
Abstract
Objective
Endovascular aortic aneurysm repair (EVAR) has been established as a standard treatment option for intact abdominal aortic aneurysm (iAAA) and gained importance due to a lower perioperative mortality than open repair (OAR). However, whether this survival advantage can be maintained or if OAR is beneficial in terms of long-term complications and reinterventions remains questionable.
Design
In this retrospective cohort study data from patients undergoing elective EVAR or OAR for iAAAs in the years 2010-2016 was analyzed. The patients were followed through 2018.
Methods
In the propensity score matched cohorts the perioperative and long-term outcomes of the patients were assessed. We identified 20 683 patients undergoing elective iAAA repair (76.4% EVAR). The propensity matched cohorts included 4886 pairs of patients.
Results
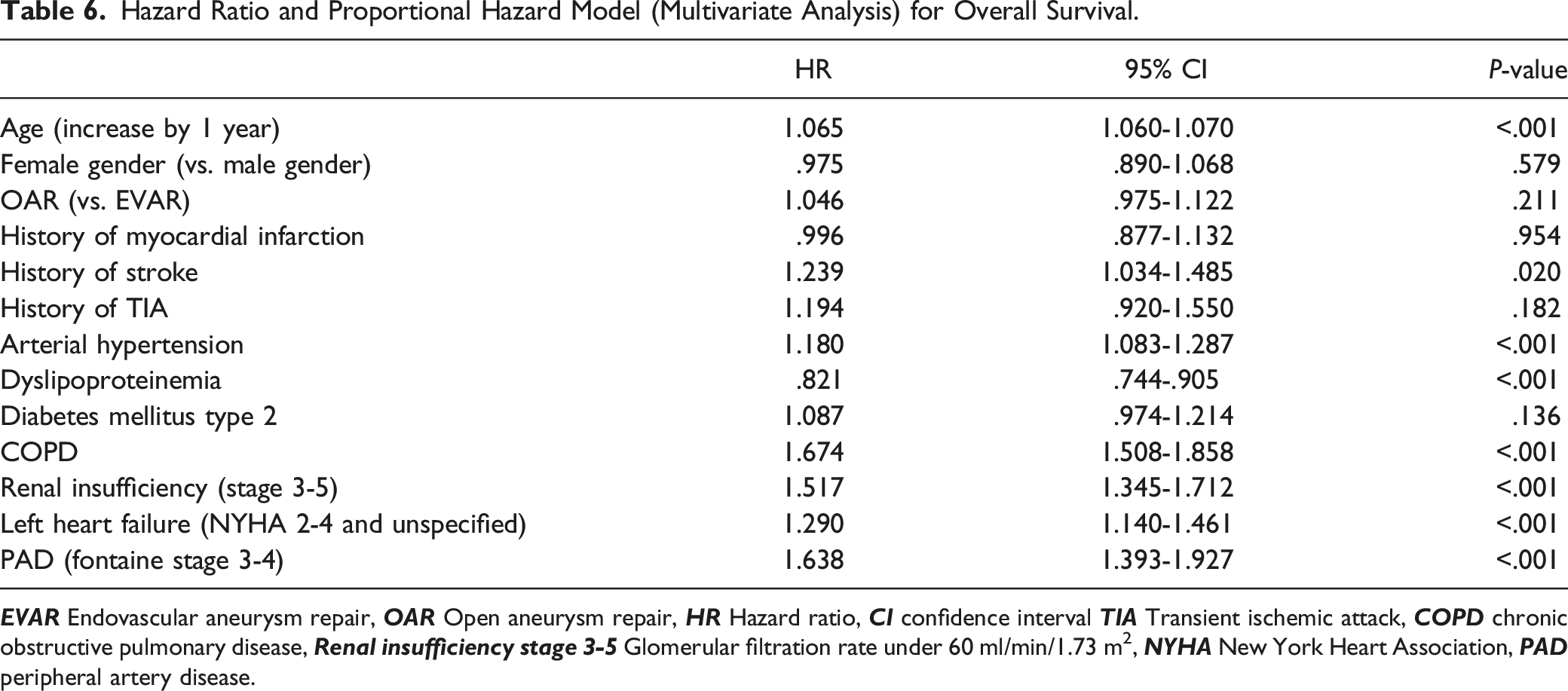
The perioperative mortality was 1.9% for EVAR and 5.9% for OAR (P = <.001). The perioperative mortality was mainly influenced by patients age (Odds-Ratio (OR):1.073, confidence interval (CI):1.058-1.088, P ≤ .001) and OAR (OR:3.242, CI:2.552-4.119, P ≤ .001). The early survival benefit after endovascular repair persisted for approximately 3 years (estimated survival EVAR 82.3%, OAR 80.9%, P = .021). After that time the estimated survival curves were similar. After 9 years the estimated survival was 51.2% after EVAR as compared to 52.8% after OAR (P = .102). The operation method didn’t influence long-term survival significantly (Hazard-Ratio (HR): 1.046, CI: .975-1.122, P = .211). The vascular reintervention rate was 17.4% in the EVAR cohort and 7.1% in the OAR cohort (P ≤ .001).
Conclusion
EVAR has a significantly lower perioperative mortality than OAR, a survival benefit that lasts up to 3 years after intervention. Thereafter, no significant difference in survival was observed between EVAR and OAR. The decision between EVAR or OAR may depend on patient preference, surgeons’ experience, and the institutions’ ability to handle complications.
