
Abstract
Introduction
Single branched thoracic endografts (SBTEs) have been designed for pathology requiring zone 2 seal during thoracic endovascular aortic repair (TEVAR). Numerous criteria must be met to allow for their implantation. Our aim was to analyze anatomic suitability for a next generation SBTE.
Methods
We reviewed 150 TEVAR procedures between 2015 and 2019. Proximal seal was: zone 0 in 21 (16%), zone 1 in 4 (3%), zone 2 in 52 (40%), zone 3 in 45 (35%), and zone 4 or distal in 7 (5%). We analyzed the Zone 2 patient’s angiograms and CT angiograms using centerline software to measure arterial diameters and length in relation to the left common carotid artery (LCCA), left subclavian artery (LSA) and proximal extent of aortic disease to determine if patients met anatomic criteria of a novel SBTE.
Results
Zone 2 average age was 64.4 ± 16.3 years; 34 patients were male (65%). Indications for repair were aneurysm (N = 9, 17%), acute dissection (N = 14, 27%), chronic dissection with aneurysmal degeneration (N = 7, 13%), intramural hematoma (N = 9, 17%), penetrating aortic ulcer (N = 5, 10%), and blunt traumatic aortic injury (BTAI, N = 8, 15%). LSA revascularization occurred in 27 patients (52%). Overall, 20 (38.5%) of the zone 2 patients met anatomic criteria. Patients with dissection met anatomic criteria less frequently than aneurysm (33% [10 of 30] vs 64% [9 of 14]). Patients treated for BTAI rarely met the anatomic criteria (1 of 8, 13%). The main anatomic constraints were an inadequate distance from the LCCA to the LSA takeoff and from the LCCA to the start of the aortic disease process.
Conclusion
Less than half of patients who require seal in zone 2 met criteria for this SBTE. Patients with aneurysms met anatomic criteria more often than those with dissection. The device would have little applicability in treating patients with BTAI.
Keywords
Introduction
Thoracic endovascular aortic repair (TEVAR) has become the preferred treatment for disease involving the descending thoracic aorta due to its lower procedural morbidity and mortality compared to open surgical repair.1-8 TEVAR has been shown to be effective in patients who present with a variety of conditions including aortic aneurysm, acute and chronic aortic dissection, penetrating aortic ulcer (PAU), intramural hematoma (IMH), and blunt traumatic aortic injury (BTAI).3-14
There are multiple stent grafts approved by the United States Food and Drug Administration (FDA) to treat thoracic aortic pathology. The individual TEVAR devices have varying indications to treat differing pathologies of the descending thoracic aorta. When disease extends proximally to involve the aortic arch, TEVAR placement may require coverage of one or more of the supra-aortic branches to achieve an appropriate seal. This practice is often used to avoid the morbidity of an open repair.15-19
Single branched thoracic endografts have been designed and evaluated to achieve proximal seal in Ishimura zone 2 18 while maintaining LSA patency through the use of a branched stent graft.20,21 Although the necessity of revascularization during intentional coverage of the LSA remains controversial, The Society of Vascular Surgery practice guideline recommend routine LSA revascularization for elective TEVAR procedures. 22 The most common surgical method to revascularize the LSA is left common carotid artery (LCCA) to LSA bypass or transposition. 23 Endovascular solutions such as laser fenestration or placement of parallel grafts have also been described.15,16,19 The goal of the single branched thoracic endograft is to maintain LSA perfusion in a single procedure without the need for adjunctive surgical or endovascular interventions.20,21
The purpose of this study is to determine the utility of a single branched thoracic endograft for the treatment of aortic pathology requiring LSA coverage to achieve proximal seal. We examined the anatomy of a group of patients treated with TEVAR achieving proximal seal in zone 2 to define which patients met anatomic eligibility requirements and to define the applicability of the device.
Methods
Study Population
We analyzed anatomic suitability for a proposed single branched thoracic endograft which remains in development. This novel graft is based on the Mona LSA TEVAR graft (Medtronic, INC, Santa Rosa, CA, Figure 1).
20
We conducted a retrospective review of all patients who underwent TEVAR at our academic referral center between 2015 and 2019. The study was approved by the institutional review board of University Hospitals Cleveland Medical Center prior to enrollment (IRB 20180847) with a waiver of informed consent granted for retrospective data analysis. Patients were divided into groups based on location of the Ishimura zone where proximal seal was achieved. Patients who underwent TEVAR after ascending aortic replacement or replacement of the hemiarch without reimplantation or bypass of the supra-aortic branches were classified similarly. Patients who underwent TEVAR following mediastinal debranching with or without ascending aortic replacement were classified as Zone 0. Patients who underwent TEVAR in conjunction with elephant trunk procedures or who underwent antegrade thoracic graft placement during mediastinal repair were excluded. The Valiant Mona LSA device (Medtronic Inc). Note the LSA branch stent graft component mated with the main stent graft.
