
Abstract
Introduction
Component separation (CS) of the Zenith Dissection Endovascular Graft and Stent have been reported with some causes. However, CS caused by aortic elongation has not yet been reported. A long treatment range with the sacrifice of some intercostal arteries (ICAs) is sometimes needed when repairing CS because of the large difference in the diameter between the proximal and distal landing zones with a reverse taper.
Case presentation
A 78-year-old man, who underwent thoracic endovascular aortic repair (TEVAR) using a Zenith Dissection Graft and stents for acute type B aortic dissection 3 years and 8 months previously was admitted to our hospital with severe back pain. Contrast-enhanced computed tomography (CT) showed separation of the SG and bare stent, and aortic elongation. As there was a large difference in the diameter of the proximal and distal landing zones with a reverse taper, a long treatment range with the sacrifice of two large ICAs was needed. Thus, TEVAR using an inverted thoracic SG technique was performed in order to shorten the treatment range to preserve a large ICA and reduce the risk of paraplegia. Completion angiography showed that the separation was repaired with preservation of the large ICA. The postoperative course was uneventful, and he was discharged on postoperative day 10 with relief of his severe pain. At 1 year after secondary TEVAR, CT showed that the diameter of the descending aorta had decreased with no separation of the SGs.
Conclusion
Deployment of an inverted thoracic SG for the treatment of CS of the Zenith Dissection Endovascular Graft and Stent is a feasible and effective procedure to preserve ICAs. An overlapping range of >1.5 times the length of a bare stent within an SG is needed to prevent CS of the Zenith Dissection Endovascular Graft and Stent caused by aortic elongation.
Introduction
