
Abstract
Aortoiliac occlusive disease (AIOD) can occur from either chronic, progressive atherosclerotic disease, acute on chronic thrombosis or acute arterial embolism, and can all result in limb ischemia. Bypass surgery had long been the gold standard for treatment for AIOD, however, with advances in endovascular techniques, minimally invasive treatment of aortoiliac lesions has become the first line choice of management in many cases. Herein, we describe a case of utilizing the Inari ClotTriever to perform aortoiliac mechanical thrombectomy and the ARTIX thrombectomy system to perform an embolectomy the superficial femoral artery, highlighting new therapies to treat AIOD.
Introduction
Aortoiliac occlusive disease (AIOD) can occur from either chronic, progressive atherosclerotic disease, acute on chronic thrombosis or acute arterial embolism. All of these conditions can result in limb ischemia. 1 The incidence of acute limb ischemia is 15 cases per 100 000 per persons per year with prevalence higher in patients with cardiovascular disease. 2 Bypass surgery had long been the gold standard for treatment for AIOD, however, with advances in endovascular techniques, the European society of Vascular Surgery now recommends utilizing endovascular techniques such as intra-arterial thrombolysis or mechanical thrombectomy.3-5 Percutaneous aspiration thrombectomy has been shown to be successful as a stand-alone first-line therapy for lower limb ischemia resulting in less use of catheter directed thrombolytics. 6 Herein, we describe a case of utilizing the Inari ClotTriever (Inari Medical, Irvine, CA) for aortoiliac mechanical thrombectomy and the ARTIX thrombectomy system (Inari Medical, Irvine, CA) to perform an embolectomy the superficial femoral artery. Written informed consent has been obtained from the patient for publication of the case report and accompanying images, along with approval by the medical center IRB HP-00085462.
Case Report
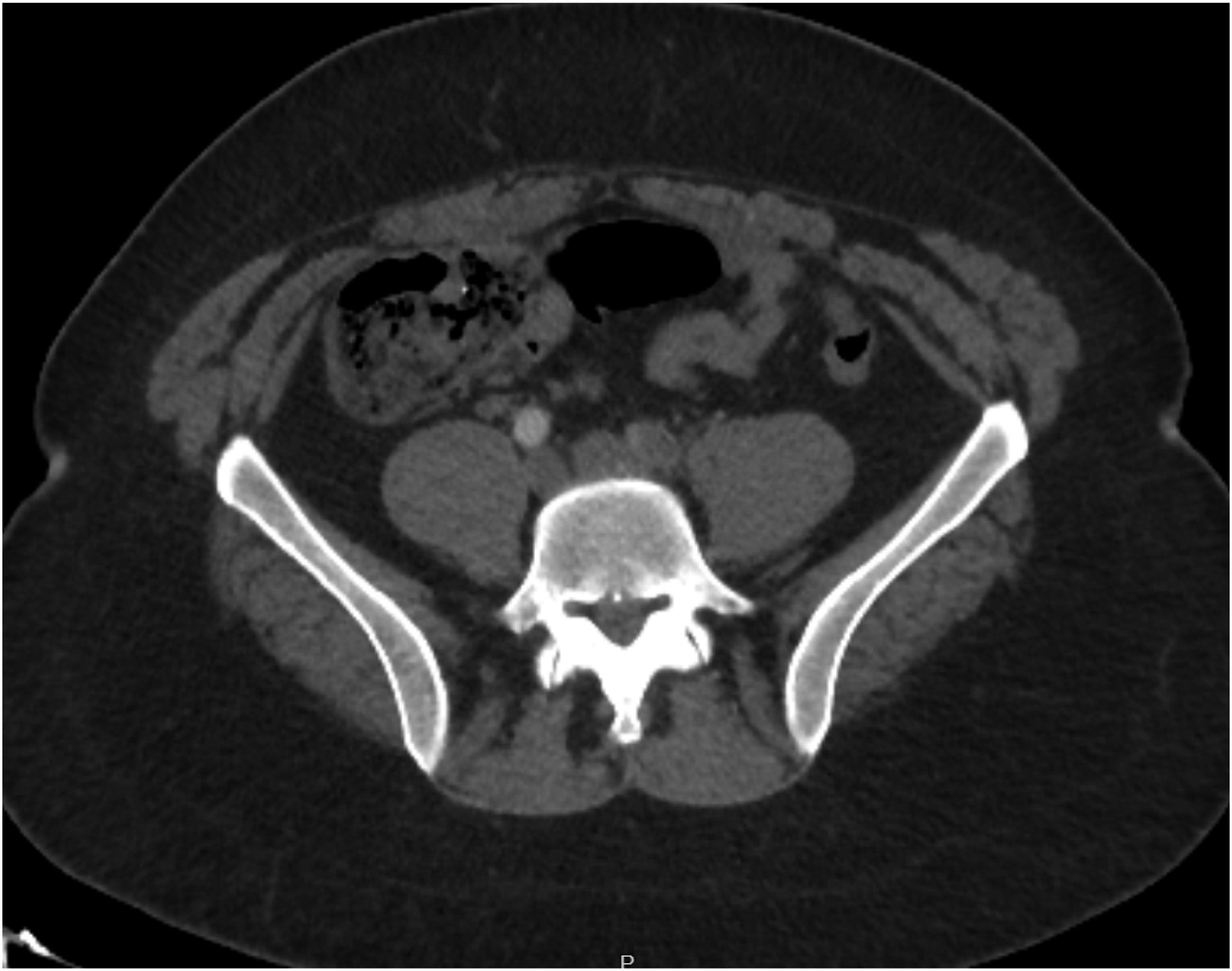
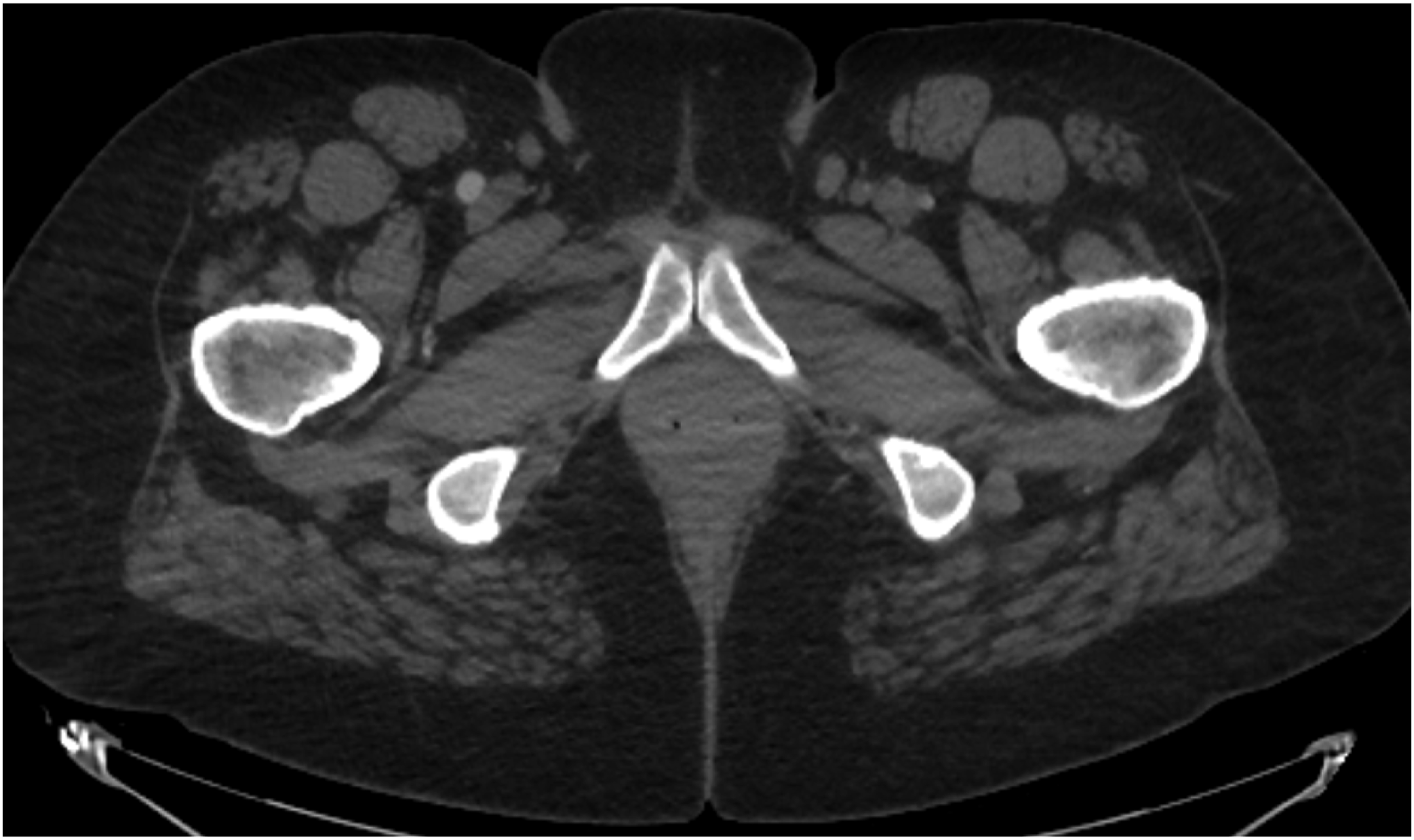
42-year-old female with past medical history of antiphospholipid syndrome, right middle cerebral artery stroke, peripheral arterial disease with several past interventions, and prior deep vein thrombosis currently maintained on rivaroxaban monotherapy, presented for acutely worsening left lower extremity pain and sensorimotor deficits. She was classified as a Rutherford grade IIB, acute limb ischemia. Computerized tomography (CT) scan identified near occlusive lesion of the distal aorta (Figure 1) and near