The group which achieved proximal seal in zone 2 were examined and make up the cohort for this study. We reviewed these patient’s operative angiograms and preoperative computed tomography angiograms (CTA). CTAs were performed per our institutional protocol using .8-2 mm slices. Three-dimensional, center-line reconstructions were created using Sectra PACS vessel analysis software (Sectra AB). We used Sectra’s imbedded program tools to create centerline images and to measure lengths and diameters. Imaging was reviewed to determine if patients met the anatomic inclusion and exclusion criteria for the proposed device.
Indications for Repair
The indications for repair were ascertained from chart and imaging review. Patients were broadly classified into 3 groups: 1, aortic aneurysm; 2, aortic dissection; or 3, trauma (blunt thoracic aortic injury, BTAI). The aneurysm group consisted of degenerative aortic aneurysm, saccular aneurysm, or penetrating aortic ulcer (PAU). The dissection group consisted of acute aortic dissection, chronic aortic dissection with aneurysmal degeneration, and intramural hematoma (IMH). PAU associated with intramural hematoma (IMH) were classified as IMH. Patients with aortic trauma from BTAI were included. Patients with penetrating aortic trauma were excluded.
Device Specifics
The proposed device is an off-the-shelf, modular, single branched thoracic endograft designed to achieve zone 2 seal while maintaining LSA patency. It combines a main stent graft (MGS) component and a branch stent graft (BSG) designed for deployment into the LSA. Proposed sizing for the MSG include diameters of 28, 31, 34, 37, 40, 43, and 46 mm. The grafts are all 150 mm in length and are not manufactured in tapered diameters. Proposed sizing for the BSG are diameters of 10, 12, or 14 mm. All are 40 mm in length.
Anatomic Criteria.
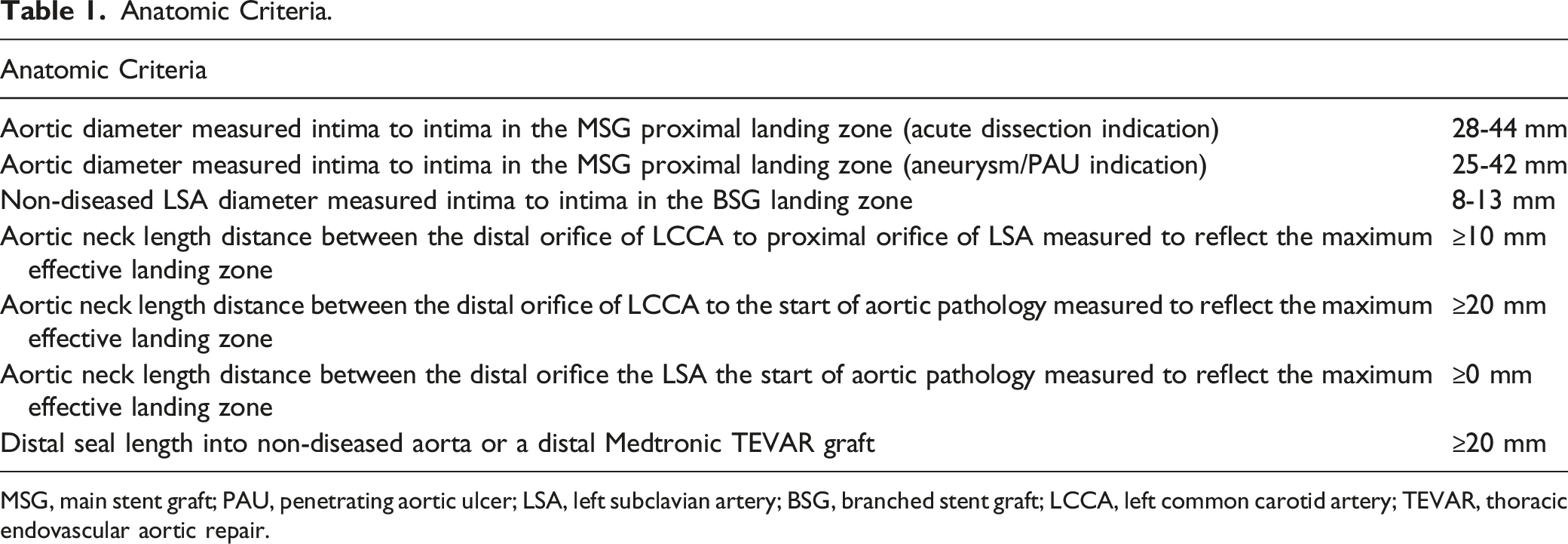
MSG, main stent graft; PAU, penetrating aortic ulcer; LSA, left subclavian artery; BSG, branched stent graft; LCCA, left common carotid artery; TEVAR, thoracic endovascular aortic repair.
