
Abstract
Background
Arterio-venous fistulae are often compromised by complications, notably thrombosis. We assess the 2 year follow-up data of a cohort of patients from a single vascular centre in the UK who underwent BCF or RCF creation with the objective of assessing the outcome differences and intervention rates between fistula types.
Materials and Methods
We retrospectively assessed a cohort of 195 patients who underwent creation of arterio-venous fistula (100 BCF, 95 RCF) between January 2016 and December 2018, following them up for 2 years assessing the outcomes and interventions on their AVFs. The outcomes assessed were primary and cumulative patency at 6 weeks, 6, 12 and 24 months. Multinomial logistic regression to account for confounding variables age, gender, procedure, side, anticoagulant, vessel size and co-morbidities was performed. A Kaplan-Meier analysis of time to endovascular intervention was also performed comparing RCF and BCF.
Results
Cumulative patency rates for BCF vs RCF were 91% vs. 89% at 6 weeks (X 2 (3, N = 194) = 4.70, P = .19), 83% vs. 76% at 6 months (X 2 (3, N = 188) = 7.72, P = .05), 78% vs. 69% at 12 months (X 2 (4, N = 175) = 5.37, P = .25) and 68% vs. 65% at 24 months (X 2 (4, N = 161) = 5.24, P = .24). Endovascular intervention rate becomes divergent at 5 months, with the steepest difference between 6 and 12 months. Comparative endovascular intervention rates between BCF and RCF were 20% vs. 31% at 6 months, 41% vs. 40% at 12 months and 40% vs. 49% at 24 months.
Conclusion
RCF seem to have significantly lower patency at 6 months and have higher endovascular intervention rates compared to BCF. A focussed surveillance protocol could prove effective in improving outcomes for RCF.
Background
Arterio-venous fistulae (AVF) provide a lifeline for end-stage renal failure (ESRF) patients to receive haemodialysis. The goal when creating an AVF is to create a long-term viable conduit for patients to stably dialyse through for as long as required. AVF confers significantly better survival benefit and dialysis function when compared to central venous catheters (CVC) and arteriovenous grafts (AVG) and thus AVF are the first line access for haemodialysis and preserved for as long as possible. 1
AVFs are planned with clinical assessment alongside duplex imaging of the upper or lower limb vasculature, commonly giving one of three options, radio-cephalic (RCF), brachio-cephalic (BCF) and basilic vein transposition fistulae (BVT). When there are multiple technically feasible possibilities patient preference is important such as dominant hand, but as a rule starting distally allowing for moving more proximal if the fistula fails. 2
It has been shown that RCFs have higher rates of primary failure and shorter durations of patency.3,4 However, they are less likely to cause steal syndrome and heart failure secondary to high-output, arm oedema and aneurysm as well as and are being cosmetically more appealing for the patients. They also preserve the upper arm veins for further access is required, and thus if technically feasible they are the first choice when creating a primary fistula. 5
AVFs are not free of complications and often do not mature into useable access for haemodialysis. Failure of AVF to be functional for dialysis is often due to early thrombosis, failure to mature or inadequate flow.6,7 If these complications are recognised early enough, then endovascular salvage procedures can be performed to force maturity or prolong fistulae survival. 8 The other possible complications, both acutely and in a chronic setting which can lead to failure or necessitate ligation are infection, aneurysm, lymphoedema, stenosis, congestive cardiac failure, steal syndrome or ischaemic neuropathy.
There is a large volume of data on short term outcomes of AVFs, and we recently published our own short term outcome data, 9 but the Medium-term outcomes are less well studied. The purpose of this study is to look at the 2-year follow-up data of a cohort of patients from a single vascular centre in the UK who underwent BCF or RCF creation with the objective of assessing the outcome differences and intervention rates between fistula types.
Materials and Methods
Data Collection
We retrospectively assessed a cohort of 195 consecutive patients who underwent creation of either BCF or RCF (100 BCF, 95 RCF) between January 2016 and December 2018 in Gloucestershire Hospitals NHS foundation trust. For all the renal access patients, their data is recorded on the Vital Data® database, which was used to identify all appropriate patients. Patients who received more complex access; AVGs, vein transpositions or lower limb fistulae were excluded. All AVFs were created in standard fashion using end-to-side anastomosis by three Consultant Vascular surgeons and warmed post-operatively for one hour.
The primary outcomes measures assessed were primary (unassisted) patency and cumulative patency rates at 6 weeks, 6, 12 and 24 months after creation. Secondary outcome measures were number of endovascular interventions at those time points, patency to transplantation and patient survival. After the point at which a patient received renal transplantation are died their fistula status was censored in the statistical analysis.
