
Abstract
Objective
Limb salvage is an important concern following complete oncologic resection for extremity soft tissue sarcoma (STS). Vascular reconstruction is essential for limb salvage. The purpose of this study was to evaluate the outcomes of vascular reconstruction in patients with extremity STS.
Methods
This is a retrospective, multi-center, case series of consecutive patients who underwent vascular reconstruction during extremity STS resection at 2 major centers in Korea. Demographics, reconstruction methods, type of conduit, surgical complications, graft patency, limb salvage rate, and patient survival were reviewed.
Results
From March 2005 to December 2020, 43 patients underwent vascular reconstructions during STS resection. Among the patients, 22 (51.2%) received arterial only, and 21 (48.8%) received simultaneous arterial and venous reconstructions. For the types of conduits, autologous saphenous veins (56.2%), artificial grafts (26.3%), and cryopreserved allografts (15.8%) were used. During a median follow-up of 23.8 months (interquartile range; 7.7-54.5), the overall primary patency of the reconstructed vessels was significantly higher in arteries than in veins (82.5% vs 56.3% at 12 months, P < .001). According to the type of conduit, the primary patency rate of autogenous vein seemed higher in venous reconstruction, however, there was no statistical significance in both arterial and venous reconstruction. There was no significant difference in primary arterial patency rate (P = .132) or incidence of surgical complications including postoperative edema or wound problem whether or not simultaneous venous reconstruction was performed with arterial reconstruction. The overall limb salvage rate and patient survival were 97.4%, 95.1%, and 89.4% and 91.9%, 81.7%, and 65.4% at 12, 24, and 36 months, respectively.
Conclusions
Patency rates were poorer in venous reconstruction than in arterial reconstruction. In terms of arterial patency and postoperative complication, the role of simultaneous arterial and venous reconstruction seems not essential, however, it needs to be evaluated in future studies.
Introduction
Soft tissue sarcomas can occur anywhere in the body, but limbs or limb girdles are most commonly affected. 1 Because surgical resection with wide margins is the mainstay of treatment with or without other treatments, 1 efforts are needed to preserve functional ability after complete oncologic resection, especially in patients with extremity STS. Moreover, treatment focused on limb salvage rather than amputation has become the norm since comparable survival outcomes between primary amputation and limb salvage groups2,3 and acceptable patency rates of reconstructed vessels were reported. 4
The percentage of adjacent vascular invasion in extremity STS was reported to be 0-5%. 5 The principle of complete oncologic surgery is en bloc resection, and limb amputation is sometimes unavoidable without vascular reconstruction.
Vascular reconstruction is performed in various situations. However, due to the rarity of extremity STS, no specific recommendations or guidelines are available for this specific need for vascular reconstruction. In this study, we analyzed and compared the patency rates of reconstructed vessels and analyzed the overall survival and limb salvage rates in patients with extremity STS who underwent vascular reconstruction as part of a limb salvage procedure during STS resection. We also tried to evaluate whether simultaneous venous reconstruction with arterial reconstruction is more beneficial than artery-only reconstruction.
Materials and Methods
This study was approved by the Institutional Review Board of Samsung Medical Center (SMC) (Approval number: 2021-10-110) and Seoul National University Hospital (SNUH) (Approval number: 1802-127-926), and obtaining informed consent from patients was waived due to its retrospective nature.
This study is a retrospective multi-center case series of 43 consecutive patients with pathologically proven STS or locally aggressive fibromatosis in the extremities who underwent vascular reconstruction following oncologic resection with invaded vessels at SMC or SNUH from March 2005 to December 2020.
For review of those patients, the following information was retrieved from electronic medical records and imaging studies: demographics, histologic type of the tumor, reconstruction method and type of conduit used for vascular reconstruction, surgical complications, graft patency, and oncologic outcomes including local recurrence rate and overall patient survival.