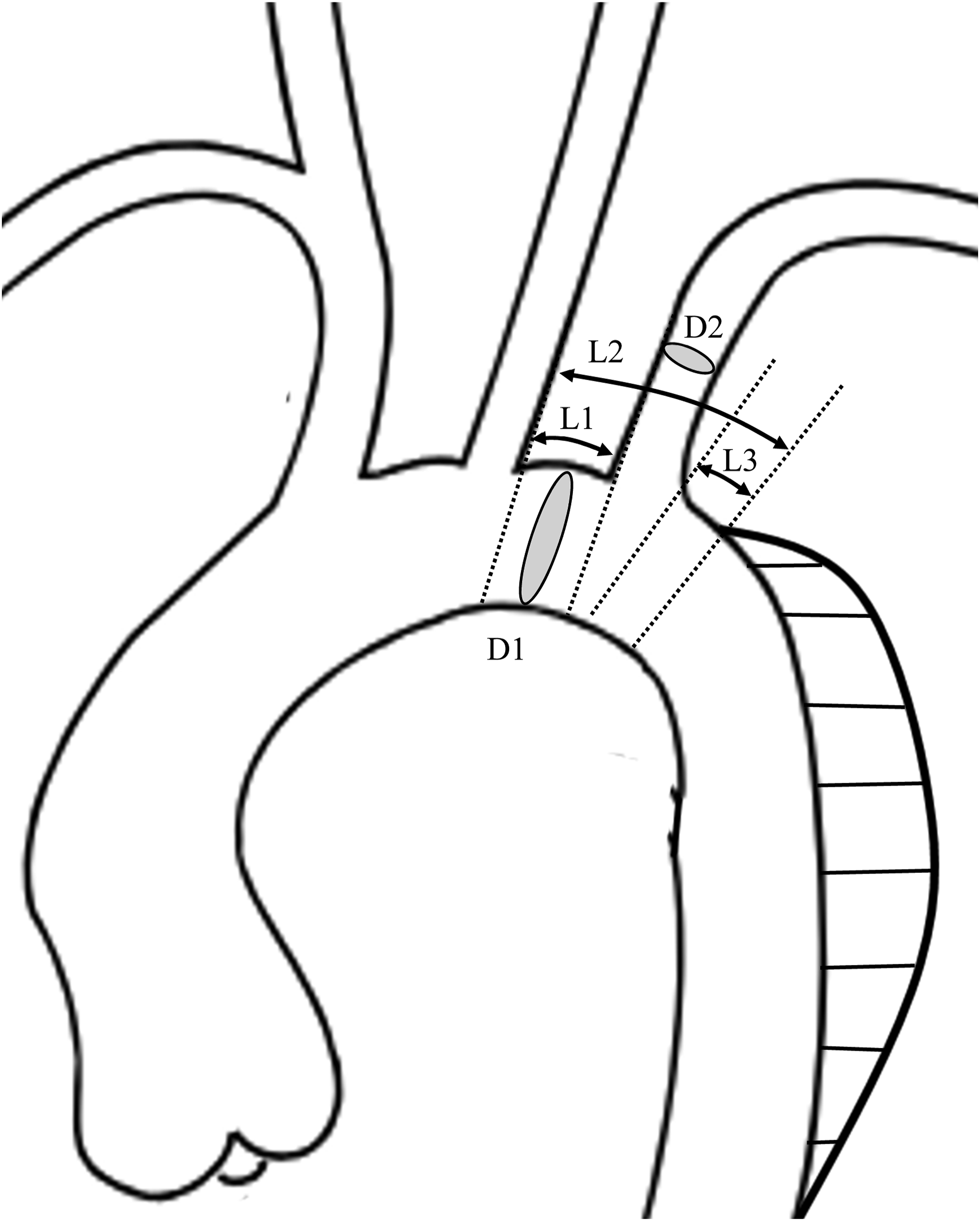
Diameter and length measurements to meet anatomic suitability. D1, diameter of the aorta in zone 2 at the site of proximal seal; D2, diameter of the left subclavian artery (LSA); L1, length from the left common carotid artery (LCCA) to the LSA; L2, length from the LCCA to the proximal extent of aortic disease; L3, length from the LSA to the proximal extent of aortic disease.
