
Abstract
Disruption in the non-anastomotic section of an axillofemoral bypass is a rare occurrence. In this report, we consider a patient who presented with a pseudoaneurysm in the non-anastomotic section of his axillofemoral bypass due to blunt trauma to the chest after a fall. Clinical presentation, management, treatment, and complications related to our case are discussed.
Keywords
Introduction
The axillofemoral bypass was first described in 1963 by Blaisdell and Hall, used for the revascularization of ischemic extremities after the excision of an infected aortic graft. 1 Placement of a graft, traditionally done using a Dacron or polytetrafluorethylene (PTFE) prosthesis, is a surgical procedure indicated for vascular insufficiency of the lower extremity secondary to significant aortic or bilateral iliac occlusion. It is a useful option in the setting of patients with contraindications to vascular reconstruction or endovascular procedures, high-risk comorbidities, and limited life expectancy.2,3 The most common complications of an axillofemoral bypass are thrombosis and infection,4,5 whereas disruption in the non-anastomotic section of an axillofemoral bypass is rare. Confirmation of the axillofemoral bypass rupture can be made through duplex ultrasound, computed tomography (CT) with contrast, or magnetic resonance angiography (MRA). Treatment involves resection of the affected area and placement of a new prosthesis or endovascular repair with a covered stent. In this report, we present a case of non-anastomotic axillofemoral bypass disruption after blunt trauma that was treated by an endovascular approach. The patient consented to the publication of the case and associated images.