Introduction
The superiority of endovascular abdominal aortic aneurysm repair (EVAR) in comparison to open aneurysm repair (OAR) with respect to the 30-day-survival-rate and perioperative complications is generally accepted, however, results on long-term survival are not consistent. In EVAR trial 1 a lower mortality after OAR than after EVAR in the 8-year follow-up period was observed. 1 In contrast, in the Over trial, long-term overall survival was similar among patients who underwent endovascular repair compared to patients who underwent open surgery. 2 Bulder et al 3 detected no difference in long-term survival between EVAR and OAR up to 10 years after surgery, whereas Li et al 4 found a higher mortality with EVAR after 5 to 9 years. Furthermore, they found a higher reintervention rate and a higher secondary rupture rate with EVAR. Many confounding factors make it difficult to compare the 2 procedures in routine clinical practice. To make the 2 procedures more comparable, Schermerhorn et al 5 analyzed perioperative and long-term survival, reinterventions, and complications after EVAR and OAR in Medicare beneficiaries in propensity score matched cohorts. In their study, the endovascular repair was associated with a significant early survival benefit compared with open repair, which gradually decreased over time. A significantly higher rate of late rupture was observed after endovascular repair than after open repair. Whether similar results can be observed in Germany in a patient population that is treated with EVAR in a significantly later period and with increasing experience with EVAR, will be examined in this study. Therefore, the perioperative complications and long-term survival after elective open (OAR) and endovascular (EVAR) repair of intact abdominal aortic aneurysms (iAAA) were analyzed using data from the largest German health insurance company, which serves about 1 third of the population (approx. 27 mill people).
Methods
In this retrospective study, anonymized patient data of “AOK-Die Gesundheitskasse” registry (largest statutory health insurance company in Germany) was analyzed. Since health insurance data was analyzed, the entire medical history of every patient was considered. Therefore, this study was not limited to 1 hospital group or medical department. Patients’ medical information was coded using the International Classification of Diseases, 10th Revision (ICD-10) and Operations and Procedures Codes (OPS). Data from all patients who underwent endovascular (OPS code: 5-38a.1) (n = 15 792) or open repair (OPS codes: 5-384.7) (n = 4891) for an iAAA (ICD code: I71.4 abdominal aorta aneurysm, without mention of rupture) between Jan. 1, 2010, and Dec. 31, 2016, were included in the study. Comorbidities, perioperative complications, and complications in the follow-up were analyzed using the documented ICD and OPS codes. All patients were followed until December 31, 2018. The mean follow-up time of the patient cohort was 79 months (minimum follow-up: 0 months, maximum follow-up 107 months). Patients’ death but not the cause of death was reported.
Propensity Score Matching
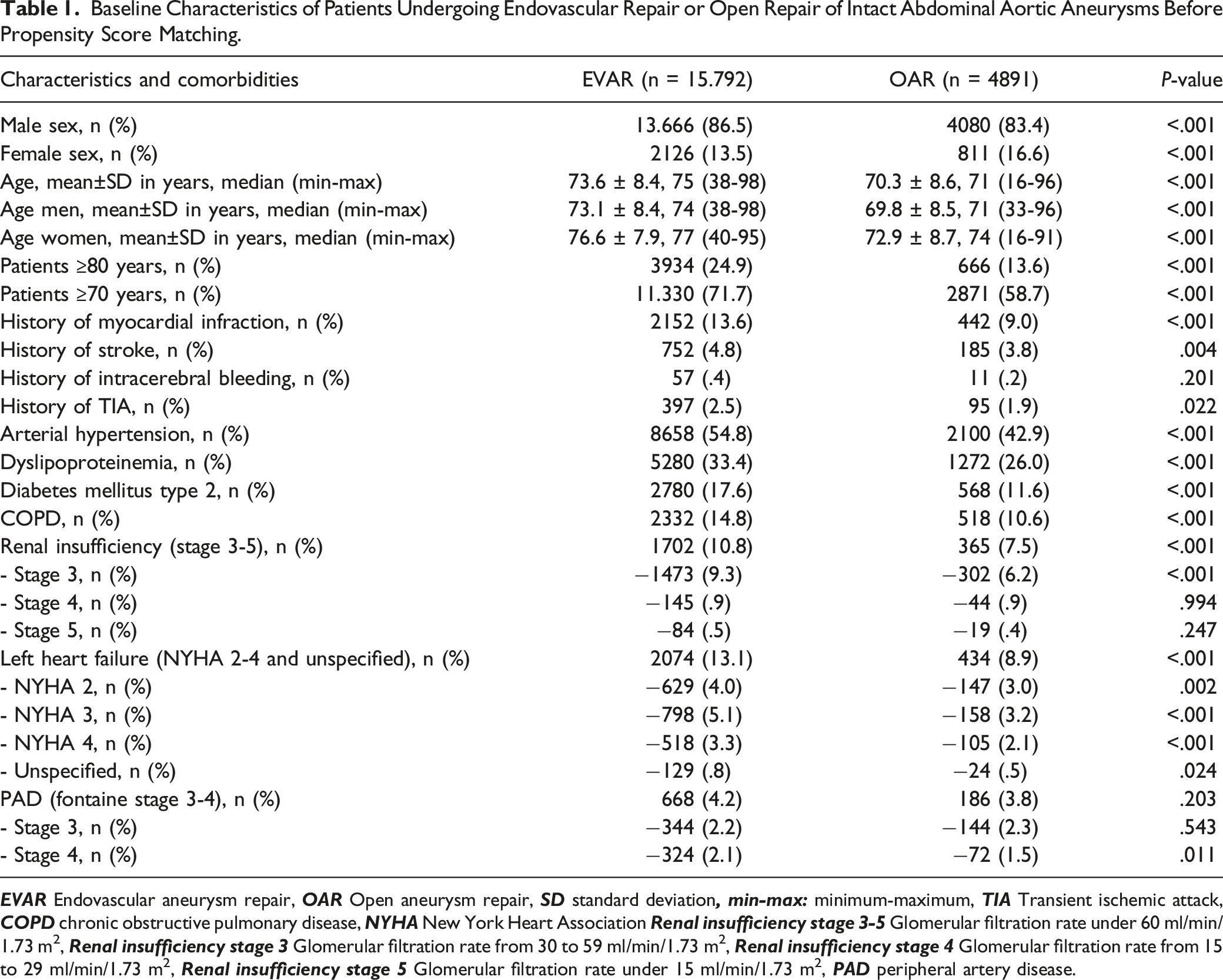
Baseline Characteristics of Patients Undergoing Endovascular Repair or Open Repair of Intact Abdominal Aortic Aneurysms Before Propensity Score Matching.