The demographic data collected was age, diabetes status, hypertension, antiplatelet or anticoagulant use, previous ipsilateral fistula, pre-operative dialysis status, and operating surgeon. Data was collected from hospital databases including TrakCare®, Infoflex®, EPR® and Vital Data®. Pre-operative vessel diameters were recorded from duplex imaging via PACS® software.. Endovascular intervention reports and images from performing interventionalist were access via PACS® software.
We define primary patency as uncomplicated use of AVF for dialysis without any procedural intervention since its creation. Secondary patency is defined as fistulae functional for dialysis as a result of intervention. We define cumulative patency as uncomplicated use of AVF for dialysis including any procedural or surgical intervention until the time of abandonment or censoring event (transplantation or death. If not dialysing, it was assessed clinically and/or evident on duplex ultrasound. AVFs were considered satisfactory if they met standard Doppler US criteria for maturation (volume flow of >600 ml/min; vein <6 mm from skin surface; vein diameter >6 mm with a length of >6 cm at that calibre).
The unit had no routine protocol for post-operative duplex scanning during the time period, ultrasound assessment was performed if poor maturation clinically or needling difficulty. Duplex scan assessed approximate volume flow in ml/min and for filling defects and stenoses, at which point the possibility of endovascular intervention would be explored.
Our institutions per-operative work up was a clinic appointment with a vascular surgeon followed by ultrasound assessment by a vascular scientist done with use of a tourniquet and the general guidance is for a minimum of 2 mm. Flow and degree of calcification is also assessed on duplex and considered by the vascular surgeon during planning.
All patients were seen either in clinic or on dialysis at six-weeks post-operatively and then followed up by the renal team at a minimum of 6 monthly intervals for the 2 year period after the initial 6 week follow-up.
Statistical Analysis
Summary data was created IBM SPSS version 26 and JASP .14.1.0 to give averages and ranges for basic demographic data. Multinomial logistic regression was used with all the co-variant demographic data to ensure none of the confounding variables were affecting the primary outcomes. Then subsequent univariate analysis was done assessing our primary outcome variables primary and secondary patency as well as intervention rate with key effector variables of fistula type and vessel diameter. Univariate analysis was Chi-squared testing, presented in the following format X 2 (degrees of freedom, N = sample size) = chi-square statistic value, p = P value. SPSS was used to construct a Kaplan-Meier analysis of time to endovascular intervention based on fistula type. R&D approval was granted and there were no conflicts of interest.
Results
Demographics
Numbers and Percentages of Patients Demographics within the Cohorts.
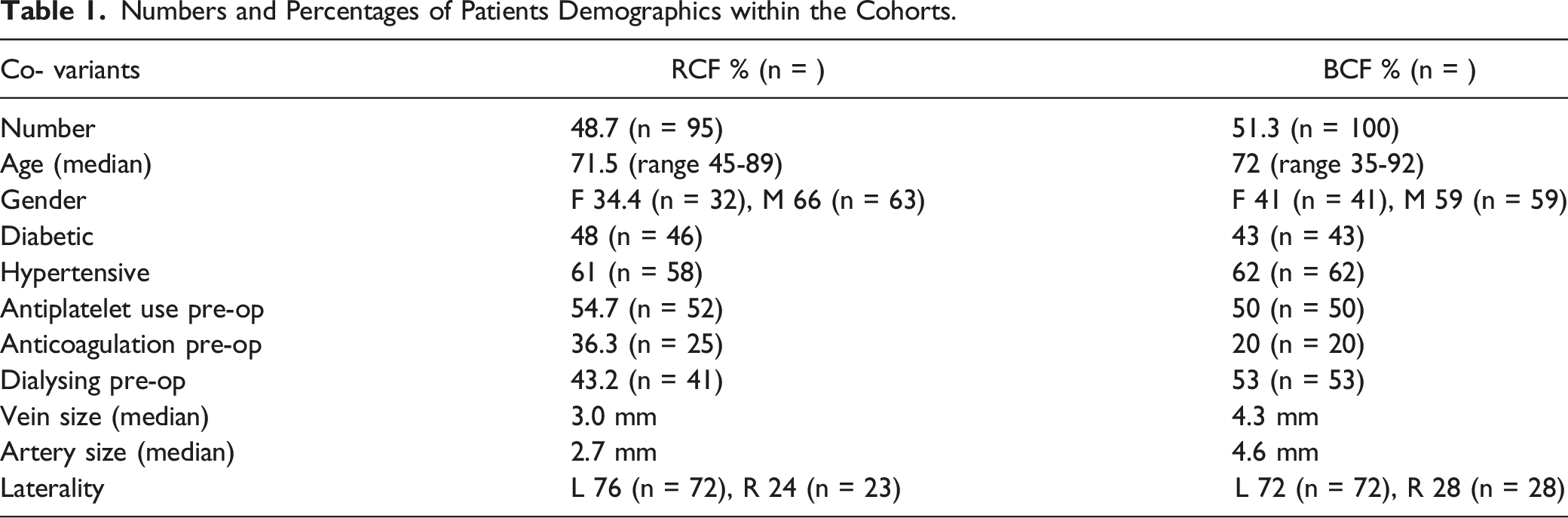
95 RCFs were created and had a median age of 72 years (range 38-85), of whom 34% were female and 66% male. 48% were diabetic and 61% hypertensive. 79% (n = 75) were primary fistulae, 76% left-sided and 24% right-sided. All of the patients whose fistula was not primary had previously had an attempted RCF on the contralateral side which had failed. The median diameter of artery and vein were 2.7 mm (range 1.6-4.5 mm) and 3.0 mm (range 1.6-5.0 mm) respectively.