The Zenith Dissection Endovascular System, which consists of a covered stent (Zenith TX2 Dissection Endovascular Graft with Pro-Form [Cook Medical, Bloomington, IN, USA]) and a bare metal stent (Zenith Dissection Endovascular Stent [Cook Medical]) has sometimes been used for the treatment of type B aortic dissection. Cases involving component separation (CS) or migration of the covered or bare stent have been reported.1,2 However, CS caused by aortic elongation have not been reported. A long treatment range with the sacrifice of some intercostal arteries is often needed when repairing component separation because of the large difference in the diameter between the proximal and distal landing zones with a reverse taper. We repaired the component separation caused by aortic elongation using a new inverted thoracic stent graft technique in order to shorten the treatment range with preservation of the intercostal arteries to reduce the risk of paraplegia.
Case Report
A 78-year-old man, who underwent TEVAR with a Zenith Dissection Endovascular Graft with Pro-Form (ZTEG-2PT-34-24-199-PF, Cook Medical) and Zenith Dissection Endovascular Stents (GZSD-36-123-2, GZSD-36-164-2, Cook Medical) for acute type B aortic dissection 3 years and 8 months previously was admitted to our hospital with severe back pain. Contrast-enhanced computed tomography (CT) on day 7 after thoracic endovascular aortic repair (TEVAR) showed that only one-fourth of the bare stent overlapped within the stent graft (Figure 1A). Contrast-enhanced CT 3 years and 8 months after TEVAR showed CS between the stent graft and bare stent (Figure 1B). Remodeling of the descending aorta was observed after TEVAR. After that, type 1b endoleak and enlargement of the descending aorta were observed. There was no distal stent graft-induced new entry; however, separation of the stent graft and bare stent was observed. As we considered that the severe back pain was induced by extension of the descending aorta caused by type 1b endoleak, we decided to treat the type 1b endoleak caused by CS of the covered stent and bare stent. An inverted thoracic stent graft technique was planned to preserve the intercostal arteries (ICAs) as much as possible to prevent paraplegia. A: Contrast-enhanced computed tomography 7 days after initial TEVAR shows that only one-fourth of the first bare stent overlapped within the stent graft (arrow). B: Contrast-enhanced computed tomography shows enhancement outside of the stent graft in the descending aorta, with separation of the stent graft and bare stent (arrow).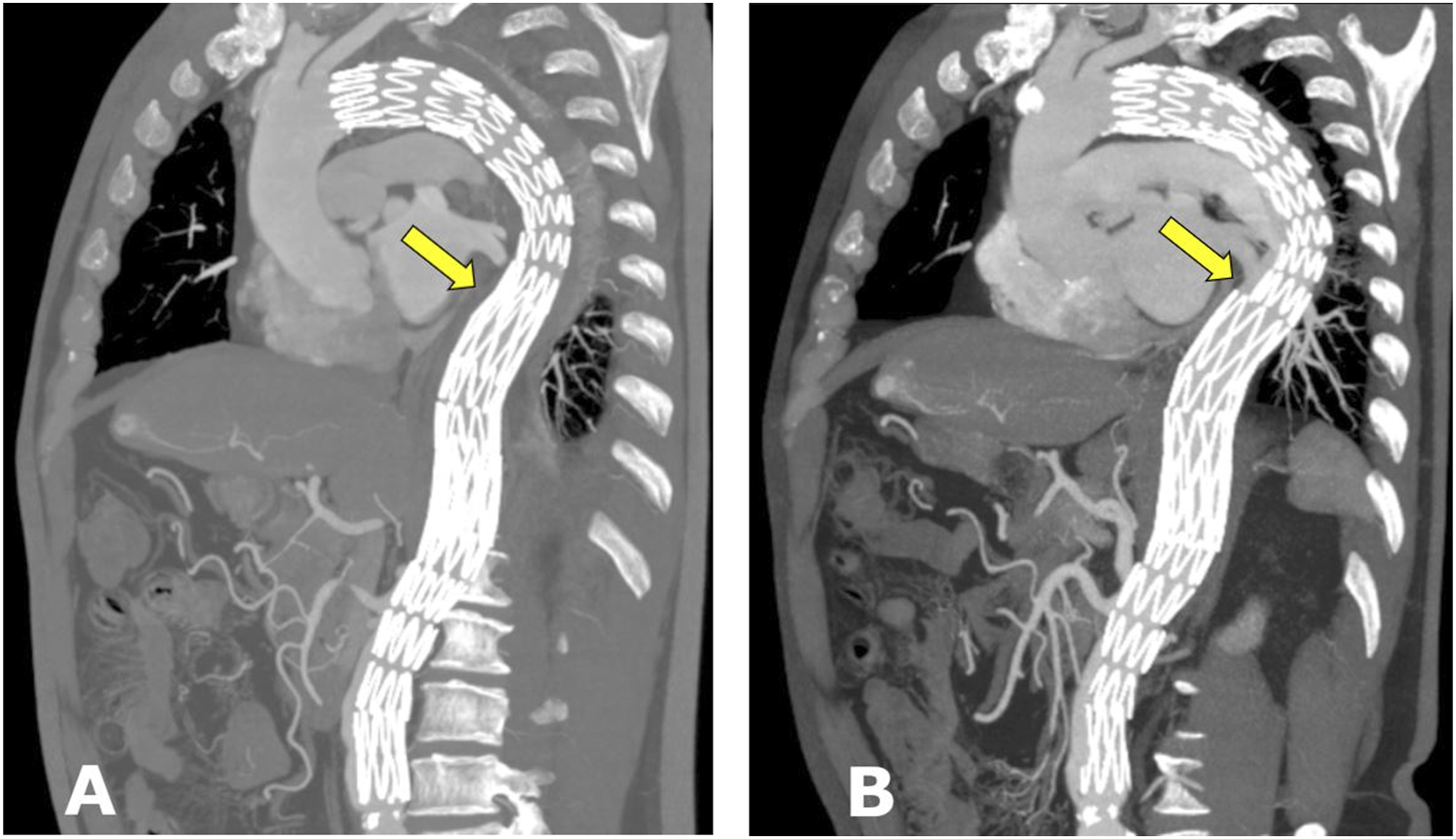