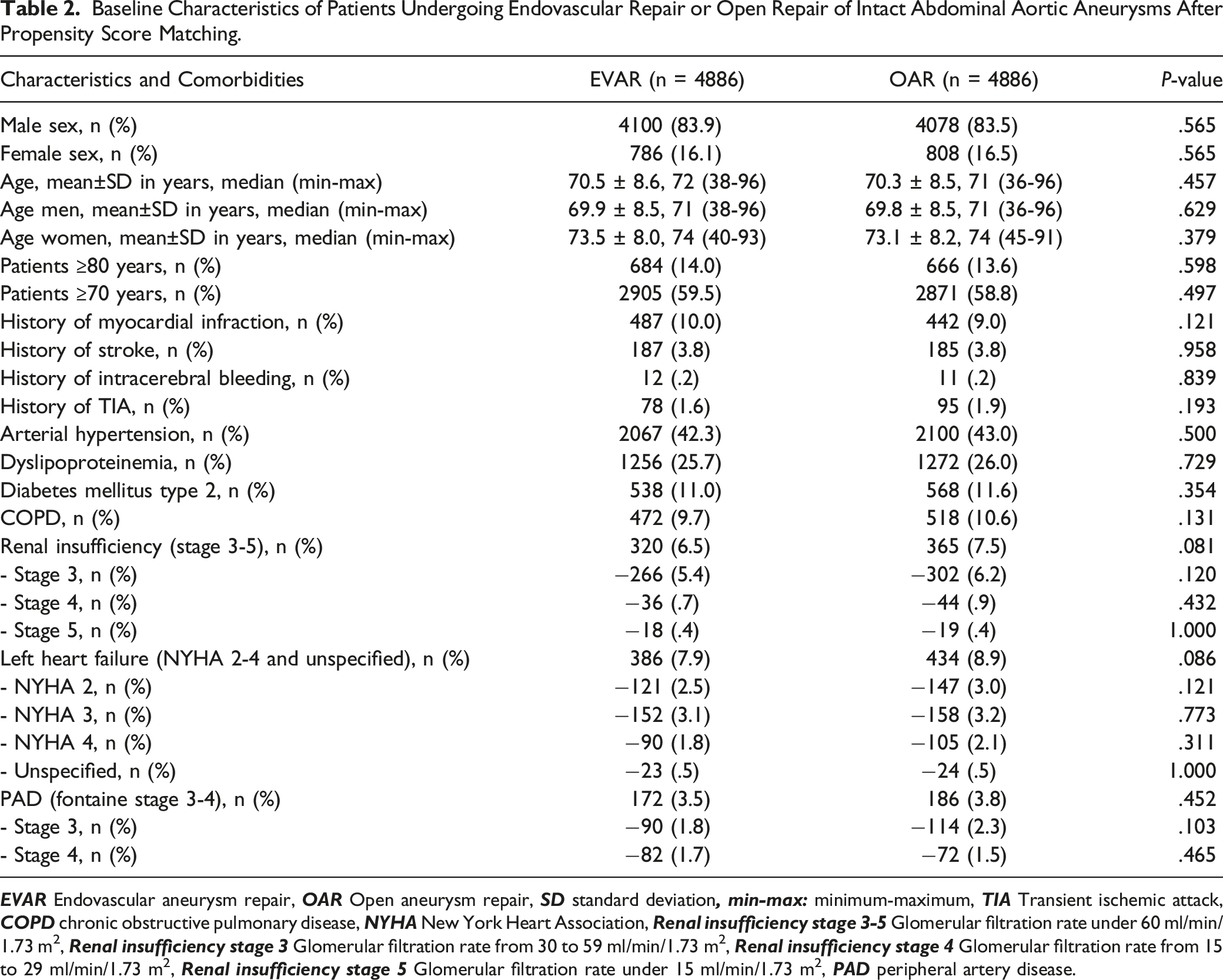
Baseline Characteristics of Patients Undergoing Endovascular Repair or Open Repair of Intact Abdominal Aortic Aneurysms After Propensity Score Matching.
Statistical Analysis
After using R for the propensity score matching the rest of the analysis was completed with SPSS 27 (IBM Deutschland GmbH, Ehningen, Deutschland). This study was designed according to the intention-to-treat principle. To analyze if there were significant differences between both operation methods Chi-square-tests were used for non-metric variables. The P-value corresponded to the significance of the Fisher’s exact test. For metric variables a Mann-Whitney-U-test was performed. Those tests were also performed to ensure that there were no significant differences between the operations methods regarding the baseline patients’ characteristic after the propensity score matching. To analyze the effect of patients’ characteristics and comorbidities on perioperative mortality a univariable binary logistic regression was performed. All statistically significant variables (P < .05) from the univariable model were included in a multivariable analysis. To estimate overall survival Kaplan-Meier tables were created. Comparisons were made using the log-rank test. We also performed separate survival analyses for 3, 5, and 9 years of follow-up. All complications and aneurysm-related reinterventions, which occurred during the follow-up period were also estimated using the Kaplan-Meier life-table method and compared with the log-rank test. Complications or reinterventions that occurred in the perioperative period were not integrated in this analysis. Univariable Cox proportional model was performed prior to a multivariable Cox proportional model to evaluate whether comorbidities, age and type of surgery had an impact on overall survival. All parameters, which had a statistically significant impact on survival in the univariable analysis (P < .05) were tested in the multivariable analysis. Log-rank tests were performed to test for significance. P-values of less than .05 were considered statistically significant.