occlusive lesion of the left common iliac artery (CIA) (Figure 2) with an occlusion of the distal common femoral artery (CFA) (Figure 3), one of the profunda branches and proximal superficial femoral artery (SFA). There was reconstitution of the SFA and chronic occlusion of the popliteal artery with reconstitution of the peroneal artery. The patient was taken emergency to the operating room for revascularization. Due prior surgical intervention there was extensive scar tissue in the groin causing high risk for poor healing and infection. Thus, it was decided to perform an endovascular intervention opposed to bilateral CFA cutdowns. CT scan showing partial thrombosis of the aorta. CT scan indicating left common iliac artery occlusion. CT scan indicating occlusion of left common femoral artery.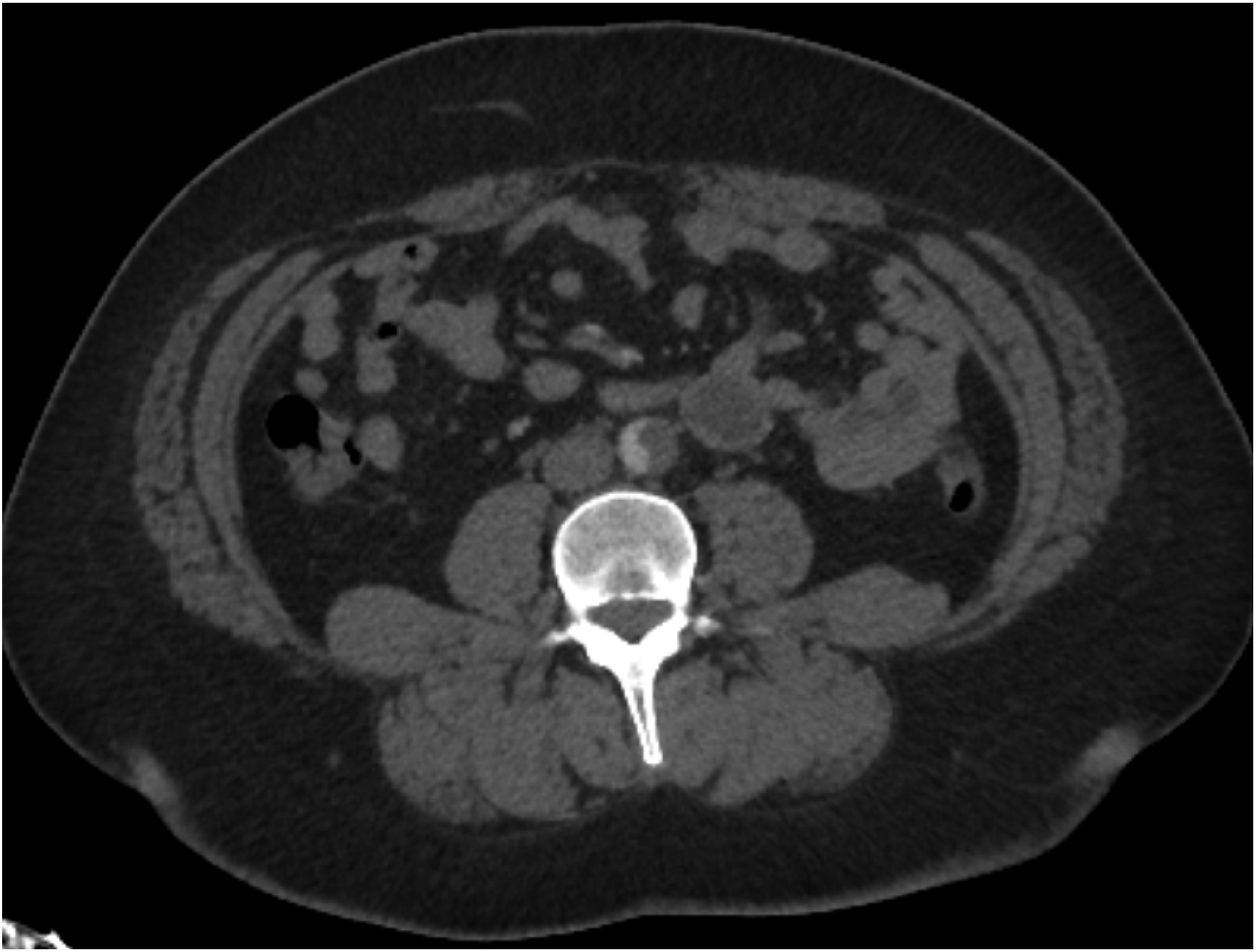
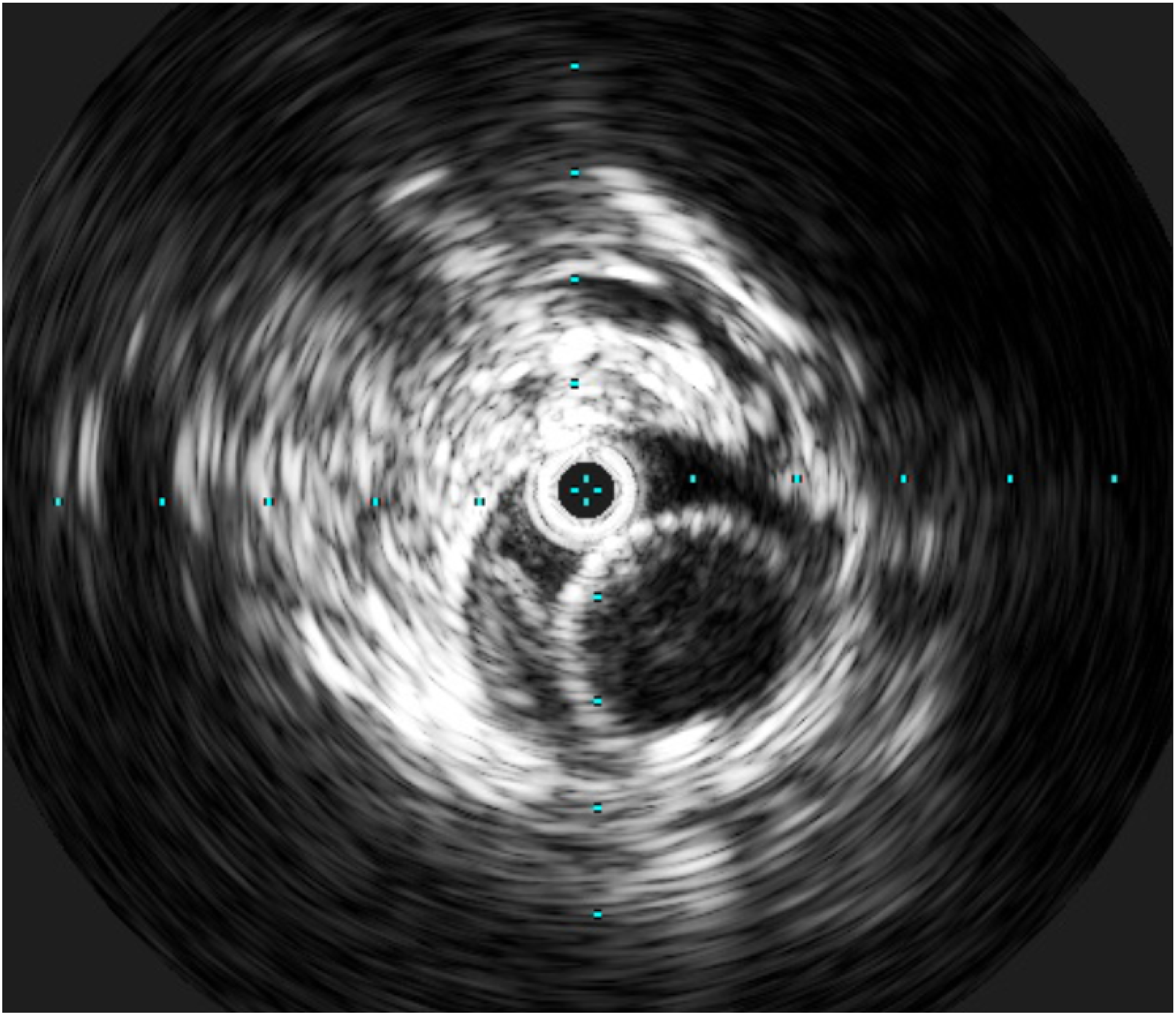
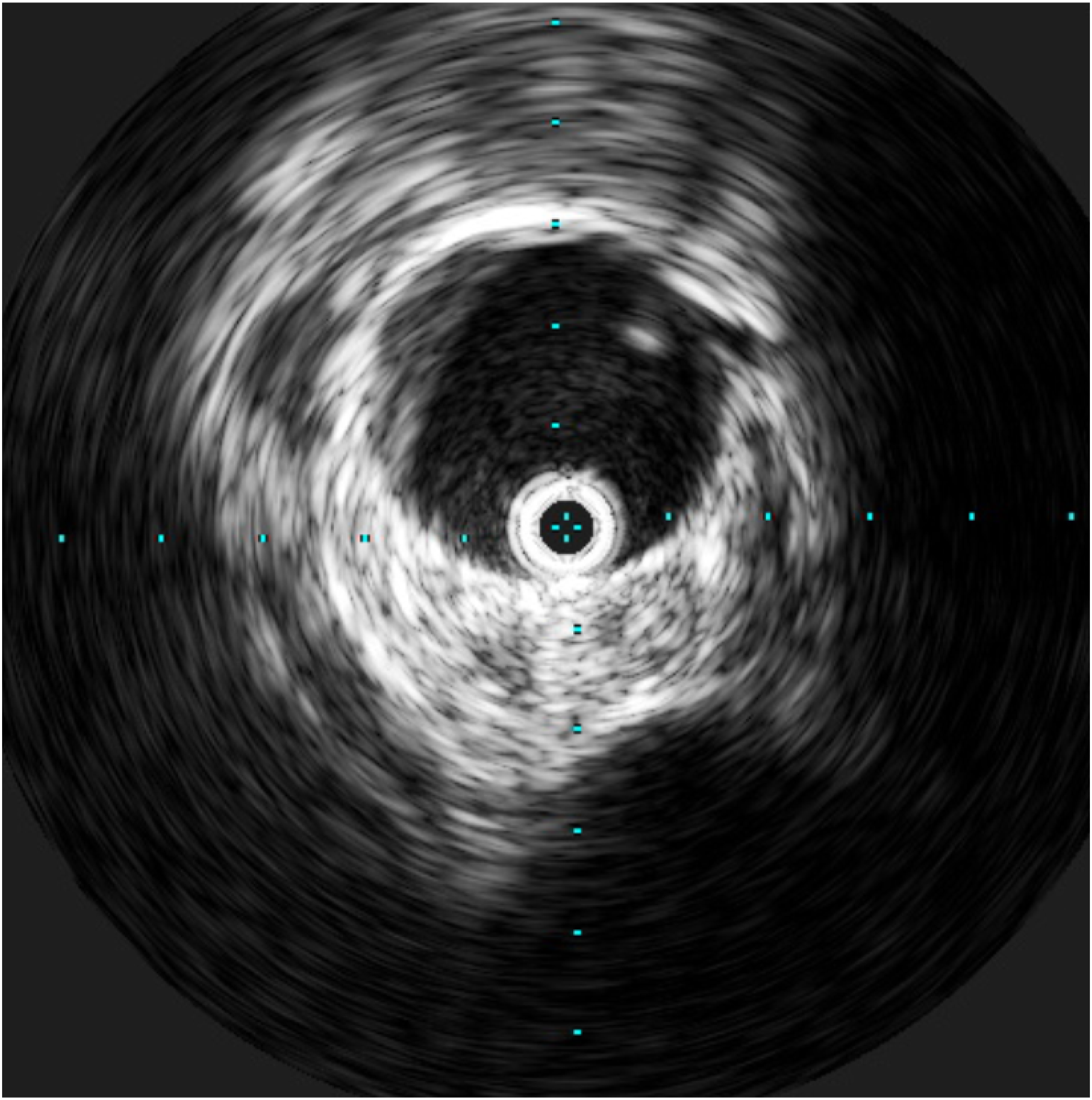
Bilateral mid-common femoral artery percutaneous access was obtained. The left side was accessed above a large embolism at the common femoral artery bifurcation. The patient was then anticoagulated with heparin and activated clotting time was greater than 250 seconds, which was checked intra-operatively. An 11 French sheath was placed in the left common