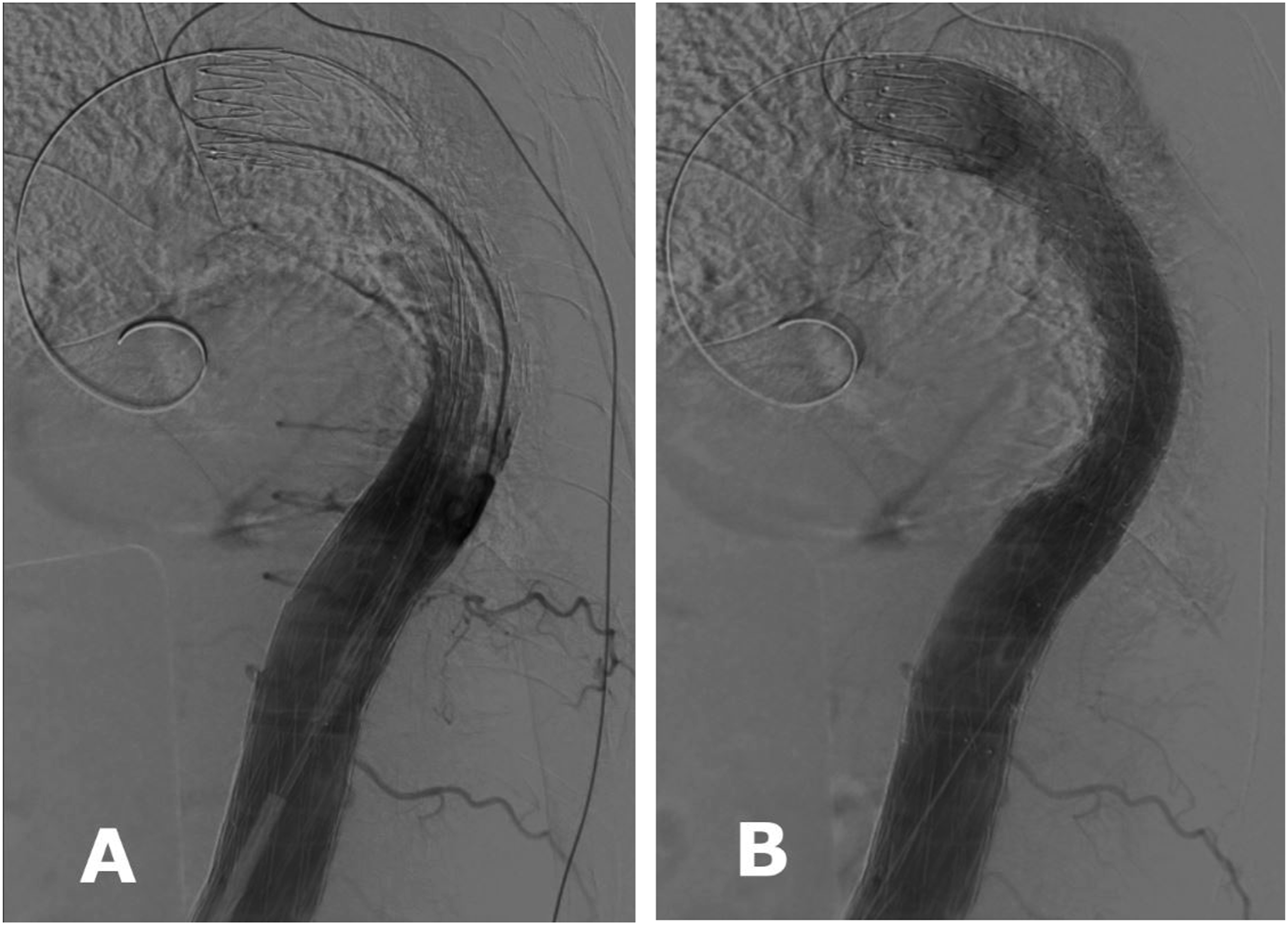
A Valiant Navion (Navion) (VNMC-37-31-C-207-TJ, Medtronic, Santa Rosa, CA, USA) was deployed on a clean table in a hybrid operating room and invertedly resheathed in the original sheath of the Navion. We recommend that an inverted stent graft is resheathed with two assistants. One operates the stent graft system while the other folds the stent graft to minimize the diameter by winding a silk thread around the stent graft without tying it. Once the next stent is half-folded using polyester tape with part of a Nelaton catheter, the silk thread can be wound around the stent graft more easily. The operator manually reloads it into the stent graft system as one assistant operates the stent graft system. This process is repeated until the inverted stent graft is entirely resheathed (Figure 2). A left common femoral artery (CFA) was exposed under general anesthesia. A GORE DrySeal Flex Introducer Sheath (20F; W. L. Gore & Associates, Inc., Flagstaff, AZ, USA) was inserted via the left CFA in the usual manner, and the inverted Navion was then delivered to the descending aorta through the Gore DrySeal Flex Introducer sheath. Operative angiography showed two large left ICAs (Figure 3A). The inverted Navion was deployed from the covered stent to the bare stent while preserving the lower large left ICA. Completion angiography showed that the gap between the stent graft and bare stent was repaired with preservation of the lower large left ICA (Figure 3B). The postoperative course was uneventful, and he was discharged on postoperative day 10 with relief of his severe pain. At one year after secondary TEVAR, CT showed that the diameter of the descending aorta had decreased with no separation of the stent grafts. A photo shows that the Navion is being invertedly resheathed using a silk thread and a polyester tape with part of a Nelaton catheter. A: Operative angiography shows two large left intercostal arteries. B: Completion angiography shows no endoleak of the descending aorta with preservation of the large left intercostal artery.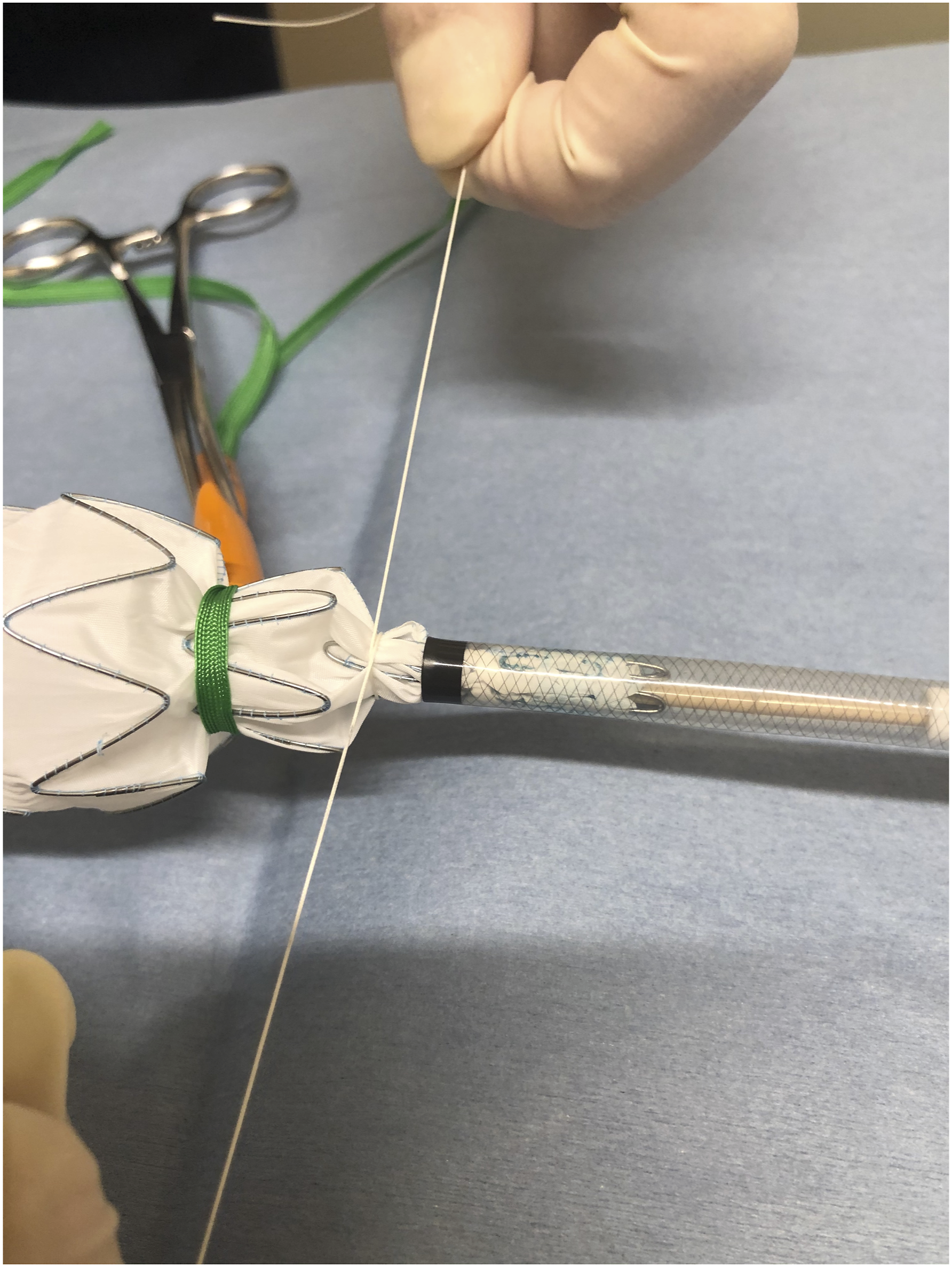