Statistical Analysis
Categorical variables are presented as counts and percentages, while continuous variable are presented as a mean ± standard deviation (SD). Categorical variables were compared using chi-square analysis. Continuous variables were compared between all groups using analysis of variance (ANOVA) and between 2 groups using Wilcoxon signed-rank tests. Statistical significance was set at P < .05. All statistical analysis was performed using SAS JMP Pro software (version 14; SAS Inc).
Results
Overall Cohort
Overall, 150 TEVAR procedures were performed in 129 patients at University Hospitals, Cleveland Medical Center between 2015 and 2019. Average age was 64.9 ± 14.7 years; 77 were male (60%). Indications for repair were thoracic aortic aneurysm (N = 44, 34%), acute aortic dissection (N = 24, 19%), chronic aortic dissection with aneurysmal degeneration (N = 26, 20%), intramural hematoma (N = 9, 7%), saccular aneurysm from penetrating aortic ulceration (N = 15, 12%), and BTAI (N = 11, 9%). In these 129 patients, the most proximal seal was achieved in zone 0 in 21 (16%), zone 1 in 4 (3%), zone 2 in 52 (40%), zone 3 in 45 (35%), and zone 4 or distal in 7 (5%).
Zone 2 Patient Cohort
Indications for TEVAR Procedure and Distribution of Those Who Met the Anatomic Criteria Expressed as N (%).
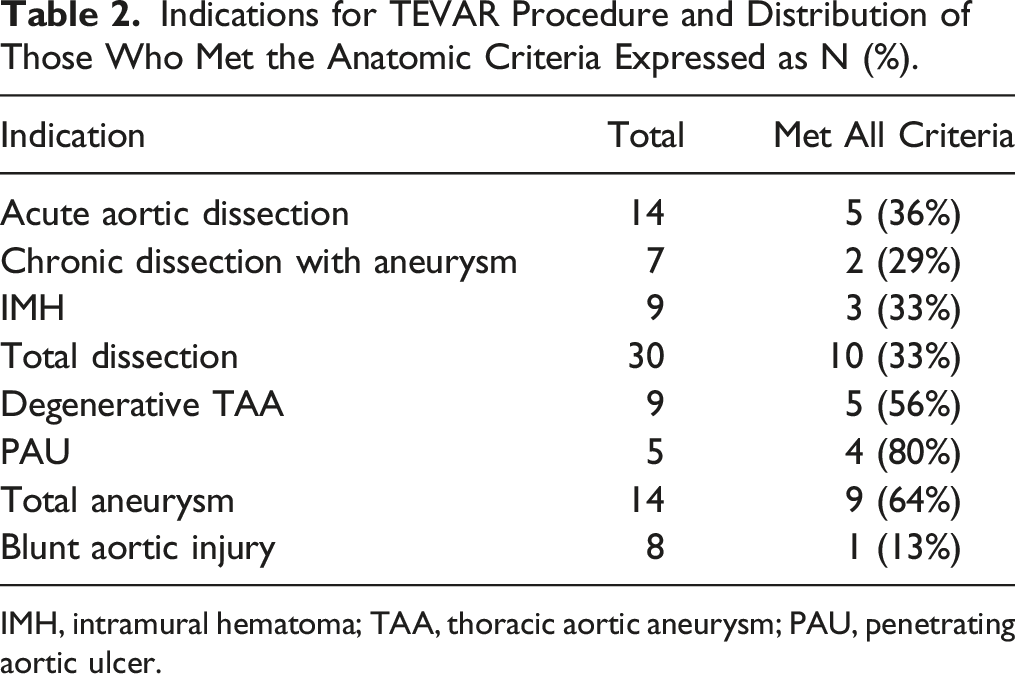
IMH, intramural hematoma; TAA, thoracic aortic aneurysm; PAU, penetrating aortic ulcer.
Anatomic Eligibility
Of the 52 zone 2 patients, 20 (38.5%) met the anatomic eligibility for the device and 32 (61.5%) did not. In relation to all TEVAR procedures performed during the study period, the device was suitable in 20 of 129 patients (15.5%). The distribution of patients who met or failed to meet the anatomic criteria by procedure indication are summarized in Table 2. Patients who underwent TEVAR for an aortic dissection indication met anatomic criteria in 33% (10 of 30). Patients treated for an aneurysm indication met criteria in 64% (9 of 14 patients). Patients treated for blunt aortic injury (BAI) rarely met the anatomic criteria with only 1 of 8 patients suitable (13%).
Gender, Mean Age and Mean Values of the Anatomic Criteria: For All Patients, for Those Who Met Criteria, and for Those Who Failed to Meet Criteria.