Case Presentation
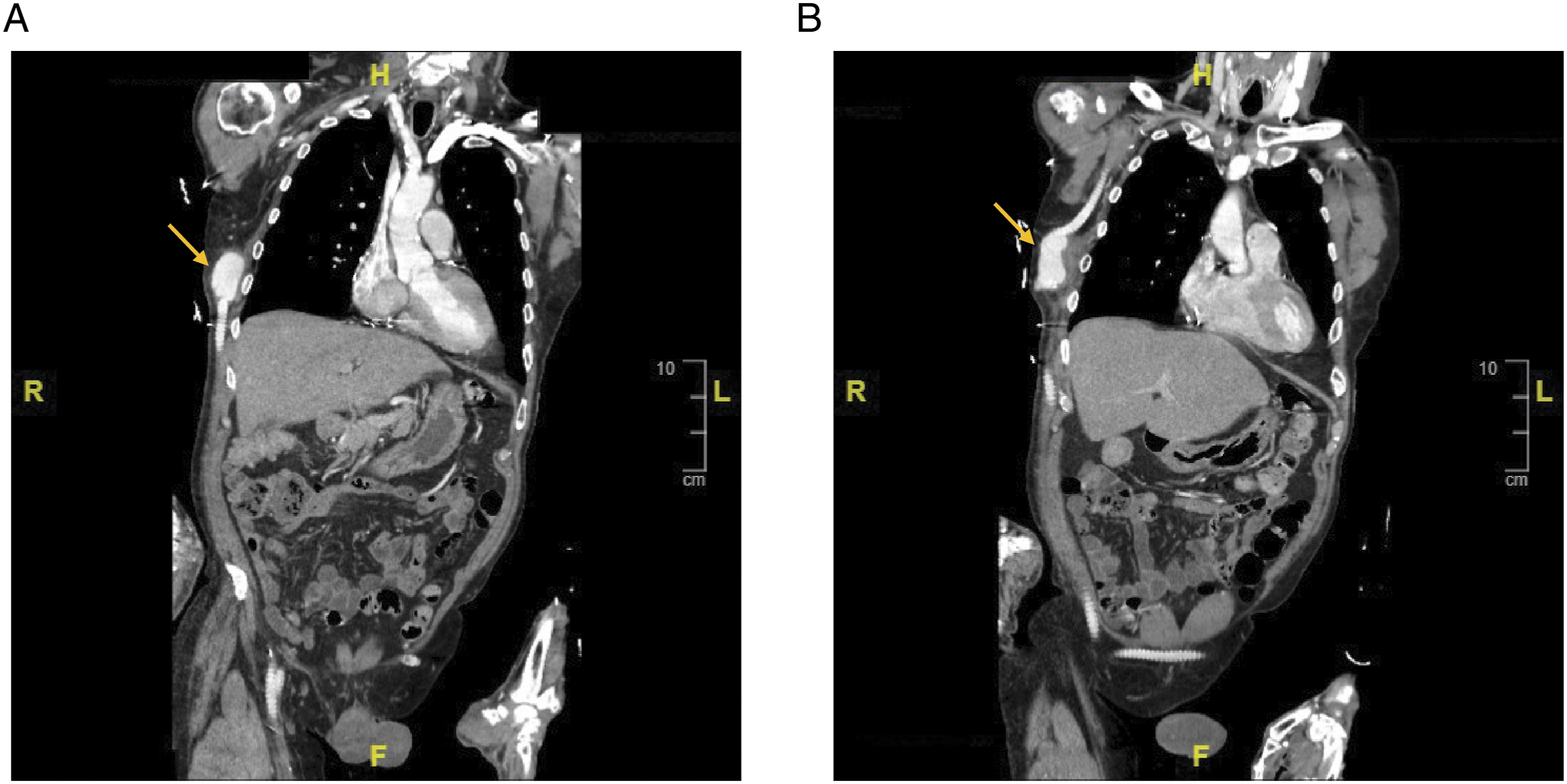
A 70-year-old male with history of stroke, hypertension, coronary artery disease, chronic kidney disease, and diabetes who underwent right axillobifemoral bypass one and a half years prior presented to the emergency department with increasing right lateral chest wall ecchymosis and pain after sustaining multiple falls. He was found to have a pulsatile mass on the lateral chest wall. Femoral pulses were palpable with monophasic signals detected at the dorsal pedal and posterior tibial arteries on Doppler bilaterally. According to his family, pain and swelling of the right chest wall had been evolving over several days after one of the falls. Computed tomography angiography (CTA) showed disruption of the placed 7-mm Propaten axillofemoral graft in the mid lateral chest wall approximately 20 cm from the axillary artery anastomosis (Figures 1 and 2). The pseudoaneurysm was approximately 5 cm in size. The remaining portion of the axillobifemoral bypass appeared patent. Based on concern for ongoing expansion of the pseudoaneurysm with possible rupture, the patient was consented for repair of the axillofemoral bypass graft pseudoaneurysm. Treatment modalities including open surgical repair and endovascular approaches were discussed with the family, and a consensus was reached to treat primarily