For all patients diagnosed with extremity STS, a multidisciplinary team consisting of a surgical oncologist (orthopedic surgeon specialized in extremity STS), medical oncologist, radiologist, and vascular surgeon discuss the evaluation and treatment details preoperatively. All patients in this study underwent magnetic resonance imaging (MRI) for local staging of the tumor and to evaluate the extent of invasion into the adjacent neurovascular structures. In addition to MRI, computed tomographic angiography (CTA) was performed to evaluate the extent of vascular invasion, intact venous system, and to identify appropriate autogenous vein conduits. Routine consultation with a vascular surgeon was performed if vessel reconstruction is anticipated.
After en bloc resection of a tumor that had invaded vascular structures, vascular reconstruction was performed. Selection of conduit types was at the discretion of the vascular surgeon based on length and caliber of the resected vessel and availability of a qualified autologous vein graft.
The great saphenous vein, if available, was the first choice for femoral arterial reconstruction in both centers. We tried to use the contralateral great saphenous vein to preserve venous outflow of the affected side, however, the ipsilateral great saphenous veins were also used by operator’s discretion based on vein quality and required length of conduit especially for both artery and vein reconstruction. Cryopreserved allografts were available in the 1 center (SMC) that operates its own biobank. If an appropriate allograft satisfying well-matched caliber and required length was available, it was the first choice of conduit, especially for iliac vessels and femoral venous reconstruction. The other difference between the 2 centers was the preference for simultaneous artery and vein reconstruction: SMC preferred artery-only reconstruction if the deep femoral venous drainage system was intact, whereas SNUH preferred simultaneous artery and vein reconstruction if possible.
Statistical Analysis
Continuous variables are expressed as median and interquartile range. Categorical variables are shown as count with percentage. The Kaplan-Meier method was used to estimate the patency of reconstructed vessels, overall limb salvage