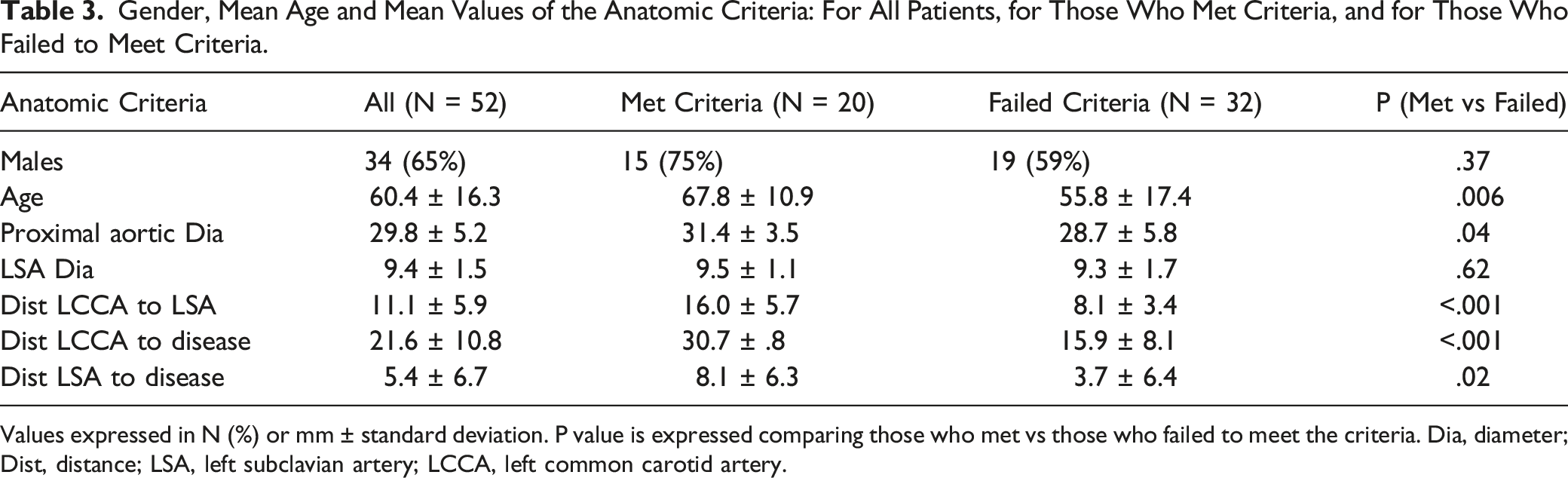
Values expressed in N (%) or mm ± standard deviation. P value is expressed comparing those who met vs those who failed to meet the criteria. Dia, diameter; Dist, distance; LSA, left subclavian artery; LCCA, left common carotid artery.
Number Who Failed Each Anatomic Criteria for All Patients and for the Group of Patients Excluding Traumatic Indication.
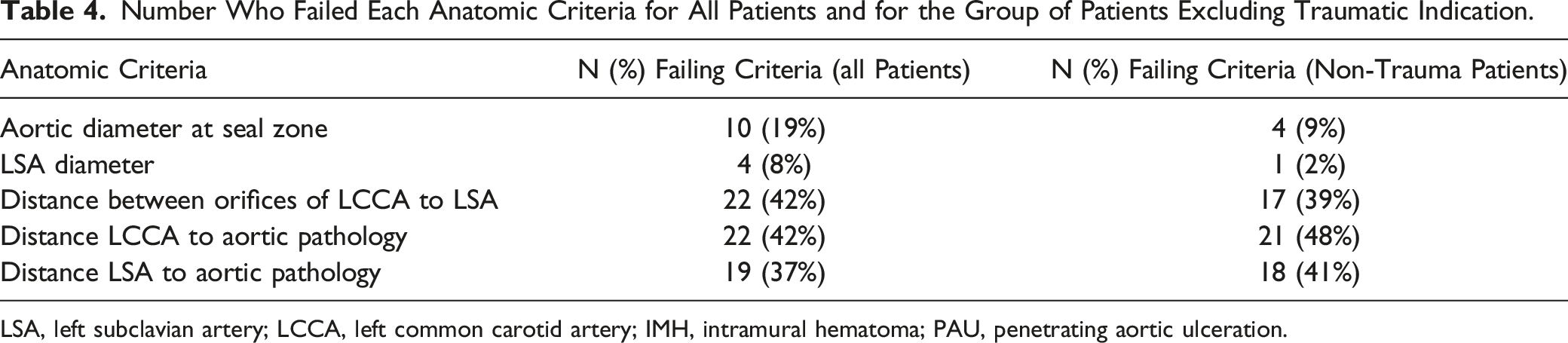
LSA, left subclavian artery; LCCA, left common carotid artery; IMH, intramural hematoma; PAU, penetrating aortic ulceration.