Results
Patients
The study population consisted of a total of 20 683 patients. 15 792 (76.4%) underwent EVAR and 4891 (23.6%) OAR (Table 1). 17 746 (85.8%) were men, and 2937 (14.2%) were women. EVAR patients were significantly older with a mean age of 73.6 years (SD: 8.4) than OAR patients with a mean age of 70.3 years (SD:8.6) (P ≤ .001). EVAR patients had significantly more comorbidities. 2152 (13.6%) EVAR patients suffered myocardial infarction before surgery compared to 442 (9.0%) OAR patients (P ≤ .001). EVAR patients were also more likely to have chronic obstructive pulmonary disease (COPD) than OAR patients (EVAR: 14.8%; OAR: 10.6%; P ≤ .001)
The propensity matched cohort included 4886 pairs of patients (mean age: 70.4 years SD: 8.5). There were no significant differences in baseline covariates between EVAR and OAR cohorts (Table 2).
Perioperative Outcome
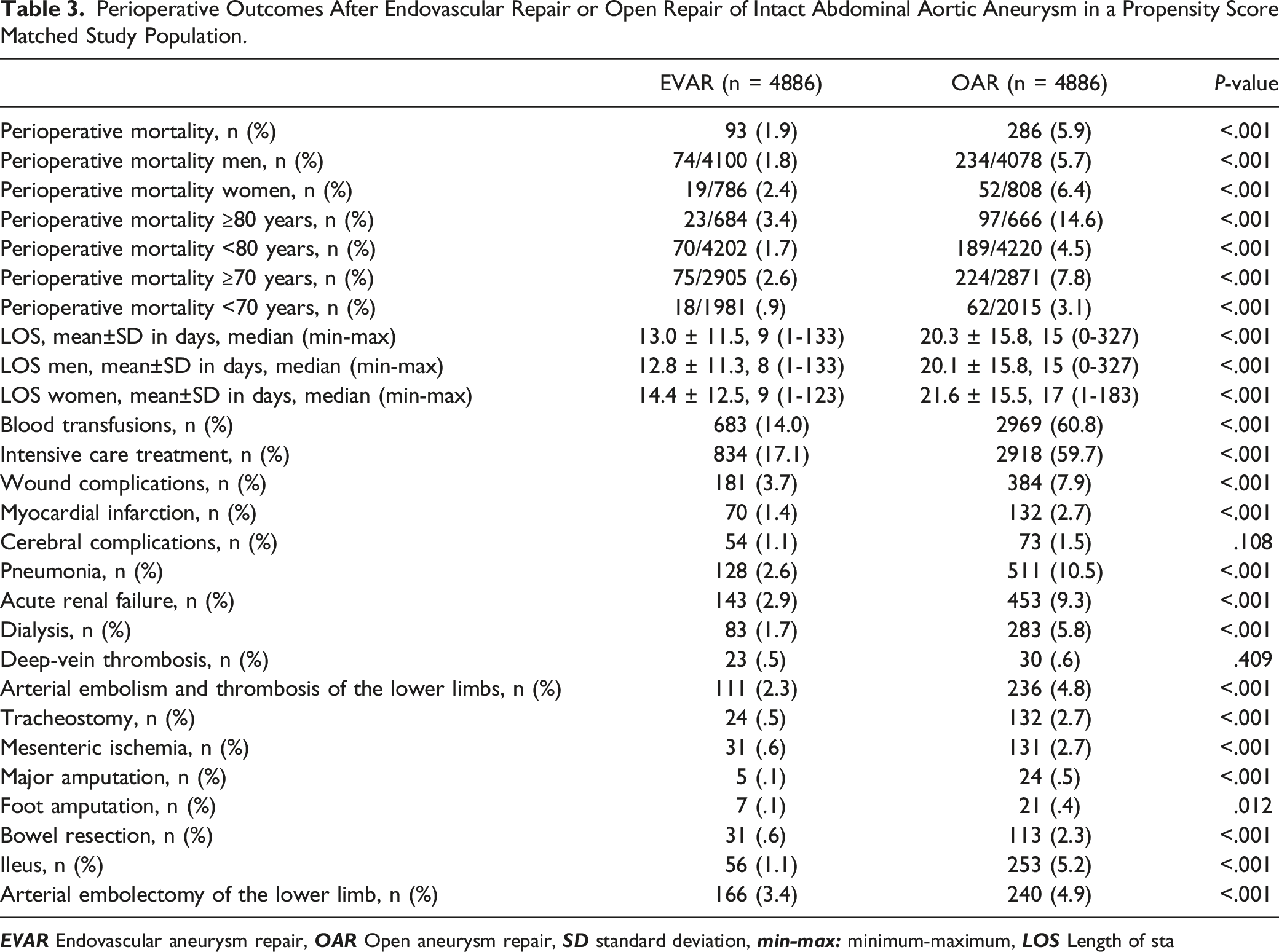
Perioperative Outcomes After Endovascular Repair or Open Repair of Intact Abdominal Aortic Aneurysm in a Propensity Score Matched Study Population.