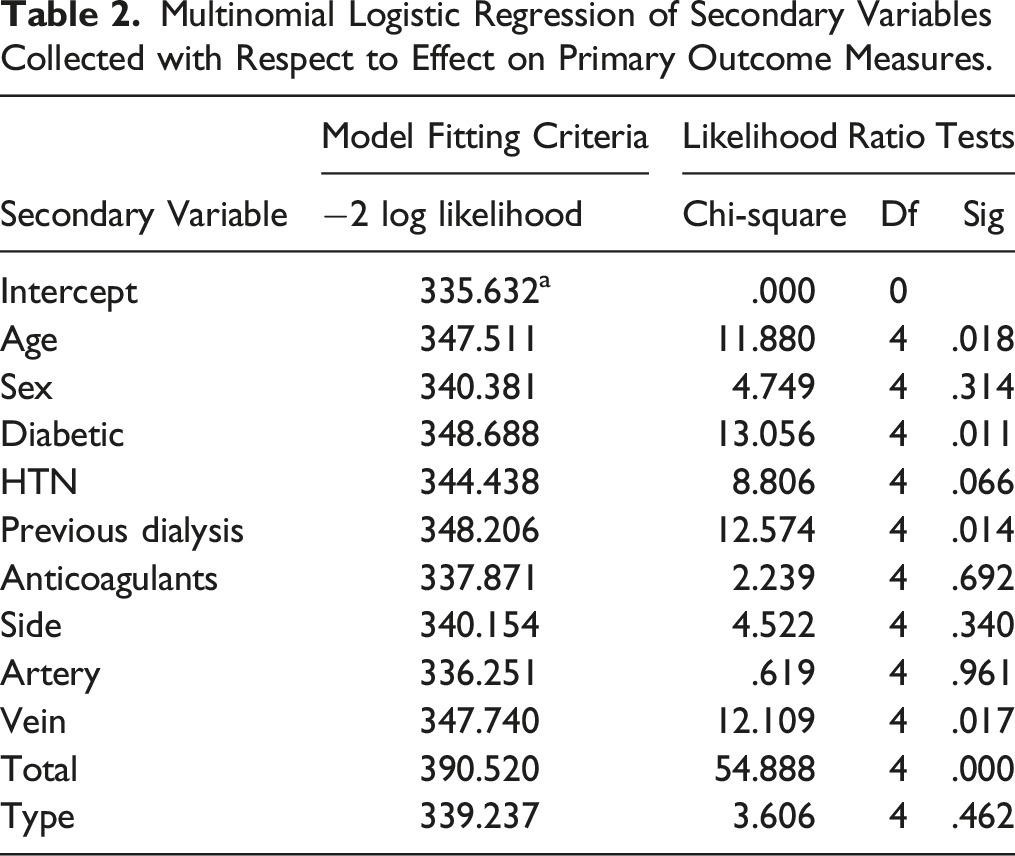
Multinomial Logistic Regression of Secondary Variables Collected with Respect to Effect on Primary Outcome Measures.
Patency
Cumulative patency rates for BCF vs RCF were 91% vs 89% at 6 weeks (X 2 (3, N = 194) = 4.70, P = .19); 83% vs. 76% at 6 months (X 2 (3, N = 188) = 7.72, P = .05); 79% vs. 69% at 12 months (X 2 (4, N = 175) = 5.37, P = .25) and 68% vs. 65% at 24 months (X 2 (4, N = 161) = 5.24, P = .24).