Discussion
Lombardi et al reported that the CS or device migration rate of the Zenith Dissection Endovascular Graft and Stent was 12.8% (11 of 86) and that only two patients required secondary intervention. Of these 11 patients (acute dissection, n = 7; nonacute dissection, n = 4), most cases of migration involved the stent graft. One case involved the dissection stent. 3 An inadequate landing zone, device undersizing, focally ruptured bare stent and stent misalignment were reported as causes of CS or migration.1,2 According to the instructions for use (IFU) of the Zenith Dissection Endovascular System―in order to prevent flaring of the bare stent―when overlapping the bare stent within the stent graft component, no more than half of a partially overlapped bare stent body should be un-overlapped. In the present case, the overlapping range after the initial TEVAR was insufficient. Furthermore, aortic elongation was observed by retrospective measurement. The distance from the left subclavian artery to the celiac artery was extended by 8 mm, whereas that from the top of the bare stent to the celiac artery was slightly extended by 1 mm for 3 years and 8 months. The main cause of CS in this case was considered to be elongation of the descending aorta. Chen et al. reported the mean rate of lengthening from the innominate artery to the celiac artery was 1.7 mm/year after TEVAR. 4 Considering aortic elongation and the IFU, as one segment of the bare stent of the Zenith Dissection Endovascular Stent is 2 cm, even one-half of a Zenith Dissection Endovascular Stent overlapping within a stent graft was considered to be an inadequate. An overlapping range of >1.5 times the length of a bare stent within a stent graft is needed to prevent CS.