rate, and patient survival rate. The patency of reconstructed vessels and patient survival were evaluated using the log-rank test. P values less than .05 were considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics Version 25 (IBM, Armonk, NY, USA).
Results
Baseline patient characteristics and oncologic treatments of 43 patients who underwent vascular reconstruction with extremity STS resection.
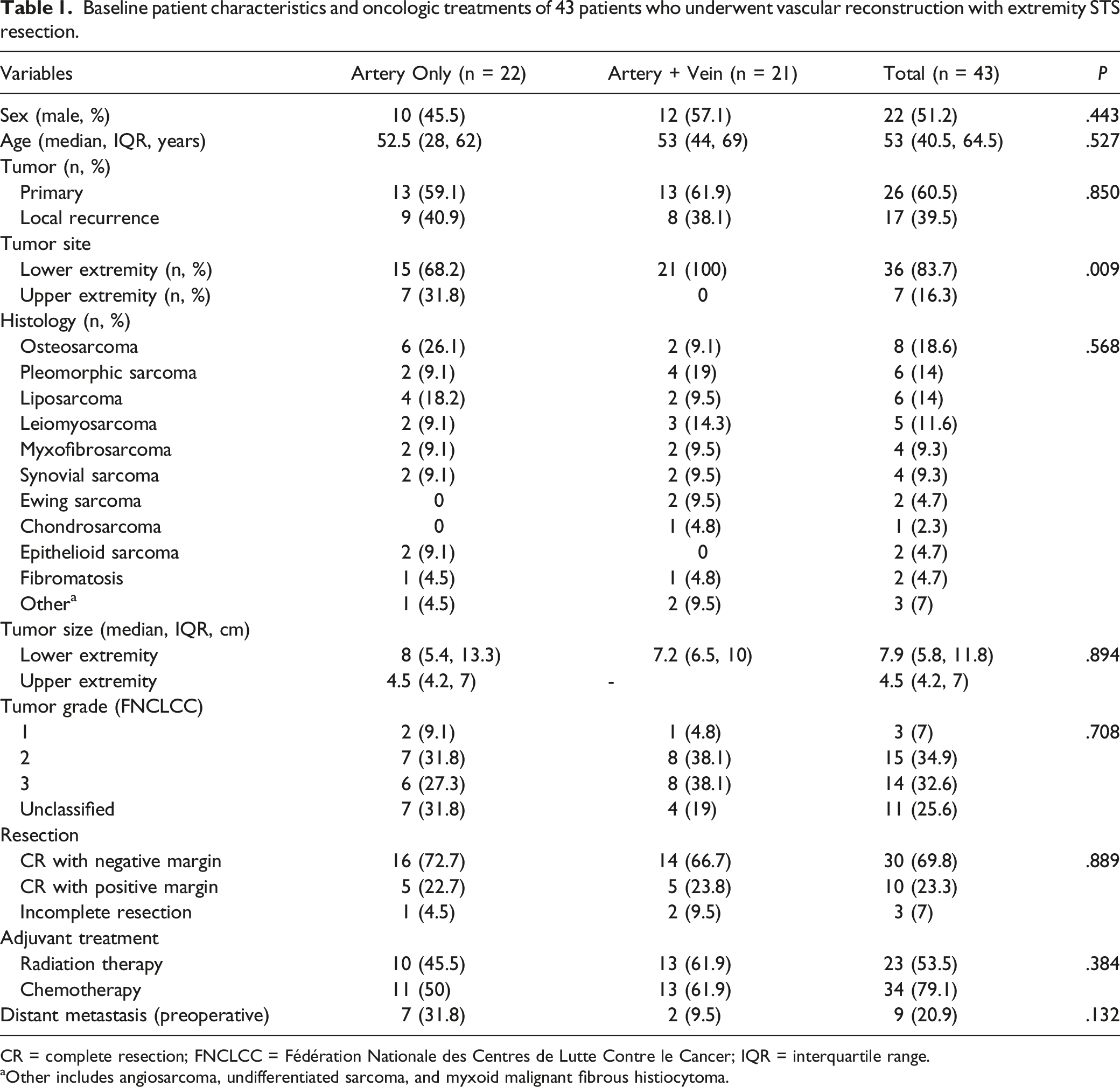
CR = complete resection; FNCLCC = Fédération Nationale des Centres de Lutte Contre le Cancer; IQR = interquartile range.
aOther includes angiosarcoma, undifferentiated sarcoma, and myxoid malignant fibrous histiocytoma.
Types of vascular reconstruction and conduits used.
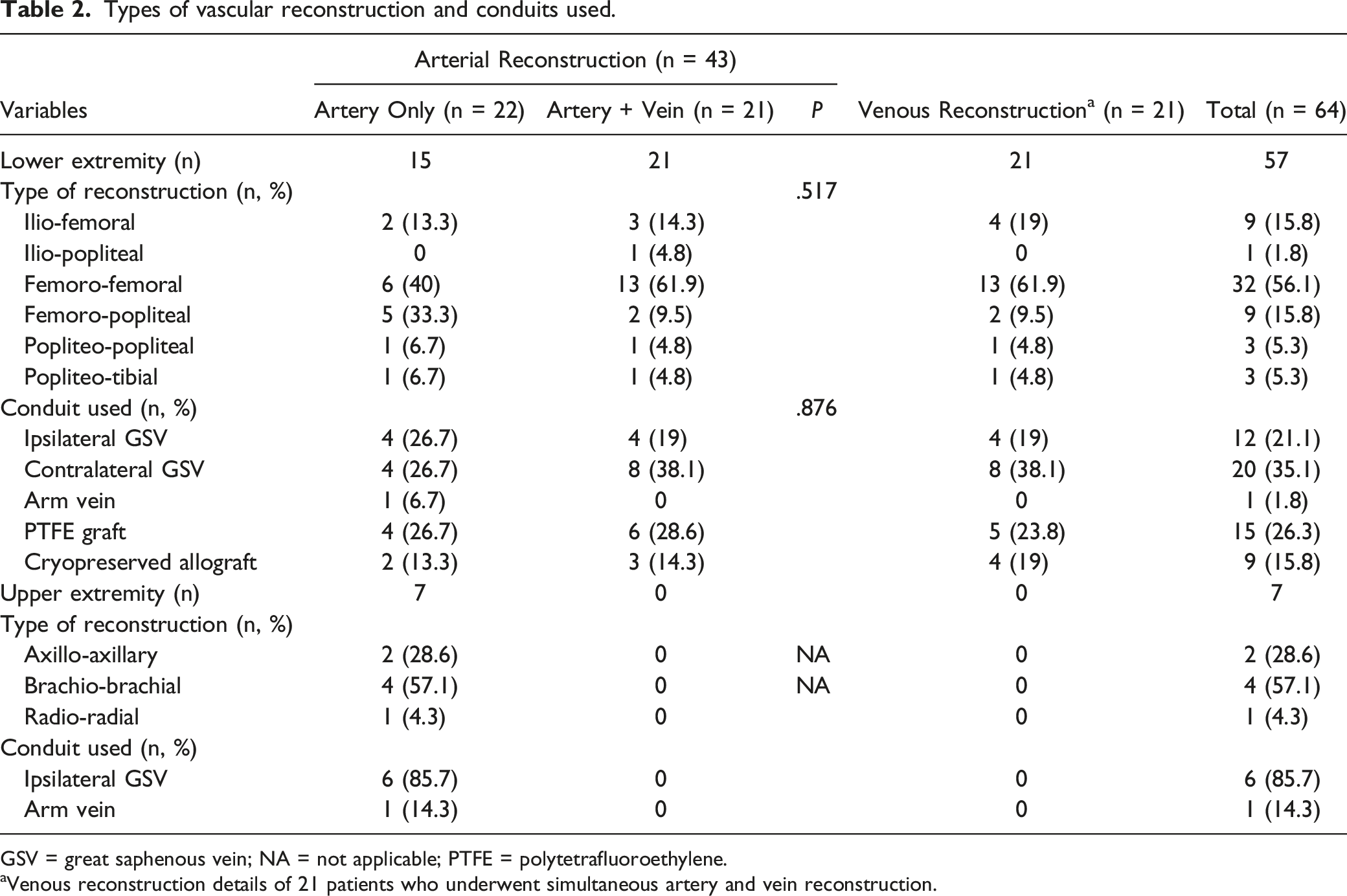
GSV = great saphenous vein; NA = not applicable; PTFE = polytetrafluoroethylene.
aVenous reconstruction details of 21 patients who underwent simultaneous artery and vein reconstruction.
Surgical complications after vascular reconstruction in 43 patients who underwent vascular reconstruction with extremity STS resection.
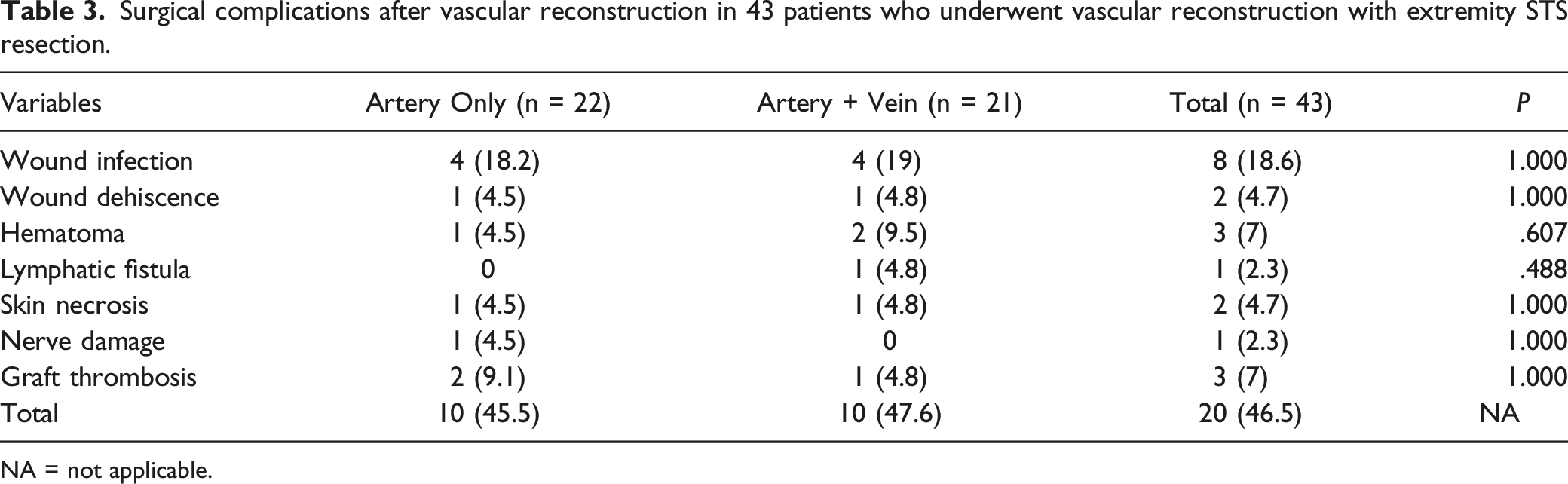
NA = not applicable.