Long-Term Survival
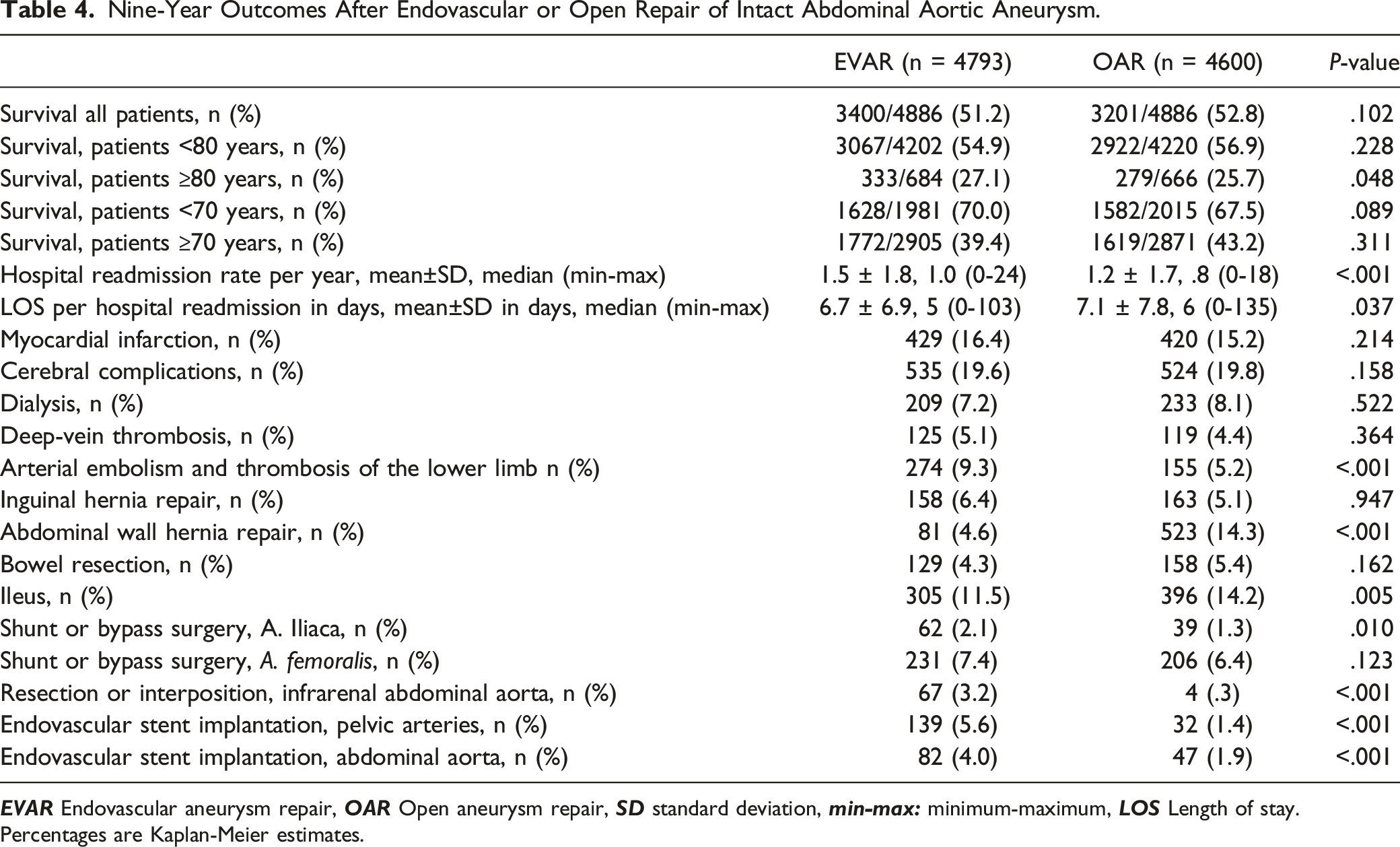
The long-term survival in the 2 cohorts is shown in Figure 1. The early survival benefit after endovascular repair persisted for approximately 3 years (EVAR estimated survival rate 82.3%, OAR 80.9%, P = .021). After that time the estimated survival curves were similar. 71.5% of EVAR patients survived 5 years compared to 70.4% of OAR patients (P = .060). After 9 years estimated survival was 51.2% among patients in the EVAR cohort as compared to 52.8% in the OAR cohort (P = .102). The survival rate depended on patients’ age as demonstrated in Table 4. There was no difference in estimated survival in patients with EVAR and OAR in the analyzed age groups, apart from patients 80 years and older. These patients showed a significantly better estimated survival after EVAR as compared to OAR (27.1% vs 25.7%, P = .048). Survival after endovascular repair or open repair of abdominal aortic aneurysm. Nine-Year Outcomes After Endovascular or Open Repair of Intact Abdominal Aortic Aneurysm. Percentages are Kaplan-Meier estimates.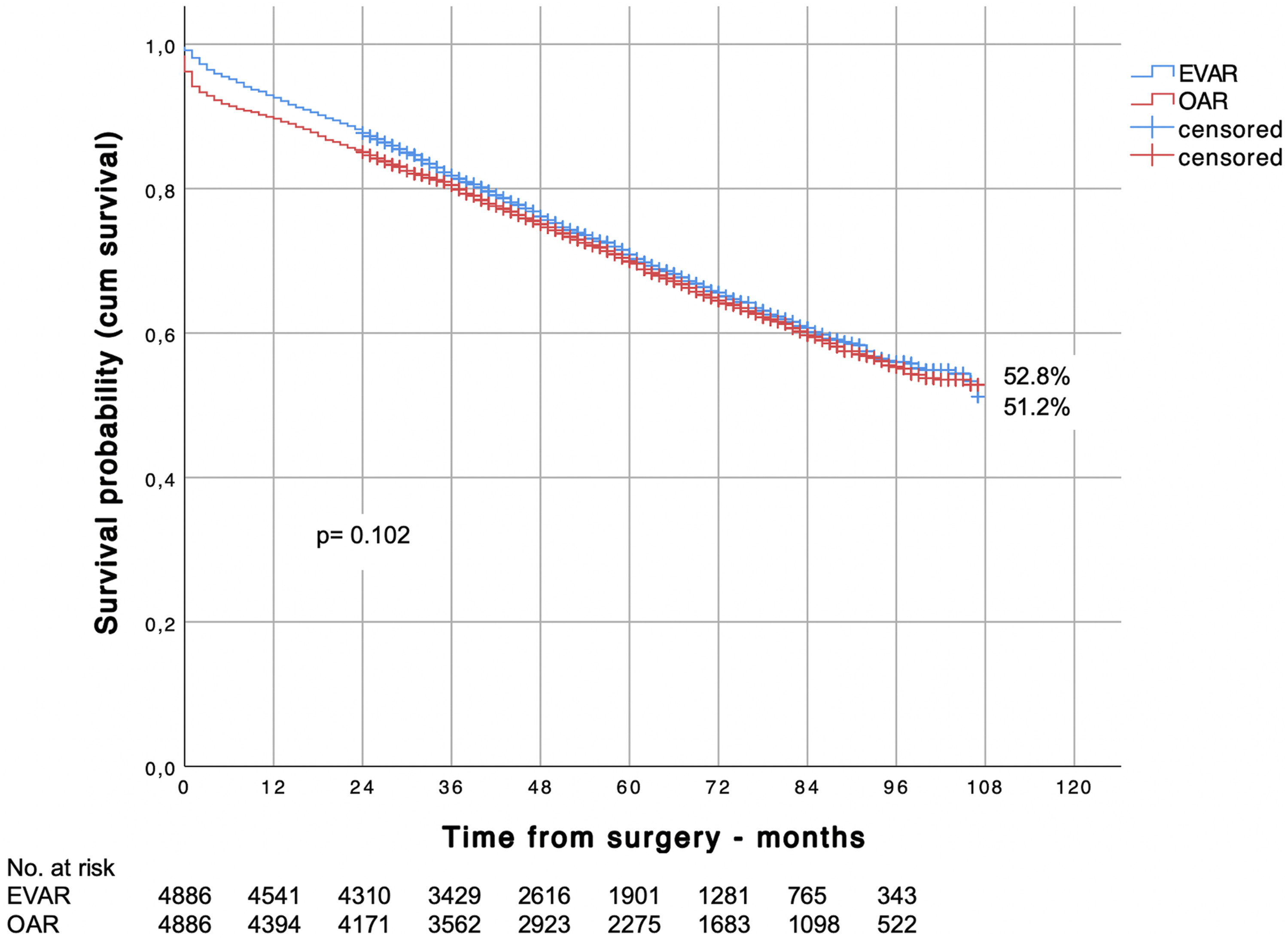