We see that early 6 weeks patency is comparable between the fistula types. Although at 6 months significantly higher BCFs were patent compared to RCFs, patency of both decline by 12 and 24 months and have comparable patency. The loss of BCF patency between 12 and 24 months is 79% to 68%, which is higher compared to the RCF patency which decreases from 69% to 65% (11% V 4%; P < .001). The rates of ligation for steal syndrome were 4% and 4.5% in RCF and BCF respectively at 2 years.
Survival and Patency to Transplantation
At 2 years, of 13 patients who died in the BCF group (13% mortality) 10 (77%) died with functioning access. Of the surviving cohort at 2 years, 14 had received renal transplants (16%), of these only 1 patient had failure of their fistula prior to transplantation which was a ligation done for steal syndrome.
In the RCF cohort, at 2 years, 21 patients had died (22% mortality), of whom 13 (62%) died with a functioning AVF. Of the surviving cohort at 2 years, 5 had received renal transplants (6.8%), all 5 of those patients had a functioning fistula at the time of transplantation.
Primary and Cumulative Patency
For the BCF cohort the primary unassisted compared to cumulative patency rate were at 89% and 91% at 6 weeks, 67% and 83% at 6 months, 49% and 79 at 12 months and 42% and 68% at 24 months respectively.
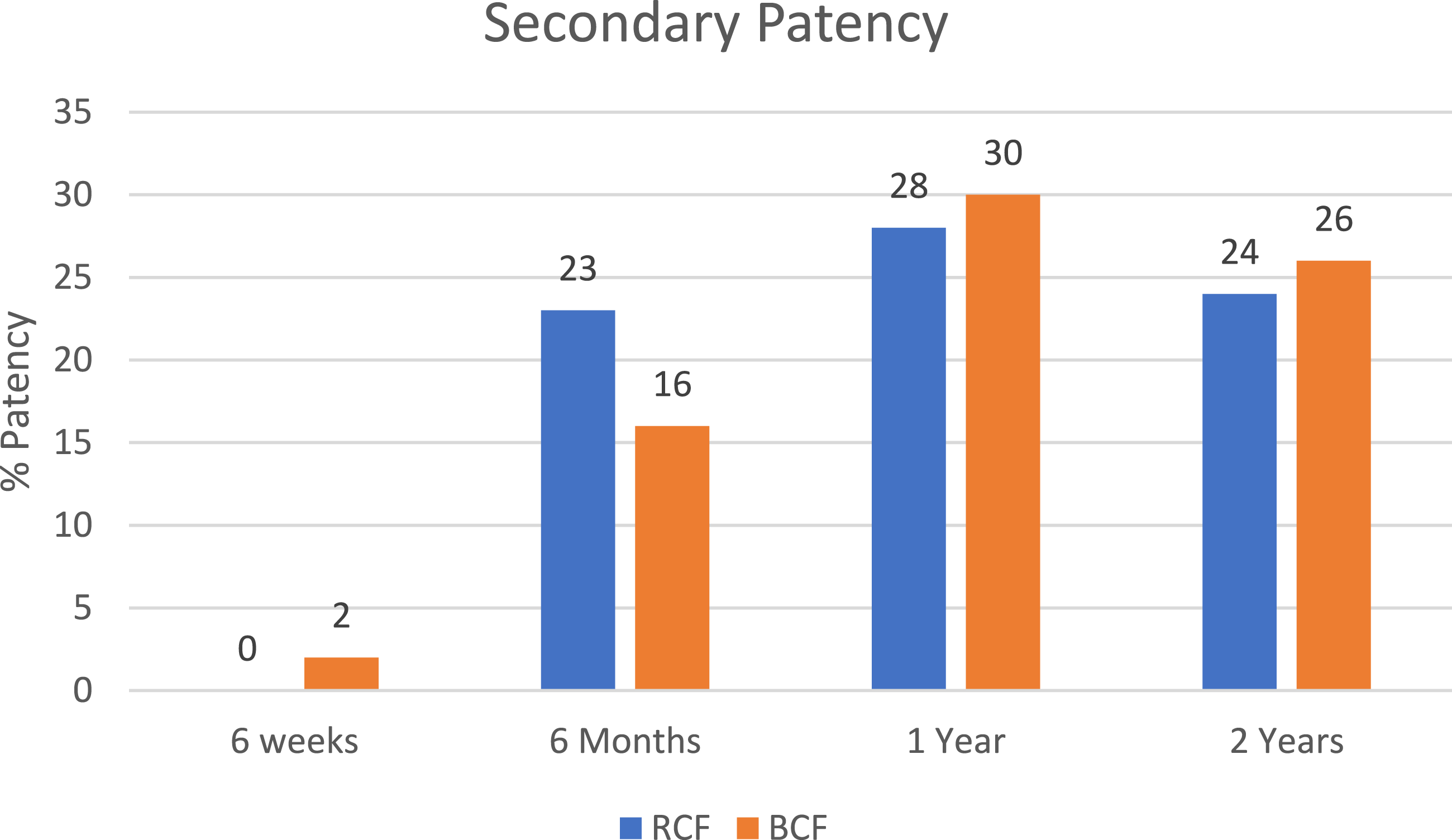
Comparing this to the RCF cohort, primary compared to cumulative patency rates were at 6 weeks 89% were primarily patent, with none having had intervention, 53% and 76% at 6 months, 43% and 69% at 12 months and 33% and 65% at 24 months respectively (see Figures 1 and 2). Primary patency rates between RCF and BCF at the timepoints of 6 weeks, 6 months, 1 year and 2 years. Secondary patency rates between RCF and BCF at the timepoints of 6 weeks, 6 months, 1 year and 2 years.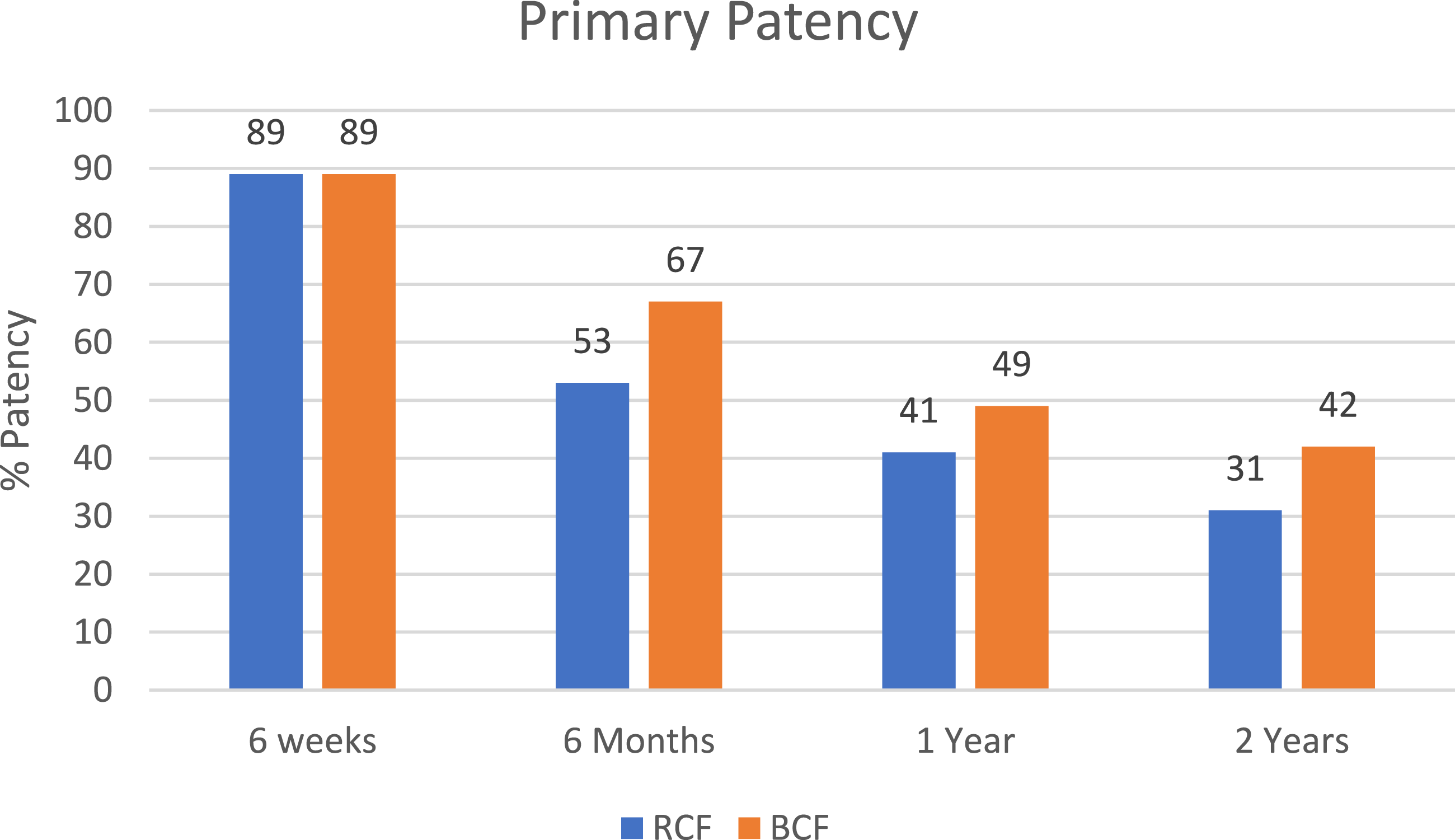
There is a trend within the RCF cohort that primary unassisted patency represents a smaller percentage of functioning fistulae, but when comparing the primary and cumulative patency between groups with univariant analysis at 6 weeks (X 2 (1, N = 176) = 1.89, P = .17), 6 months (X 2 (1, N = 150) = 2.90, P = .09), 12 months (X 2 (1, N = 127) = .019, P = .90), and 24 months (X 2 (1, N = 95) = 1.21, P = .27) we found no statistically significant divide between the types of fistulae.