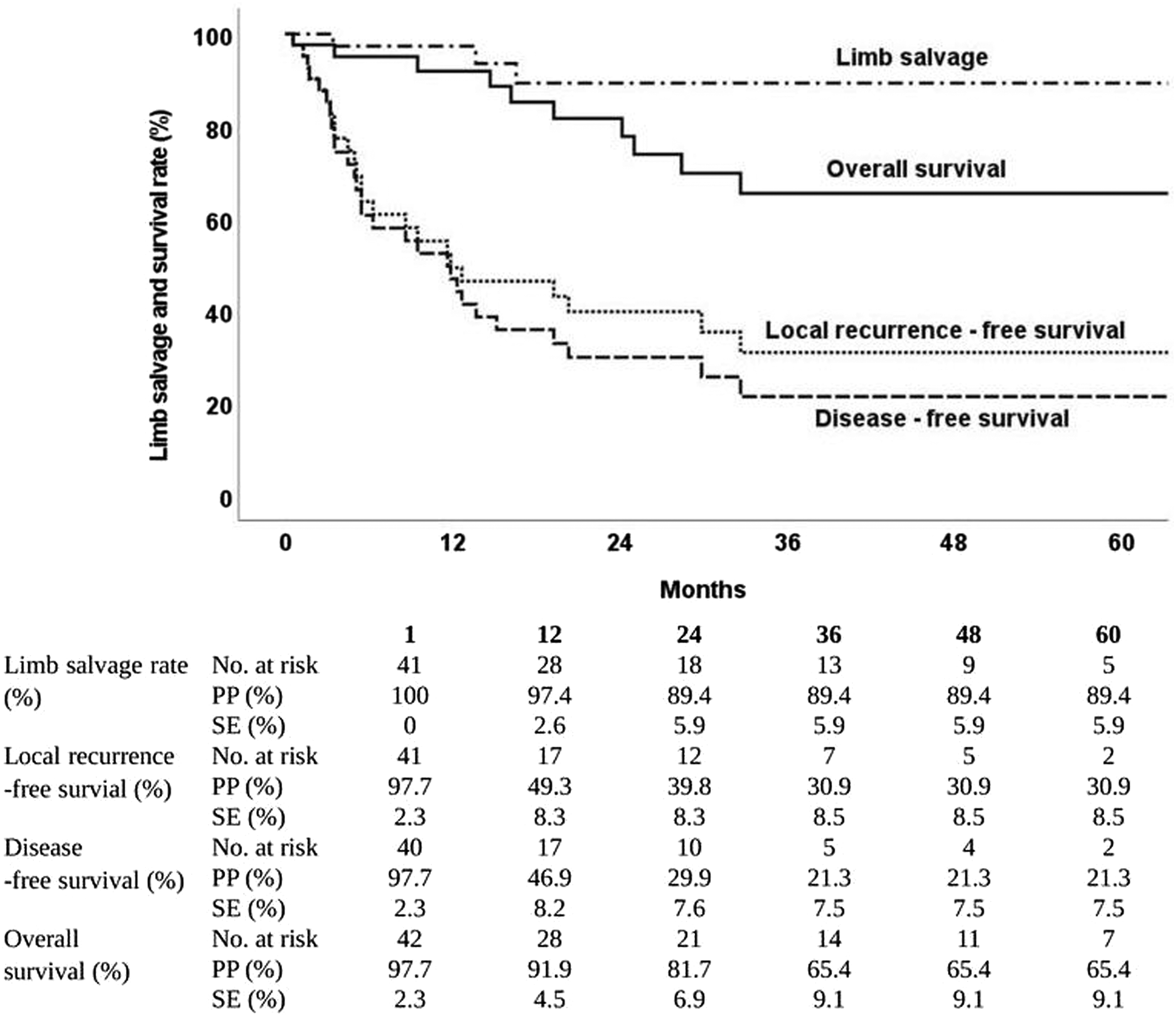
The median follow-up duration was 23.8 months (IQR 7.7-54.5). A Kaplan-Meier analysis of the patency rates in vascular reconstruction revealed that the secondary and assisted primary patency rates of arterial reconstructions were significantly longer at all time points than were all the patency rates of venous reconstructions (P < .001) (Figure 1). The Kaplan-Meier analysis in Figure 2 shows the primary patency rates stratified by type of conduit used in arterial (Figure 2(a)) and venous (Figure 2(b)) reconstructions. In arterial reconstruction, the patency rates did not differ significantly according to type of conduit used (P = .202). In venous reconstruction, autogenous veins seemed a higher primary patency rate at 12 months (74.1%) and thereafter (59.3%) compared to cryopreserved allografts (25% and 25%), however there was no statistical significance (P = .077). Comparison of primary arterial patency rates between the artery-only reconstruction group and the simultaneous artery and vein reconstruction group is shown in Figure 2(c). The primary arterial patency did not differ significantly between the 2 groups (P = .132). The overall limb salvage rate was 97.4% at 12 months, and 89.4% at 24 months and thereafter (Figure 3). The overall survival rates at 12, 24, and 36 months were 91.9%, 81.7%, and 65.4%, respectively, and the local recurrence-free survival and disease-free survival rates were smaller than the overall survival rates (Figure 3). Kaplan-Meier estimates of primary, assisted primary, and secondary patency rates in vascular reconstruction after extremity STS resection. Kaplan-Meier estimates of primary patency rates in (a) arterial and (b) venous reconstructions according to the type of conduit used, and (c) primary arterial patency rates with and without simultaneous venous reconstruction. Kaplan-Meier estimates of overall limb salvage rate and survival outcomes in 43 patients.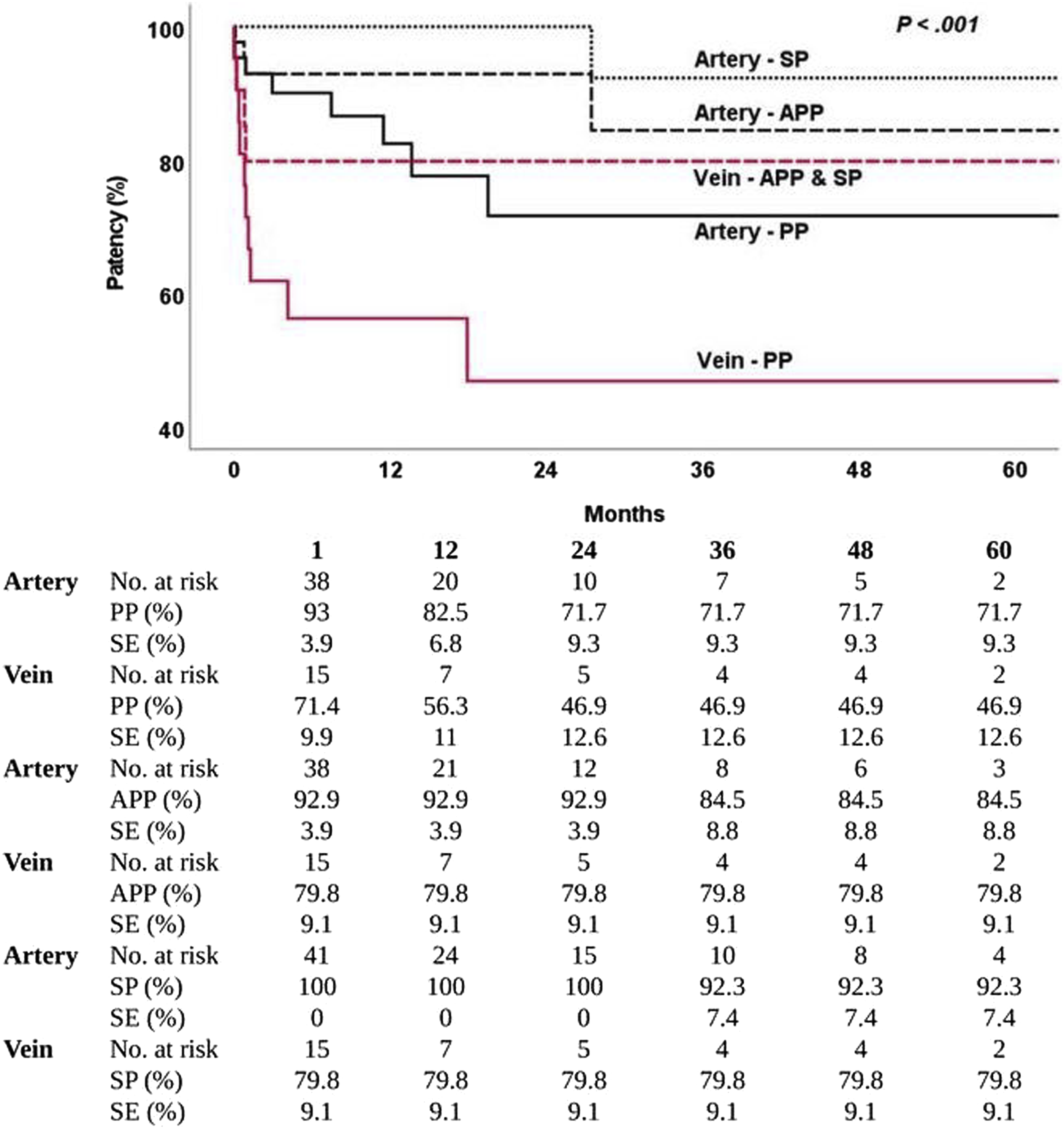