Reason for Failure to Meet Criteria
Number of Patients Who Failed to Meet the Anatomic Criteria by Indication for Repair and Number of Patients Who Failed Each Anatomic Criteria by Indication (Patients Could Fail to Meet Multiple Anatomic Criteria).
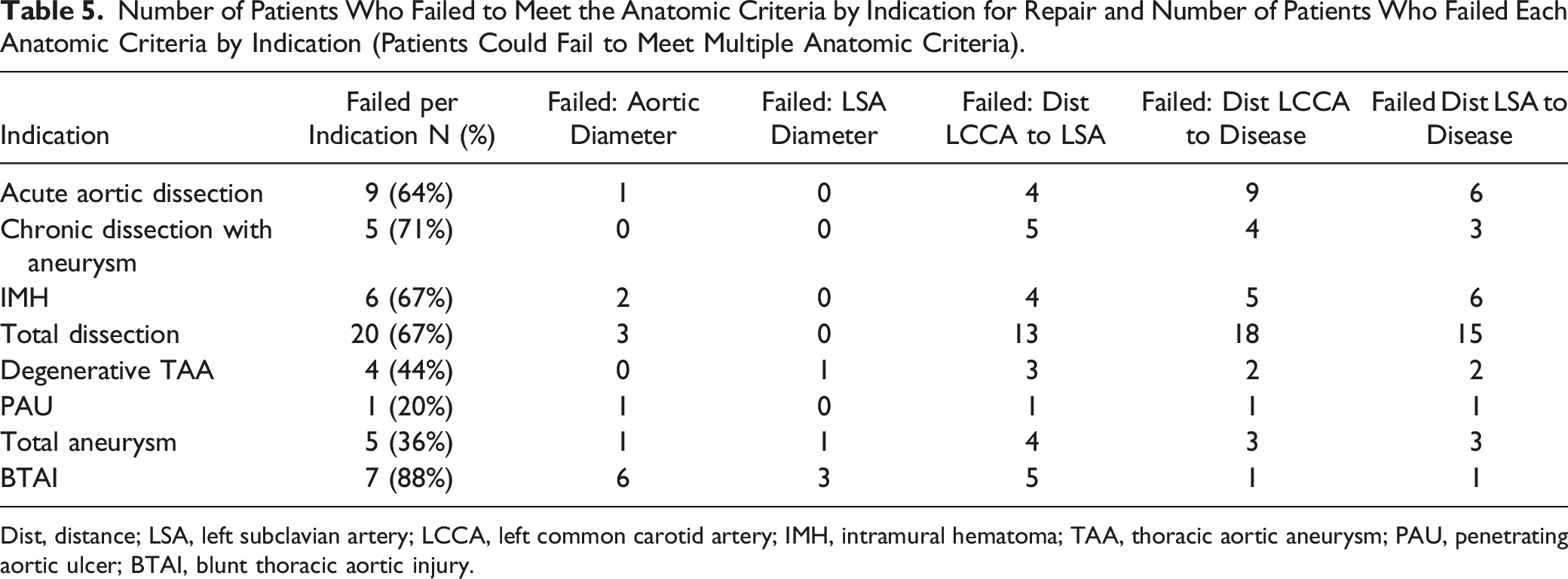
Dist, distance; LSA, left subclavian artery; LCCA, left common carotid artery; IMH, intramural hematoma; TAA, thoracic aortic aneurysm; PAU, penetrating aortic ulcer; BTAI, blunt thoracic aortic injury.
Acute aortic dissection
Only 1 patient failed due to small aortic diameter (24 mm) and none failed due to size of the LSA. The most common reason for failure was inadequate distance between the proximal extent of the dissection and both the LCCA and the LSA. One of these also had inadequate distance between the LCCA and LSA. Two others failed for inadequate distance between the LCCA and LSA. Three of the excluded patients were close to qualifying: one failed due to a LCCA to LSA distance of 8 mm and a LCCA to aortic dissection distance of 19 mm and 2 failed due to LCCA to aortic dissection distance of 18 mm in one and 16 mm in the other.
Chronic aortic dissection with aneurysmal degeneration
Four of the 5 patients who failed to meet criteria had inadequate distance from the LCCA to the LSA and had the aortic disease too close to the LCCA and LSA. One patient failed due solely to inadequate distance between LCCA and the LSA (3 mm).
Intramural hematoma
All 6 of the patients who failed had disease extending proximal to the LSA. Five of the 6 also had inadequate distance from the LCCA to the start of the aortic disease and 4 of the 6 had inadequate distance LCCA to LSA. Two of these had aortic diameter which failed to meet the aortic dissection diameter criteria (28-44 mm) at 24 mm and 26 mm.