femoral artery and an 8 French sheath in the right common femoral artery. Diagnostic aortogram was preformed that revealed extent of disease in the aorta and iliac systems, identified on pre-operative CT scan, from the right-sided access. Intravascular ultrasound (IVUS) catheter (Philips Healthcare Inc, Best, Netherlands) was passed and confirmed extent of the occlusive disease (Figure 4). An Amplatz wire was passed into the left subclavian artery under fluoroscopic guidance. Next, the Inari ClotTriever mechanical thrombectomy device (Inari Medical, Irvine, CA) was passed on the wire and pulled back multiple times to remove the occlusive atherosclerotic disease and thrombus (Figure 5). The ClotTriever device has a 19 cm length open collection bag, a 45 mm long coring element and a 31 cm shaft length, which is why the stiff wire was placed into the left subclavian artery. The device has a fully expanded diameter of 16 mm. Following 4 passes with the device, completion aortogram revealed improvement in the aortoiliac occlusion (Figure 6). This finding was confirmed with intravascular ultrasound assessment. There was still a large amount of acute on chronic thrombus noted in the distal left common femoral artery due to need to access above the embolus due to the size of the vessel needed for the sheath. Left-sided wires and sheath were removed and arteriotomy was closed in standard fashion. IVUS of aorta Pre-thrombectomy. IVUS of aorta with Clottriever device in aorta during thrombectomy. IVUS of aorta post-thrombectomy.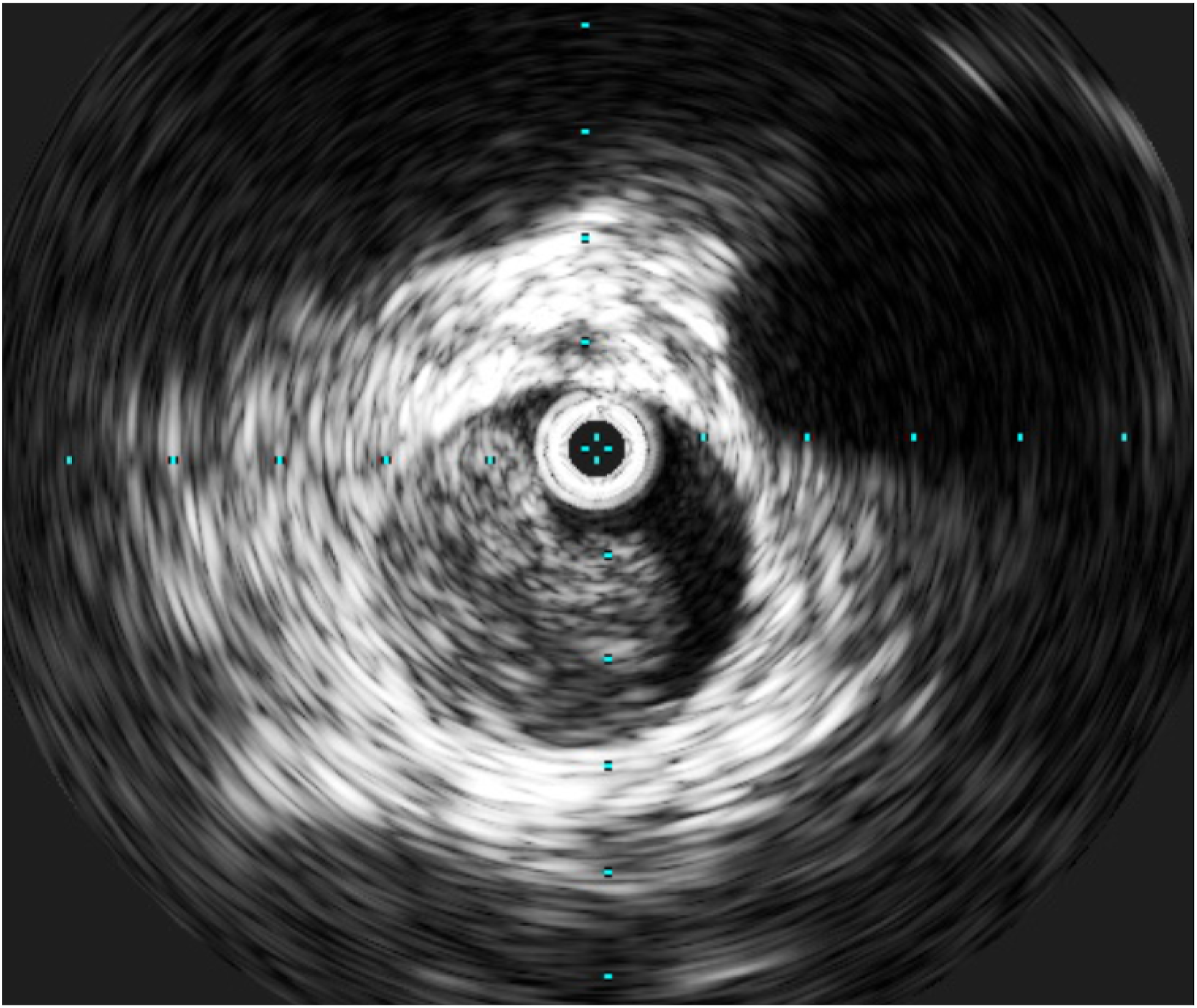
Next from the right-sided access, we went up and over the aortic bifurcation with an Artix thrombectomy sheath and device (Inari Medical, Irvine, CA). The sheath was placed in the external iliac artery and balloon occlusion was begun. Wire was passed through the common femoral thrombus and into the superficial femoral artery. Multiple passes were performed and the femoral bifurcation was revascularized completely (Figure 7). The patient had chronic occlusion of the popliteal artery with reconstitution of the peroneal artery giving rise to the plantar vessels in the foot which would need to be addressed once recovered from this operation. At this point the procedure was concluded and wires and catheters were removed. Arteriotomy was closed and patient was taken to the recovery room. The procedure lasted approximately 30 minutes. Her lower extremity compartments remained soft and no fasciotomy was indicated. Post intervention angiogram.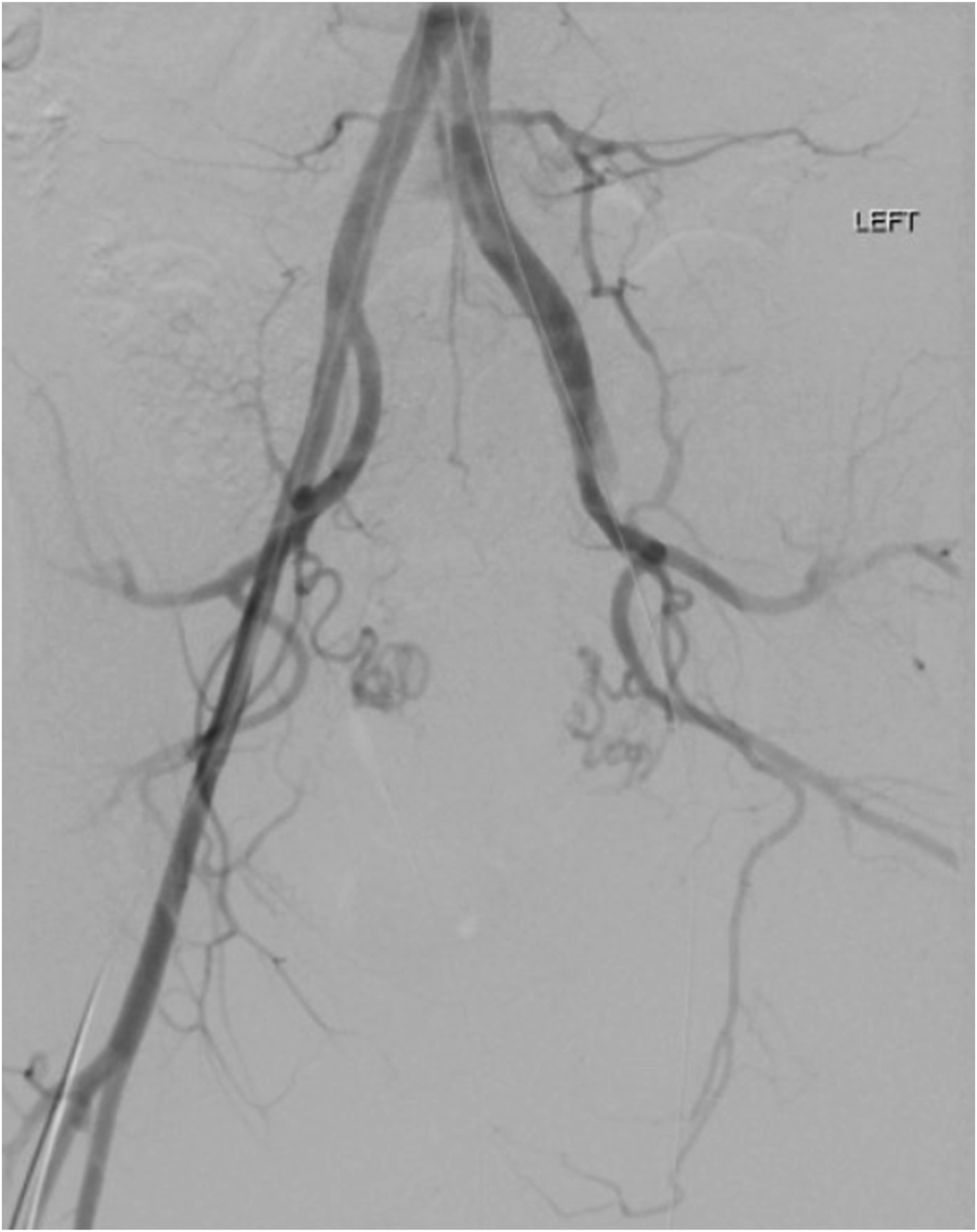