Discussion
Early literature on extremity STS treatment reported a 5-10% ultimate amputation rate in patients with sarcoma of the limbs. 7 However, limb amputation severely limits functional ability. Extremity STS affects people with a median age in the 50s, 8 who are usually socioeconomically active in society, as in our patients. Chemotherapy for STS has increased the 5-year survival rates with localized tumors up to 60%. 9 Clinicians should provide their best efforts to preserve patient limbs as far as oncologic outcomes are not affected.
For limb salvage in patients with extremity STS that infiltrates major vascular structures, vascular reconstruction is essential. Because reconstructive procedures in cancer surgery are common for vascular surgeons,10,11 a part of the authors have reported outcomes of vascular reconstructions in extremity STS based on a single-center data in 2018. 12 Importance of planned assistance of vascular surgeons was emphasized in another recent study with a positive impact on outcomes. 13 The objective of our study at this time was to update and re-evaluate the outcomes of vascular reconstructions in extremity STS based on a large group of patients from 2 tertiary centers. This study showed a high limb salvage rate of 89.4% at 24 months after surgery.
In our previous study, the best conduit for bypass in terms of graft patency was the autologous saphenous vein. 12 Since then, types of conduit used have been expanded to include cryopreserved allografts. Analyses of graft patency according to type of conduit were separately performed for arterial and venous reconstructions. In arterial