Other Long-Term Outcomes
Hospital readmission rates per year and long-term complication rates in the follow-up period are given in Table 4. Yearly hospital readmissions were more frequently seen with EVAR as compared to OAR (1.5 vs 1.2, P ≤ .001). The length of stay per readmission, however, was longer in the OAR cohort (7.1 days vs 6.7 days, P = .037). Embolism and thrombosis of the lower limb were more often seen in the EVAR cohort (9.3% vs 5.2%, P ≤ .001). In the follow-up, abdominal wall hernia repairs were performed in only 4.6% of EVAR patients but in 14.3% OAR patients (P ≤ .001), ileus occurred in 11.5% of EVAR patients vs 14.2% of OAR patients (P = .005)
The vascular reintervention rate is shown in Figure 2. 17.4% of EVAR patients underwent at least 1 additional vascular reintervention at the end of follow-up compared to only 7.1% of OAR patients (P ≤ .001). Cumulative incidence of vascular reintervention after endovascular repair or open repair of abdominal aortic aneury.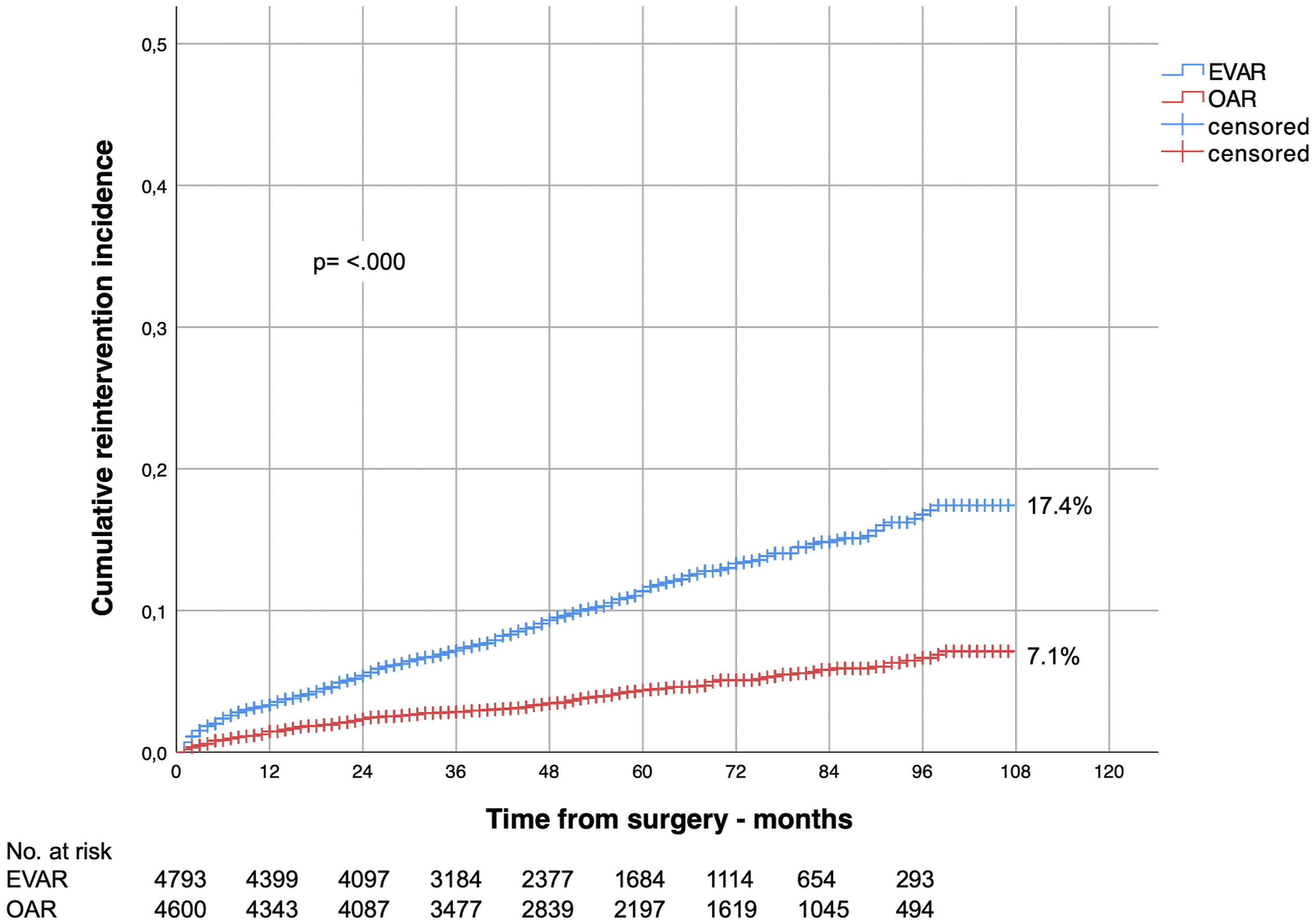
Sensitivity Analysis
Multivariate Binary Logistic Regression Analysis Regarding Perioperativ Mortality.