There are no previous reports of treatment using an inverted thoracic stent graft, whereas there are some reports of the treatment of solitary iliac aneurysms using an inverted abdominal stent graft limb (including our previous report).5-8 As there was a large difference in the diameters of the proximal and distal landing zones, a long treatment range with the sacrifice of two large ICAs was needed to repair the CS. The inverted stent graft technique was selected to shorten the treatment range and preserve a large ICA. Prophylactic cerebrospinal fluid drainage in TEVAR is controversial. Although >20 cm of the aorta in the present case was covered, we did not use a lumbar drain in this case as only one pair of intercostal arteries was occluded and lower three pairs of intercostal arteries were preserved with a patent left subclavian artery, bilateral hypogastric arteries and lumbar arteries in this treatment. 9 Unfortunately, the Navion is not currently available. However, the Valiant Captivia stent graft system (Medtronic), which is similar to the Navion stent graft system and the same as the Endurant II (Medtronic) contralateral limb that we described in our previous report on the inverted stent graft technique, is available. 5 Therefore, deployment of an inverted Valiant Captivia is considered to be a theoretically feasible procedure for shortening the treatment range in the descending aorta.
Conclusion
Deployment of an inverted thoracic SG for the treatment of CS of the Zenith Dissection Endovascular Graft and Stent is a feasible and effective procedure to preserve ICAs. An overlapping range of >1.5 times the length of a bare stent within an SG is needed to prevent CS of the Zenith Dissection Endovascular Graft and Stent caused by aortic elongation.
Footnotes
Acknowledgments
We sincerely appreciate Ako Takusagawa for her cooperation in obtaining the photographs.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Satoshi Nishi has received consulting fees from Cook Medical Japan, Medtronic Japan Co., Ltd., MEDICO'S HIRATA INC., Japan Lifeline, and TERUMO CORPORATION.
Funding
The research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed Consent
The patient gave his informed consent for the publication of the details and images related to this report.