reconstruction, the primary patency rates did not differ significantly by type of conduit. In venous reconstruction, autologous vein grafts seemed having a better primary patency rate than cryopreserved allografts or prosthetic grafts, however, without statistical significance. Nishinari et al 14 recommended an autologous graft for venous revascularization from their prospective follow-up results of 20 patients with malignant limb tumors. Despite reports of various graft patency rates in previous studies, the results have generally been better in arterial reconstruction than venous reconstruction.15,16 Shah et al 15 calculated patency according to conduit type in their recent study and found that synthetic grafts seemed to produce poorer patency rates in veins (20%) than in arteries (71.4%). Mlees et al 17 reported a result similar to ours for arterial patency according to conduit and found that arterial graft occlusion rate was not significantly greater in the synthetic graft group than in the autologous vein group. Not much is known about use of cryopreserved allografts for vascular reconstruction, specifically in extremity STS. One case reported use of an allograft for arterial reconstruction, but it did not provide follow-up results. 18 They recommended using a cryopreserved arterial allograft if an appropriate length and caliber of autologous vein was unavailable. Based on our results, allografts for arterial reconstruction seem to be a reliable choice of conduit in terms of patency rate. However, there are some general concerns about allografts, such as secondary deterioration from stenosis or dilatation. 19 We did not experience such complications in our patients during the follow-up period, but further research is required to verify the feasibility and safety of cryopreserved allografts.