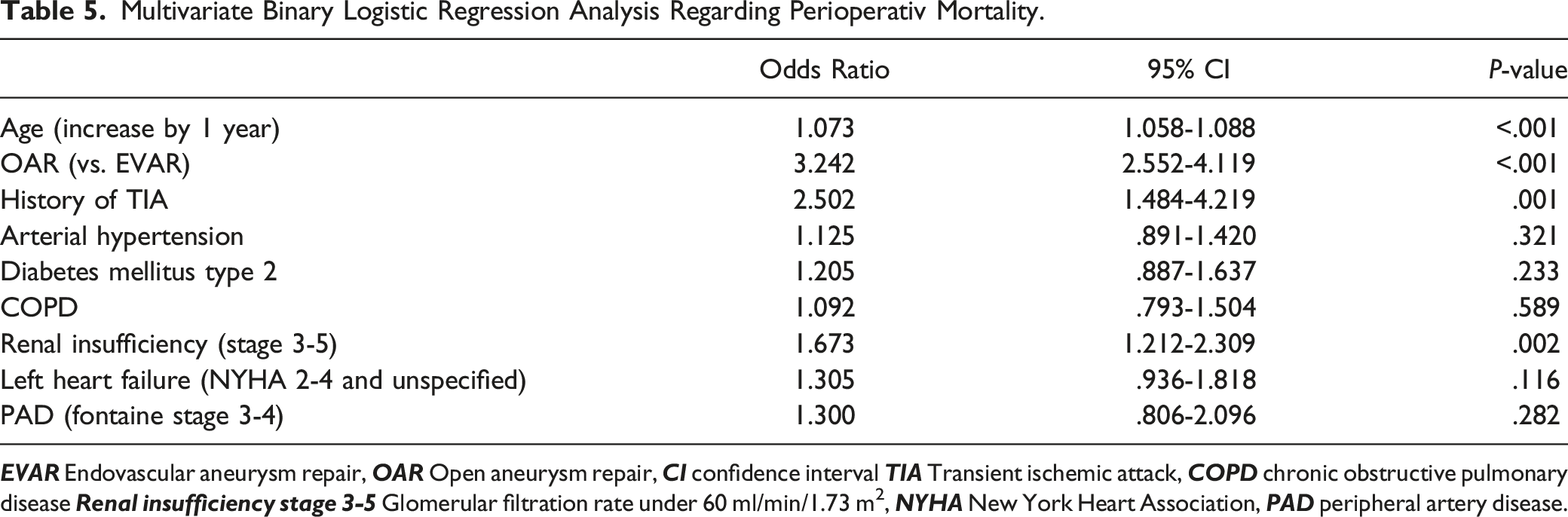
Patient gender was not included in the multivariable binary logistic regression analysis because it had no significant influence on perioperative mortality in the univariable analysis (female gender: OR: 1.191, CI: .915-1.551, P = .194).
Hazard Ratio and Proportional Hazard Model (Multivariate Analysis) for Overall Survival.
Discussion
In this propensity score matched cohort study, perioperative mortality was significantly lower after EVAR as compared to OAR, which resulted in a survival benefit that persisted up to 3 years after surgery. Subsequently, EVAR and OAR did not differ in their survival up to 9 years after surgery. This confirmed the results of the meta-analysis by Bulder et al, 3 who found no difference between EVAR and OAR in long-term survival up to 10 years postoperatively. Schermerhorn et al 5 also found in their matched cohort study only an early survival benefit up to 3 years with endovascular repair compared to open repair. After that time the survival was similar in the 2 groups. These results are also consistent with a retrospective population-based cohort study from Ontario, Canada by Salata et al. 6 They detected 4010 propensity score matched patient pairs among 17 683 patients, who underwent elective AAA surgery. Compared with OAR, EVAR was associated with a higher survival rate up to 1 year after repair and a higher major adverse cardiovascular event–free survival rate up to 4 years after repair. Survival analyses demonstrated no statistically significant differences in long-term survival, reintervention, and secondary rupture for patients who underwent EVAR compared with those who underwent OAR. In this study, endovascular aortic repair was not associated with a difference in long-term survival even during more than 13 years’ maximum follow-up.