through an endovascular approach given the patient’s comorbidities. Computed tomography angiography revealed a pseudoaneurysm (yellow arrow) in the right lateral chest wall. Image is in axial view. Computed tomography angiography showed a pseudoaneurysm (yellow arrow) disrupting the otherwise intact axillofemoral graft (A, B) in the right mid lateral chest wall. Images are in coronal view.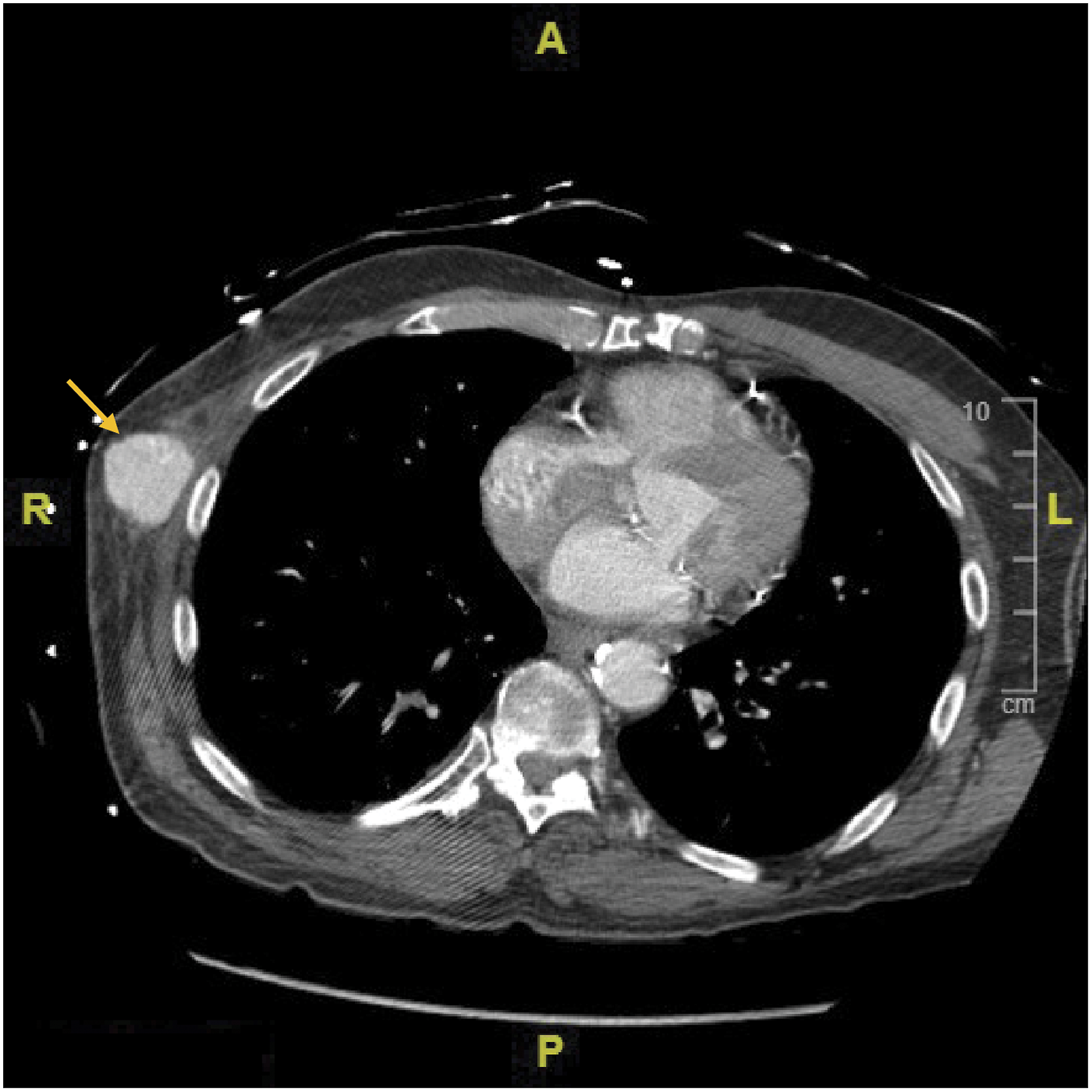
Surgical repair involved a longitudinal incision made over the right axillofemoral graft in the right lateral lower abdomen below the costal margin. Upon exposure of the graft in a subfascial plane, it was mobilized over a length of approximately 5 cm and double looped with vessel loops proximally and distally. A CV6 Gore-Tex mattress suture was placed, and the graft was punctured through the mattress suture with a micro puncture needle. A micro puncture sheath was inserted and exchanged for an 8-French sheath.
A retrograde angiogram of the right axillofemoral graft showed the pseudoaneurysm in the mid lateral chest (Figure 3A). A .035 angled Glide wire was advanced through the graft in a retrograde fashion. It traversed across the pseudoaneurysm and entered into the more proximal component of the axillofemoral graft. A Berenstein catheter was advanced. Contrast injection in the Berenstein catheter proximal to the pseudoaneurysm showed proper intraluminal positioning. A Rosen wire was placed. Retrograde angiogram showed disruption (A) of the axillofemoral graft (yellow arrow) that was repaired by placement of a stent (B) in the right mid lateral chest wall (yellow arrow). Patent flow was confirmed proximal (C) and distal (D) to the site of repair. Images are in coronal view.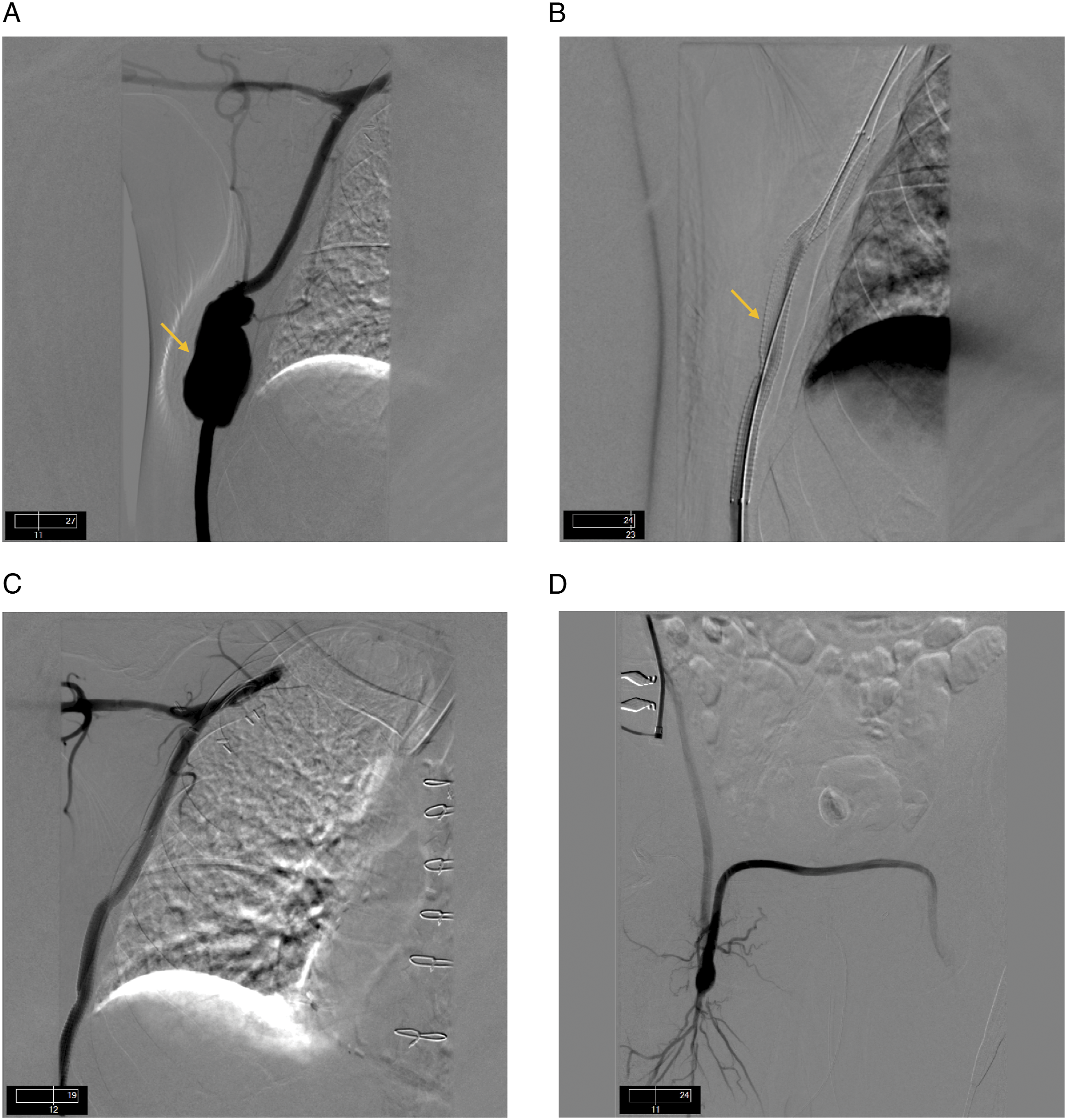
The graft component appeared to have separated approximately 5 cm with some angulation of the disrupted ends. A decision was made to bridge the pseudoaneurysm with an 8 mm × 15 cm Gore Viabahn stent. This was advanced and centered across the pseudoaneurysm. There was an approximate 4 to 5 cm overlap both proximally and distally. The stent graft was deployed and post dilated with an 8 × 40 balloon proximally and distally (Figure 3B). Subsequent retrograde and antegrade angiography showed a widely patent stent graph with no extravasation into the pseudoaneurysm (Figure 3C and D).
The 8-French sheath was removed, and the previously placed mattress suture was tied down. Two additional CV6 Gore-Tex mattress sutures were placed to achieve good hemostasis. Strong Doppler signals were detected over the graft and femoral arteries were palpable bilaterally.
The patient had an uncomplicated post-operative hospital course. His home aspirin and Plavix were resumed, and he was discharged on post-operative day 3. A follow-up arterial duplex in 3 months showed a patent bypass without any concerns. A computed tomography pulmonary embolus (CTPE) protocol obtained at the 5 month mark while he was hospitalized for other reasons showed a patent bypass with the stent in good position and resolution of the pseudoaneurysm.
