffucci patient. (A) The local image of the patient’s oral cavity. (B) MRI image of oral level. (C) MRI image of submandibular level.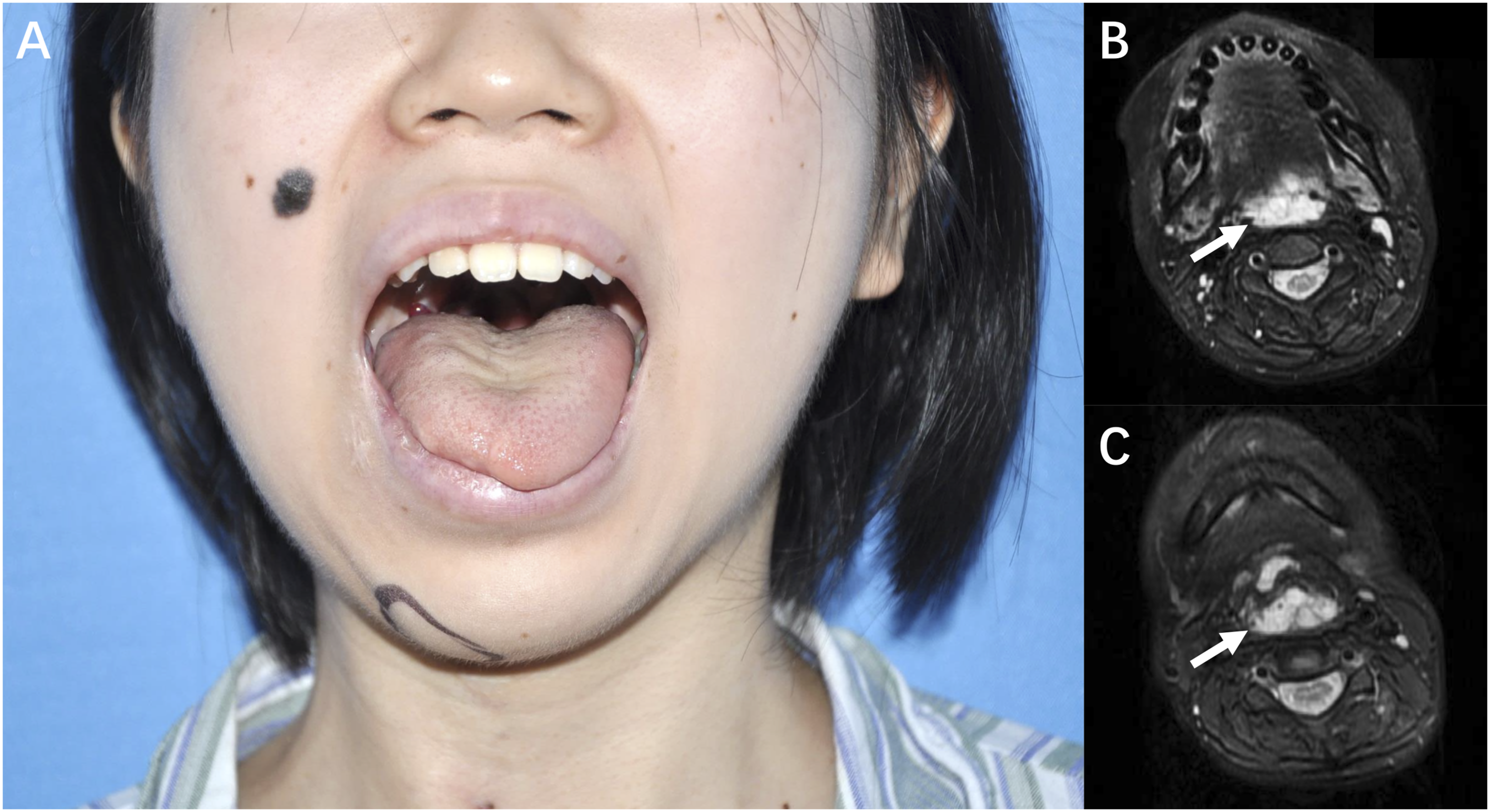
Discussion
Distinguishing Maffucci syndrome from Ollier disease (OD) should be the first priority in its differential diagnosis. Whether Maffucci syndrome and OD are mutually independent diseases is unclear, and patients with OD also develop multiple enchondromas, although without evidence of VMs. 6 Unlike the soft and compressible nature of standard VMs, these lesions typically present with hard and nodular masses on the skin or mucosa in patients with Maffucci syndrome. The morphological abnormalities of veins give rise to blood flow stasis and thrombosis, thereby increasing the possibility of calcification; phlebolith is commonly observed in VMs lesions. 7 Extensive or multiple VMs always give rise to lesion hypercoagulability, also known as local intravascular coagulation. 8 Therefore, assessing and treating abnormal coagulation function in patients with VMs is the top priority. In our center, heparin is traditionally administered to improve coagulation function in patients with VMs with low fibrin levels (below 1.0 g/L) before treatment. Here, no coagulation dysfunction was observed in our patient with Maffucci syndrome, although the patient had multiple VMs.