Thoracic aortic aneurysm
Two of the 4 patients who failed to meet criteria had inadequate distance from the LCCA to the LSA and inadequate distance from the proximal extent of the aneurysm to both the LSA and LCCA. One patient failed due solely to a small LSA (6 mm) and another solely due to inadequate distance from the LCCA to LSA.
Penetrating aortic ulcer
Only 1 patient did not meet criteria due to a small aorta (24 mm) and inadequate distance for all 3 distance measures.
Blunt thoracic aortic injury
6 of the 8 who failed to meet criteria had an inadequate aortic diameter, 3 had inadequate LSA diameter and 5 had inadequate distance from the LCCA to the LSA. The only patient who met criteria was a 55-year-old man with an aortic diameter of 30 mm.
Discussion
More than 25 years after Dake and colleagues introduced the concept of endovascular repair of the thoracic aorta, 24 TEVAR has gained acceptance as the preferred treatment for thoracic aortic pathology.1-14 Since that time, numerous trials have shown lower rates of morbidity and mortality for TEVAR compared to open surgical repair of the descending thoracic aorta. This is true not only for patients who present for treatment of thoracic aneurysm and PAU, indications for which the initial grafts were approved, but also for the treatment of acute or chronic dissection.1,4,9,10,12 Additionally, TEVAR has been commonly used to repair the aorta after blunt thoracic aortic injury.6,8,14
The benefits of TEVAR have led to an expansion of its application to include landing the graft into the aortic arch.15-18 Achieving a proximal seal in the aortic arch requires coverage of one or more of the supra-aortic branch vessels. There are a variety of methods which have been utilized to revascularize these covered aortic branches including mediastinal debranching, extra-anatomic bypass, parallel stent grafts, graft fenestration, and the use of branched endovascular stent grafts.15-18,20,21,25-31 The need to achieve seal at or proximal to zone 2 is common and necessary in upwards of 40% of patients treated for descending thoracic aneurysms. 20 In our series, proximal seal was achieved at or proximal to zone 2 in 60% of the patients; 40% in zone 2 and 20% in zone 0 or zone 1. This highlights the need for even more complex branched thoracic endografts to preserve flow to aortic branch vessels as these endovascular therapies continue to extend proximally into the aortic arch.
LSA revascularization during TEVAR remains controversial since the consequences of coverage remain uncertain. The indications for revascularization of the LSA are not fully defined. To aid in decision making, The Society for Vascular Surgery (SVS) published a clinical practice guidelines suggesting routine LSA revascularization for elective TEVAR and strongly recommending revascularization in cases where coverage would lead to ischemia of a critical organ, such as in a patient with a left internal mammary artery (LIMA) coronary bypass graft. 22 The committee of experts who wrote the practice guideline pointed out, however, that that their recommendations were based on low-quality evidence. Prior to writing the guidelines, the committee commissioned a systematic review and meta-analysis which found that LSA coverage without revascularization was associated only with an increased risk of arm ischemia and vertebrobasilar ischemia, and that there were no statistically significant increases in the risk of spinal cord ischemia, anterior circulation stroke, or death. 32 A Cochrane review concluded: “It is not possible to draw conclusions with regard to the optimal management of LSA coverage in TEVAR.” 23 A number of reviews on the need for LSA revascularization yield conflicting information possibly due to the retrospective nature of the studies where an unclear number of patients were revascularized selectively.23,32-35
Despite the lack of quality evidence many providers still routinely revascularize the LSA; others selectively revascularize for symptoms of arm ischemia, presence of a LIMA bypass, or vertebrobasilar insufficiency. However, surgical revascularization of the LSA with bypass or transposition has been associated with complications in as many as 15% including chyle leak, phrenic nerve paralysis and peripheral nerve palsies.36-38 Early and late graft occlusion has also been reported.38,39 This has led device manufacturers to design and study devices which can be placed in a single stage which both cover the aortic pathology and maintain LSA patency.20,21
Initial results of 2 individual single branched systems have been described. Roselli et al 20 reported results in 9 patients using the Valiant Mona LSA Thoracic Stent Graft System (Medtronic) in the treatment of descending thoracic aneurysms. Technical success was achieved in all patients with the absence of an endoleak noted at the conclusion of the procedure. Four patient has minor non-disabling strokes within 30 days attributed to arch and carotid manipulation. No patients required reintervention or developed arm ischemia during follow up. Dake et al 21 reported the results for the prospective multicenter trial of the Gore Thoracic Branch Endoprosthesis (WL Gore) which enrolled 84 patients. Acute technical success was achieved in 77 patients (92%). There were 3 procedure related strokes and 2 patients suffered complications from spinal cord ischemia. At 1 year there were 8 endoleaks, 1 aneurysm increased in size, and 4 patients died from non-aortic cause.