Endovascular Intervention
When looked at interventions to salvage or mature a fistula and rates of intervention for BCF vs. RCF were 2% vs. 0% at 6 weeks (X 2 (1, N = 194) = .095, P = .75), 20% vs. 31% at 6 months (X 2 (1, N = 188) = 5.71, P = .01), 39% vs. 40% at 12 months (X 2 (1, N = 175) = .002, P = .96) and 39% vs. 49% at 24 months (X 2 (1, N = 161) = 1.21, P = .27). We see from this univariant analysis the RCFs at 6 months have a significantly higher intervention rate.
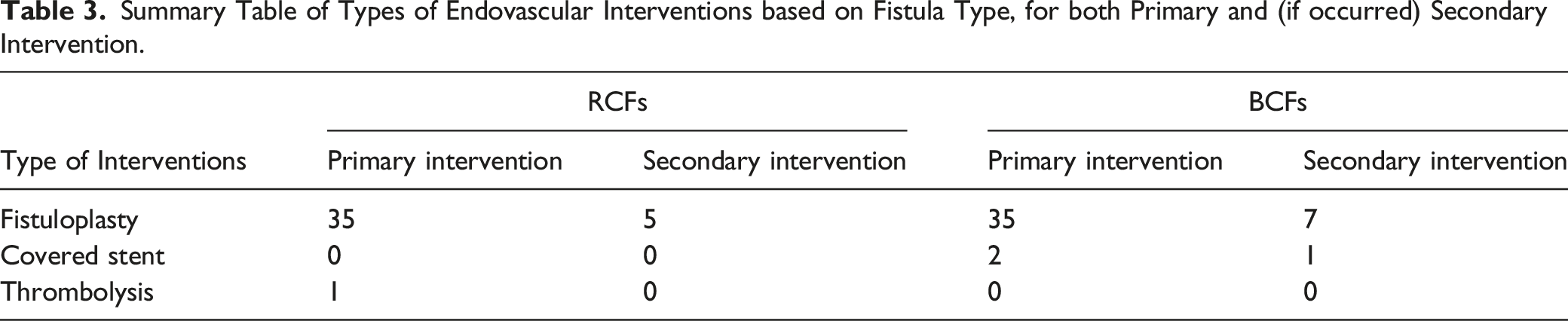
When this data is plotted on a Kaplan-Meier curve (see Figure 3) we see that endovascular intervention rate becomes divergent at 5 months, with the steepest difference between 6 and 12 months. The mean time to intervention is 4.14 months for both cohorts together. Nearly all of the endovascular interventions were fistuloplasty. There were no drug eluting balloons used; there were only 2 covered stents used and 1 case of fistula thrombolysis (see Table 3). For RCFs that received an intervention the mean number of procedures was 1.26, but for BCF is was 2. Kaplan-Meier of Endovascular interventions over time - the surviving fistulae have the endovascular interventions plotted at their time of intervention over the 24 month study period. Summary Table of Types of Endovascular Interventions based on Fistula Type, for both Primary and (if occurred) Secondary Intervention.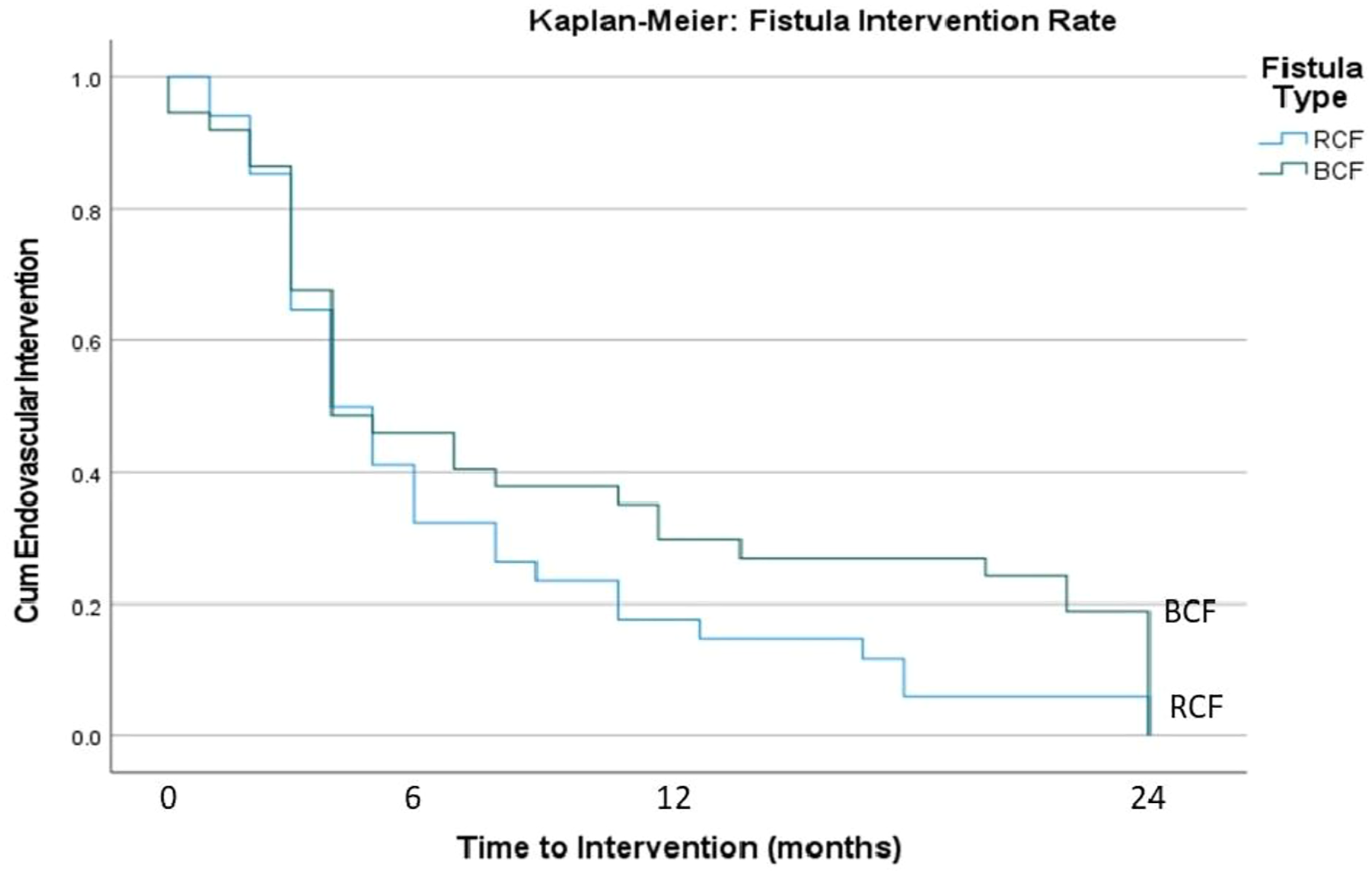
Vessel Diameter