Theoretically, sclerotherapy is less invasive than surgery; however, it cannot promptly eradicate lesions as with surgical treatments. Localized VMs usually require repeated treatments to reach stability and further atrophy, and even more treatments are required for extensive types. Considering that the tongue plays a pivotal role in mastication and deglutition in the oral and maxillofacial region, local resection was performed in the present case instead of sclerotherapy to treat the mucosal VMs in the oral cavity, which led the patient to regain oral functions and promptly eliminated the VMs. In contrast, traditional sclerotherapy was implemented for the oropharyngeal VMs, as it was difficult to approach surgically.
Akan et al 9 performed percutaneous sclerotherapy and ligation to manage multiple oral and oropharyngeal VMs in a patient with Maffucci syndrome while Nassiri et al 10 performed staged sclerotherapy and surgical treatment for vulvar VMs in a patient with Maffucci syndrome. These findings also provided us with references regarding the use of surgery combined with sclerotherapy to compensate for the disadvantages of sclerotherapy alone. Nevertheless, regardless of treatment type, a prophylactic tracheostomy was required to prevent oropharyngeal swelling and pharyngeal tissue-induced asphyxia.
Enchondroma, which is prone to occur in the metaphysis or epiphysis of the phalanges, can cause hypoplasia of the affected side and present with the “frosted glass” sign on X-ray examinations (Figure 1). Enchondroma has the potential for malignant transformation, thereby increasing the probability of malignant tumors in patients with Maffucci syndrome. 11 Christopher et al 12 reported on a patient with Maffucci syndrome with enchondroma-induced myelopathy that was treated with surgical management. Furthermore, the previous case involving surgery for OD may provide a reference for treating patients with Maffucci syndrome. Klein et al 13 reported that early surgical treatment comprising curettage leads to sound clinical, cosmetic, and radiological outcomes. Early surgical treatment of well-developed or symptomatic enchondromas in patients with OD should be considered. In the treatment of patients with Maffucci syndrome, given that surgical treatments come at the expense of anatomical structure damage, the indications for surgery in patients with enchondroma should be: 1) evidence that the enchondroma has undergone malignant transformation, 2) enchondroma has affected the patient’s function, and 3) curettage is a priority over amputation.
Conclusions
In the VMs in head and neck region of a patient with Maffucci syndrome, surgical treatment combined with ethanol-based sclerotherapy efficiently removed the lesion and promptly restored the patient’s oral function.
Supplemental Material
Supplemental Material
Supplemental Material
Footnotes
Acknowledgments
We appreciate all the medical workers from the Department of Interventional Therapy, Shanghai Ninth People’s Hospital, for their active cooperation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No.81871458), the Clinical Research Program of Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (No. JYLJ202111), and the Transverse Research Project of Shanghai Ninth People’s Hospital (No. JYHX2022007).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.