The present study is so far the largest cohort study with the longest follow-up reported from Germany after EVAR and OAR. German health insurance data (DAK Gesundheit) was also presented by Behrendt et al 7 They analyzed long-term survival after EVAR (n = 3493) and OAR (n = 1457) in a smaller unmatched cohort. In their study, hospital mortality was 1.2% after EVAR and 5.4% after OAR. Kaplan-Meier analyses of survival after iAAA repair showed that the early benefit in cumulative survival after elective EVAR was reversed at about 1.5 years of follow-up. In the adjusted analyses using Cox proportional hazard models, survival was similar between the EVAR and OAR groups (HR:1.028; CI:0.889- 1.188, P = .708). This data is consistent with the results found in the matched population here (hospital mortality EVAR 1.9%, OAR 5.9%).
Varkevisser et al 8 compared the long-term mortality between EVAR and open abdominal aneurysm repair for patients of different ages. In their study, EVAR in patients younger than 65 was associated with higher long-term all-cause mortality compared with open repair. The overall mortality was balanced between EVAR and open repair in patients aged between 65 and 79 years, and lower after EVAR as compared to OAR in patients aged 80 years. They concluded that a young, healthy patient with low operative risk and a long-life expectancy may be considered for open AAA repair, whereas EVAR remains the preferred treatment for most older AAA patients. Our results are consistent with these findings, patients younger than 70 years (EVAR: 70.0%, OAR: 67.5%, P = .089) and older than 70 years (EVAR: 39.4%, OAR: 43.2%, P = .311) as well as patients younger than 80 years (EVAR: 54.9%, OAR: 56.9%, P = .228) did not significantly differ in their long-term survival with respect to the surgical procedure (EVAR or OAR). Only patients, who were 80 years and older, survived significantly longer after EVAR than after OAR (EVAR: 27.1%, OAR: 25.7% P = .048). Based on that our results favor EVAR for patients of older age. Especially given the high hospital mortality of OAR, the implication must be to offer OAR only in high-volume centers with low hospital mortality, at least for older and high-risk patients. 9 Anyhow, the 5.9% OAR hospital mortality observed here does not meet the standard required by the SVS guidelines, 10 which calls for perioperative mortality of 5% or less.
The long-term survival and cardiovascular morbidity between women and men undergoing elective abdominal aortic aneurysm (AAA) repair at National Health Service hospitals in England was reported by Desai et al 11 Female patients had higher 30-day mortality with both open repair (OR 1.39, CI 1.25-1.56, P < .001) and EVAR (OR 1.57, CI 1.23-2.00, P < .001) compared to men. Women patients had higher 30-day, 1-year, 5-year, and aortic-related mortalities compared with men for both types of AAA repair. O`Donnell et al 12 compared long-term survival, aneurysm-related mortality, and rates of endoleaks and reinterventions between male and female patients in the Endurant Stent Graft Natural Selection Global Postmarket Registry (ENGAGE) using 2:1 propensity score matching. In their study, female patients had long-term outcomes comparable to those of male patients. In our study female sex was not a risk factor, neither for perioperative mortality (univariable analyses female sex: OR: 1.191, CI: .915-1.551, P = .194) nor for long-term outcome (female sex: HR:0.975, CI:0.890-1.068, P = .579). Behrendt et al 13 also concluded that short- or long-term survival and reintervention outcomes were similar in both sexes.
Schermerhorn et al 5 noted a significantly increased risk of rupture with EVAR (5.4%) compared to OAR (1.4%). Similar results are reported by Yei et al. 14 In their analysis of the Society for Vascular Surgery (SVS) Vascular Quality Initiative (VQI) database, regarding a total of 32 760 patients, 2852 patients each with EVAR and OAR were included in a propensity score matched comparison. In their study, endovascular repair was associated with significantly higher rates of long-term rupture and reintervention. We were not able to comment on the long-term aneurysm rupture rate with endovascular and open repair, because the causes of death of the patients were not reported. Nevertheless, in our study the hospital readmission rate per year was also significantly higher after EVAR with 1.5 ± 1.8 than after OAR with 1.2 ± 1.7 (P ≤ .001). In contrast, the hospital stay per readmission was significantly shorter for EVAR (6.7 ± 6.9 days vs 7.1 ± 7.8 days, P = .037). Additionally, we determined vascular reinterventions, they were significantly (P ≤ .001) higher in EVAR patients (17.4%) as compared to OAR patients (7.1%) (Figure 2). However, other reasons for readmission were less frequently seen with EVAR as compared to OAR (ileus: 11.5% vs 14.2%, P = .005; abdominal wall hernia repair 4.6% vs 14.3%, P ≤ .001).
Limitations of this study include potential coding errors. The cause of death was not reported in the given dataset, therefore aneurysm-related deaths could not be specified. The endoleak-rate and aneurysm-rupture rate were not documented.
Furthermore, hospital mortality in patients over 80 years of age seems to be very high with OAR (14.6%). Whether the AOK data represent the overall standard quality of open aortic aneurysm repair in Germany is unknown. The levels of the treating hospitals and the percentage of patients treated in high- and low-volume hospitals were unknown.
Information on aneurysm anatomy (juxtarenal/infrarenal) and aneurysm size is not reported in this study
Conclusion
Summarizing these results, the in-hospital mortality was significantly lower after EVAR than after OAR, which resulted in a survival benefit that persisted up to 3 years after surgery. Nevertheless, at a long-term follow-up of 9 years, there were no significant differences between OAR and EVAR in terms of patient survival. Thus, we suggest that the decision between EVAR and OAR should depend on the patient’s preference and given the high hospital mortality of OAR in elderly patients, on the surgeon’s experience.
Footnotes
Author Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Jasmin Epple and Reinhart T. Grundmann. The statistical analysis was performed by Jasmin Epple and Neelam Lingwal. The first draft of the manuscript was written by Reinhart T. Grundmann and Jasmin Epple, involving all authors. The final version of this paper was approved by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.