There is significant difference in vessel size between the fistula types; for the RCFs an artery and vein median diameter of 2.7 mm and 3.0 mm, and for the BCFs an artery and vein median diameter of 4.6 mm and 4.3 mm (artery: Mann-Whitney U = 947, P < .001 and vein: Mann Whitney U = 2447, P < .001).
Taking the null hypothesis of the size of the vein or artery does not influence outcome (primary patency vs endovascular intervention vs occlusion), we did a Kruskal-Wallis between artery and vein size against outcome. We found that after 2 years the only statistically significant factor was vein diameter H(3) = 12.9 P = .005. The larger the vein the higher chance of primary patency; at 6 weeks vein P < .001; at 6 months vein P < .001,; at 12 months vein P = .028.
Mann-Whitney and effect size calculation at 6 months, we see that for venous diameter P < .001 rank-biserial correlation .401, and for arterial size P = .017 rank-biserial correlation .262, the rank correlation of the vein which is the effect size calculation is close to twice that of the artery, meaning variance within the vein size have a statistically greater impact on the outcome.
Using liner regression between the total number of endovascular interventions and the vessel diameters, both artery and vein there was no statistically significant relationship between size and number of interventions (artery: P = .81, vein: P = .95), we cannot therefore say that smaller vessels require more endovascular interventions.