Post-operative course for the patient included starting on anticoagulation and discharge home on post-operative day 4. This was the index procedure for this patient to provide inflow. Four weeks later she underwent left SFA to plantar bypass to restore arterial perfusion to her left lower extremity and heal and medial foot wound that had developed. She now ambulates pain free and has returned to work and is an active member of the community.
Discussion
The benefit of percutaneous thrombectomy in acute aortoiliac occlusive disease is the rapid ability to remove a large amount of clot burden and rapidly establish reperfusion which is beneficial for patient prognosis and limb salvage. 7 The Inari ClotTriever an endovascular mechanical thrombectomy devise designed to remove large thrombi and emboli in a single session without the need for thrombolytics. 8 The ClotTriever was found to be safe and effective in treating acute and nonacute lower extremity DVTs. 9 While this devise is generally used in venous procedures it is approved for arterial interventions as well. In this case the ClotTriever was utilized to capture and remove a large clot burden from distal aorta and iliac arteries due to the size of catheter needed. Other devises on the market would not have given the length needed to perform this endovascular procedure.
The ARTIX thrombectomy system is a mechanical thrombectomy devices which captures emboli for thrombectomy procedures. 10 The ability to perform peripheral mechanical thrombectomy with aspiration to remove thrombus percutaneously allows for procedures to remain minimally invasive with faster recovery time. Treating AIOD minimally invasively is ideal for complex patient with many comorbid conditions or in this case re-operative groins with scar tissue.
Morgan & Belli highlight that percutaneous thrombectomy is an established technique for removing acute thrombus from the arterial system and can be used as sole therapy or adjunctive. 11 Recent literature has highlighted using percutaneous thrombectomy as adjunctive treatments with success in acute limb ischemia. Loffroy et al. highlighted the use of percutaneous mechanical atherectomy in conjunction with percutaneous thrombectomy as a minimally in invasive approach for recanalizing arterial lesions. 12 Mechanical thrombectomy is also discussed as a first line minimally invasive treatment for infrainguinal disease which is safe, rapid, and effective. 13 The use of endovascular therapy for extensive AIOD has been shown to have technical success with resolution of symptoms and low complications. 4 With AIOD affecting over 2 million people 14 in the United States alone, finding optimal ways to treat these lesions is needed.
There are possible complications with using any medical devise or procedure. For example, the coring element here could have caught on the aortic plaque. If the Inari ClotTriever is not oriented optimally it can cause dissection of the aorta. As with all procedure, the individual and all possible risks and benefits were considered. In this case, using endovascular technique for the index procedure lead to short hospital stay and optimized her for the eventual lower extremity bypass to treat her ischemic rest pain.
Conclusion
Endovascular treatment for acute limb ischemia has been show to have excellent clinical and technical results. Finding new treatment modalities for complex patients is necessary as comorbid conditions can make traditional surgical options risky for patients. The ClotTrevier devise not only effective in removing large clot burden from lower extremity veins, it was also successful in removing thrombus from the distal aorta. The Arterx Thombinator system can be successfully used for thromboendarterectomies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.