Discussion
Axillofemoral bypass is a well-known surgical procedure. It is an extra anatomic bypass mainly indicated for symptomatic aortoiliac occlusive disease in patients who are not endovascular candidates and are at high risk for direct aortic repair. It is also considered in infected native aorta, prosthetic grafts, or aortoenteric fistulae. Axillofemoral bypass can be a good option for patients with critical ischemia of lower extremities with a “hostile abdomen” such as in cases of multiple previous abdominal surgeries, active intra-abdominal infection, or presence of intestinal or urinary stomas. When reserved for high-risk patients with limited life expectancy, the patency and limb salvage results are comparable between aortofemoral vs axillofemoral procedures. 6 5 year patency is up to 70% for axillofemoral bypass. 7
Complications associated with axillofemoral bypass include upper extremity thromboembolism secondary to graft thrombosis, seroma formation, graft infection, and disruption of the anastomosis site. 8 Anastomotic disruption, commonly known as the “Pull-out syndrome”, occurs at the axillary artery anastomosis site typically in the early post-operative period. It is attributed to technical issues, infection, and mechanical stress. Disruption is often preceded by exertion around the shoulder joint. It is associated with sudden onset of pain, swelling, and paresthesia in the upper arm secondary to the development of a hematoma or pseudoaneurysm. 9
Disruption of an axillofemoral bypass graft at a non-anastomotic site is an uncommon complication. In a nonsystematic review of the PubMed/MEDLINE database, an analysis of 14 cases from 1963 - 2016 revealed that disruption in the non-anastomotic section of an axillofemoral bypass is a very rare complication that is more frequently observed in unifemoral bypass (9 cases), ringed PTFE grafts (only 3 cases involved a Dacron prosthesis), and blunt trauma (no cases with open trauma), with 86% of cases involving the level of the costal rim, particularly on the left side (8 cases vs 5 cases involving the right side). 4 The most common cause of graft disruption is acute contusion-related trauma due to its subcutaneous location with symptoms of a false aneurysm. 4 In our case, we believe that the rings of the PTFE graft could have a role in this complication by creating a tear in the body of the graft after blunt trauma. The patient’s body habitus could have also played a role – as our patient had a low body mass index (BMI), it is possible that if he had more soft tissue coverage over his PTFE graft, this complication would not have happened.
The use of a particular graft material (Dacron or PTFE) has not been shown to have significant difference in patency outcomes or complications when used for aortofemoral bypass. 10 However, no studies are available which compare the two materials in terms of graft disruption due to trauma.
Multiple different approaches for the repair of the disruption or pseudoaneurysm have been attempted in previously described cases. These include partial resection with interposition graft repair,10-14 explantation of aortofemoral graft with femorofemoral bypass, 15 as well as direct suture repair after pseudoaneurysm resection. Recently, endovascular repair with covered stents has been described by Grochow et al and Mousa et al.16,17 In the case described by Grochow et al, a Bard (Tempe, AZ) Fluency self-expanding flexible stent was used. 16 Mousa et al described utilizing intravascular ultrasound (IVUS) to calibrate the size of the graft proximal and distal to disruption, the size of pathology, cross sectional gain and evaluation of stent expansion; in this case, a Gore Viabahn stent was used. 17 We also chose to place a Gore Viabhan stent, which is a flexible self-expanding stent excellent for use in areas that can be subjected to compression. Reports of both open and endovascular repair have documented good outcomes in the short term with little information regarding long term results.4,17 An endovascular approach was chosen in the case of our patient given his multiple cardiovascular risk factors and comorbidities.
Conclusion
Disruption in the non-anastomotic region of an axillofemoral bypass is a rare but known event with potentially devastating consequences. Different repair techniques have been described with surgical open repair as a prominent option for the treatment and management of non-anastomotic axillofemoral bypass disruptions. However, endovascular repair with covered stenting remains a viable option, especially in patients who are at high risk due to medical comorbidities. In the case of our patient, the disruption in the non-anastomotic region of our patient’s axillofemoral bypass after blunt trauma was successfully treated via endovascular approach.
Footnotes
Author Contributions
Concept – HS, MS; Design – YJL, HS; Supervision – HS, MS; Literature Review – HS, YJL; Writing – HS, YJL; Critical Review – YJL, HS, MS, MIE.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent:
Written informed consent was obtained from the patient.