Diabetes
Univariate analysis found no significant impact on outcome from all the secondary variables apart from diabetes. At 2 years with both RCF and BCF cohorts together diabetes had significant impact on outcome (X 2 (4, N = 161) = 9.74, P = .045), when the cohorts were taken individually P values were not significant for diabetes effect on outcome.
Discussion
This study demonstrates good patency rates with both types of fistulae and the results are comparable to many large-scale studies used in a meta-analysis by Jaishi et al. 10 We see that the RCFs have overall lower patency, most significantly at 6 months and an overall higher endovascular intervention rate, as well as a higher number of deaths with failed access. When analysing the nature of the fistulae this appears likely to relate to vessel size, with RCFs using significantly smaller vessels and vein size significantly correlating with outcome at 2 years and artery size correlating with outcome to 6 months, we find it likely that both artery and vein have an impact but that the vein is a more significant indicator, a finding also seen by Mendes et al and Lauvau et al.11,12 In other studies, by Wan et al and Shinstock et al there has been some further evidence that the arterial size is also of significant importance.13,14 The endovascular intervention rate first diverges at 5 months and is most divergent till 12 months. Salvage procedure keep fistula active longer, anticipating targets for intervention ahead of occlusion with proactive surveillance will likely improve fistula longevity. Given that RCF are at most risk, beginning a surveillance protocol improve outcomes and when selecting access following the adage: the right access for the right patient at the right time, a frail elderly patient with ESRF may have adequate vessels for a RCF, but it would be better they have one access with fewer interventions to last till their final illness whether that be BCF or even early canulation grafts. With this in mind for this cohort of patients a size of 2 mm for consideration of RCF may be insufficient and should be increased to 3 mm.
An important secondary variable is diabetes we found that the presence of diabetes significantly impacts patency rates at 2 years. There is some evidence from other studies that diabetic patients have lower patency rates and is thought to be due to calcification, and that concurrent diabetes and old age a significant predictor of poor primary patency. 15 Making the diabetic population undergoing RCF formation a particularly high-risk group for needing intervention.
When looking at both RCF and BCF, overall, as a function of access; survival to transplantation or death with a functioning AVF we considered a success, as it has provided its function for both these cohorts albeit to different ends. RCF overall had poorer outcomes, with higher mortality, and higher death with failed access, as well as lower rates of transplantation. While overall the outcomes with BCFs were better, there is a dip in patency which appears to happen later between 6 months and 1-year, routine surveillance of this cohort would be of benefit, but the time point at which it is of most use may be some months later to that of the RCF cohort. There may be a from all fistulae having focussed surveillance and results of SONAR study might provide this evidence. 16
Our study has several limitations, notably it is not a randomised study, and while the cohorts are comparable on the secondary variables assessed due to lack of randomisation there could be hidden variables that are disproportionate, crucially smoking status which is likely to have a significant impact on thrombotic events in AVFs, as Kler et al demonstrated previously. 17 Unfortunately, it was impossible to capture patient smoking status retrospectively. We have excluded, AVGs, transpositions and lower limb fistulae in this study which we think is reasonable when considering the question of surveillance as for the most part as there a very different in anatomical nature or in the case of AVGs the pathophysiology of stenosis and occlusion is different. There was a degree of heterogenicity in the assessment of a functionality of the fistulae; clinical assessment, duplex assessment, or functional dialysis were all used. By 2 years nearly all patients were still actively using their fistula for dialysis, or had been transplanted, or occluded the heterogenicity of assessment is likely not an issue.
While a study with a long follow-up is often a strength, in this case its important to be mindful of the pitfalls when relating the fundamentals at the time of creation, such as vessel size or type to longer term outcomes as over time these fistulae are used and their treatment will of course play a role in their longevity. Variables such as puncture technique, rate and sites which will be variable based on the dialysis nurse and centre, however there is a degree of homogeneity in their training limiting poor technique as an impact on occlusion.
Conclusion
In conclusion we have shown that vessel choice is key and that a larger vein is a major factor in fistula success and should be considered crucial when planning vascular access, that in RCFs by their anatomical nature carry a higher risk of intervention and failure. This data suggest that that early surveillance and intervention as required, could improve outcomes for RCFs, allowing sustained patency comparable with BCFs without ongoing need for increased intervention. As a result this study supports that RCFs, particularly diabetics would benefit from an early surveillance programme, at present there are ongoing RCTs attempting to establish definitive guidance. 16 Moreover, work of this nature is opening the discussion which is ongoing about the early or pre-emptive treatment of stenosis or swing points that may lead to thrombosis even when at that time point not causing a clinical problem or dialysis disfunction, a controversial topic which at present isn’t thought to be of benefit. 18
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.