To determine the clinical need for the next generation device, we studied our patients who underwent TEVAR with proximal fixation in zone 2. We examined the angiograms and CTA scans from 52 patients to determine the value and applicability of such a device. In our analysis, only 38.5% of patients met the anatomic inclusion/exclusion criteria. We found that patients treated for blunt thoracic aortic injury rarely met the anatomic criteria due to smaller proximal aortic diameters and tight clustering of the aortic branch vessels. By excluding BTAI patients, the proportion of patients meeting criteria increased to 45%. Overall, patients who met criteria tended to have larger average aortic diameters at the proximal landing zone and longer distances between the great vessels and between the LCCA and the disease process.
Further subgroup analysis found that TEVAR procedures for aneurysm or PAU met anatomic criteria twice as often as patients treated for dissection. The increased rate of ineligibility in the dissection cohort can be attributed to inadequate lengths from the intimal tear to LSA and LCCA. In half of the dissection patients, the intimal flap extended to or proximal to the LSA which was an anatomic exclusion criteria. Additionally, 60% of these patients had an inadequate distance from the LCCA to the start of the aortic disease.
Patients with BTAI failed due to smaller proximal aortic diameters and crowded aortic arches. In our series, these injuries tended to occur in younger patients. In this younger group of patients, otherwise normal native aortic anatomy precludes them from treatment with these new technologies. Extending their applicability by modifying these devices for smaller aortic diameters is likely unwarranted, as the tight arch vessel anatomy would still preclude treatment with such a device.
Another study found similar anatomic eligibility in patients treated for type B dissection. A single institution analysis reported on the anatomic suitability for the Gore Thoracic Branch Endoprosthesis in patients with complicated type B dissection treated with TEVAR into zone 2. 40 Only 16 of 57 (28%) patients met the anatomic eligibility criteria for the device. Patients failed to meet criteria primarily due to insufficient length between the aortic branches.
Modifications that would increase the applicability of these devices to allow for treatment of aortic dissection would require more relaxed length constraints. In patients with acute dissection treated for malperfusion, the goal of treatment is coverage of the proximal entry tear and repressurization of the true lumen. In this situation, a shorter and potentially less secure proximal seal zone might yield an acceptable clinical outcome. If these criteria were changed, potentially 3 of the previously excluded patients who narrowly missed inclusion in our series would have been able to be treated. Of these 3, one failed due to both a LCCA to LSA distance of 8 mm (rather than 10 mm) and a LCCA to aortic dissection distance of 19 mm (rather than 20 mm), and 2 failed due to LCCA to aortic dissection distance of 18 mm and 16 mm. Such modifications to the inclusion criteria would need to be investigated to determine outcome.
Recently, structural failures of the Valiant Navion thoracic stent graft were identified in the Valiant Evo United States (US) and international clinical trial. 41 Core laboratory evaluation revealed stent structural failure in 11 of 83 patients available for study between 1-4 years after implantation. These findings led to a voluntary global recall of this device and ongoing evaluation of the graft by the manufacturer. Therefore, the fate of this proposed single branch endograft remains unclear. Despite this, the anatomic requirements which will lead to successful implantation are similar among the grafts such that this analysis may have broader applicability.
The chief limitation of this study is the relatively small sample of patients examined. Furthermore, these patients were treated for varying indications leading to even smaller sub-groups for comparison. A larger sample size might reveal a different outcome. The CT angiograms were reviewed internally and were not subject to core lab analysis. These patients were collected from a large academic referral center and may reflect more complex pathology as evidenced by the fact that only 40% of TEVAR patients achieved seal at or distal to zone 3.
Conclusion
Forty-five percent of patients with non-traumatic thoracic aortic pathology who require TEVAR seal extending into Zone 2 met the anatomic criteria for this novel SBTE. This device may offer the ability to provide flow to the LSA when sealing in zone 2 without the need for adjuvant revascularization procedures. Patients with degenerative and saccular aneurysms more often met the IFU compared to those with acute dissection. Patients who present with blunt thoracic aortic injury would rarely be a candidate for such a device due to both small aortic diameter and clustering of the supra-aortic branches. The main anatomic constraints for this device were an inadequate distance from the LCCA to the LSA takeoff and from the LCCA to the start of the aortic disease process.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors Note
Presented at the Plenary Session, 44th Annual Meeting of the Midwestern Vascular Surgical Society, 2020.