Even though several previous studies have dealt with vascular reconstruction for patients with extremity STS, necessity of simultaneous venous reconstruction with arterial reconstruction is controversial. The indications for venous reconstruction are impairment of all 3 lower-limb venous drainage systems of the superficial femoral, deep femoral, and saphenous veins as the result of tumor resection.20,21 Some other authors noted that patients benefit from venous reconstruction if development of collateral circulation is not achieved following obstruction of the main venous drainage systems.22,23 A group of researchers who emphasized the need for venous reconstruction reported a longer duration of limb edema postoperatively with artery-only reconstruction. 23 In a report of Matsushita et al, 24 10 patients underwent limb-sparing surgery with only arterial reconstruction, and chronic venous disease including symptoms of severe edema and eczema was observed during the median 48 months of follow-up.
We prefer to perform vein reconstruction if an autologous conduit or cryopreserved allograft is available. However, if a prosthetic graft is the only option of conduit, then the decision to reconstruct the vein depends on the vascular surgeon. In our study, the incidence of surgical complications did not differ significantly between the artery-only and simultaneous artery and vein reconstruction groups. Clinicians who do not always perform venous reconstruction argue that vein ligation does not negatively affect limb preservation. 25 Although it is not a case of oncovascular surgery, Verma et al 26 reported that 35% of their patient developed limb edema which responds to compression therapy after femoral vein harvest for aorta reconstruction as far as preserving the profunda vein and popliteal genicular draining veins. Intact popliteal genicular draining veins were also known to be subsequent for compensating femoral vein occlusion. 27 The patency rate of venous reconstruction is also an issue. In general, long-term patency rate of the major venous reconstruction is not much reported, however, low velocity and low pressure nature of venous blood flow and propensity for post-reconstructive thrombosis might be major causes of inferior venous patency rate to the arterial patency rate. 28 Unsatisfactory results were reported despite distal arterio-venous fistula formation and use of anticoagulants.21,25,29 Our results also indicate an inferior patency rate in venous reconstruction than in arterial reconstruction.
In addition to surgical complications, we also compared the arterial graft patency rate between the artery-only and simultaneous artery and vein reconstruction groups and found no difference. Not much is known about how simultaneous venous reconstruction affects arterial patency, and further investigation is needed.
Conclusions
In patients who underwent extremity STS resection with appropriate vascular reconstruction, the overall limb salvage rate was considerable. Regarding the patency rates of different conduits, autologous veins seemed to be the best option for both arterial and venous reconstruction, however, without statistical significance. The patency rates of venous reconstructions were poorer than those of arterial reconstructions. Based on our results, venous reconstruction performed concurrently with arterial reconstruction did not affect the incidence of surgical complications or arterial patency rate after limb salvage surgery for extremity STS. However, additional future studies based on a larger number of patients are needed to evaluate the role of simultaneous arterial and venous reconstruction.
Limitations
This was a retrospective study with a small sample size and inherent selection bias. Postoperative use of antiplatelet or anticoagulant medications after vascular reconstruction was not standardized but varied by vascular surgeon. Due to the retrospective nature of the study, we were unable to collect precise information about functional outcomes following limb salvage surgery, including phlebolymphedema or level of unassisted mobilization. Regular postoperative imaging follow-up is not standardized, which could result in underdiagnosis of graft failure or other complications. However, this study did include various types of reconstruction conduits with relatively long follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.