
Abstract
Botulinum toxin type A (BoNT/A) is a potent neurotoxin with widely use range, for the good outcomes in the treatment of pain, it was considered as an unique analgesic drugs with the feature of sustained efficacy after a single application, but up to now, treating chronic limb-threatening ischemia (CLTI) with BoNT/A was rarely reported. We present a 91-year-old man with CLTI, the main clinical manifestations were left foot rest pain, intermittent claudication and toe necrosis, the patient refused invasive treatments, and the pain failure to respond to conventional analgesic drugs, the subcutaneous injections of BoNT/A was performed to the patient. The pain score on the visual analog scale (VAS), decreased from 5-6 (before treatment) to 1 within days after infiltration, and keep in 1-2 of VAS during follow-up. Our case report demonstrated that BoNT/A may be an unique minimally invasive solution for treating rest pain in CLTI.
Introduction
Chronic limb-threatening ischemia (CLTI) is a clinical syndrome defined by the presence of peripheral artery disease (PAD) in combination with rest pain, gangrene, or a lower limb ulceration >2 weeks duration. 1 The treatment of CLTI include pharmacotherapy, revascularization, nonrevascularization therapies, lifestyle modifications, wound care, and amputation. 1 Although open surgical and endovascular revascularization are the important treatments for limb salvage, but some elderly patients with high risk factors or disadvantaged anatomy, unsuitable for procedure that have to accept conservative treatment, when the conventional pharmacotherapy not result in good outcome, the rest pain, intermittent claudication and toe necrosis are the thorny problems that have a serious negative impact on the patients’ quality of life, especially rest pain, it would be a great challenge for clinicians.1,2 Botulinum toxin type A (BoNT/A) is a potent neurotoxin, with good therapeutic effects in treating pain, such as chronic migraine, posttraumatic neuralgia, trigeminal neuralgia, complex regional pain syndrome (CRPS), and Raynaud’s phenomena (RP).3-7 At present, treating rest pain with BoNT/A in CLTI was rarely reported. This article reported a case of CLTI received a good outcome by subcutaneous injections of BoNT/A.
Case Report
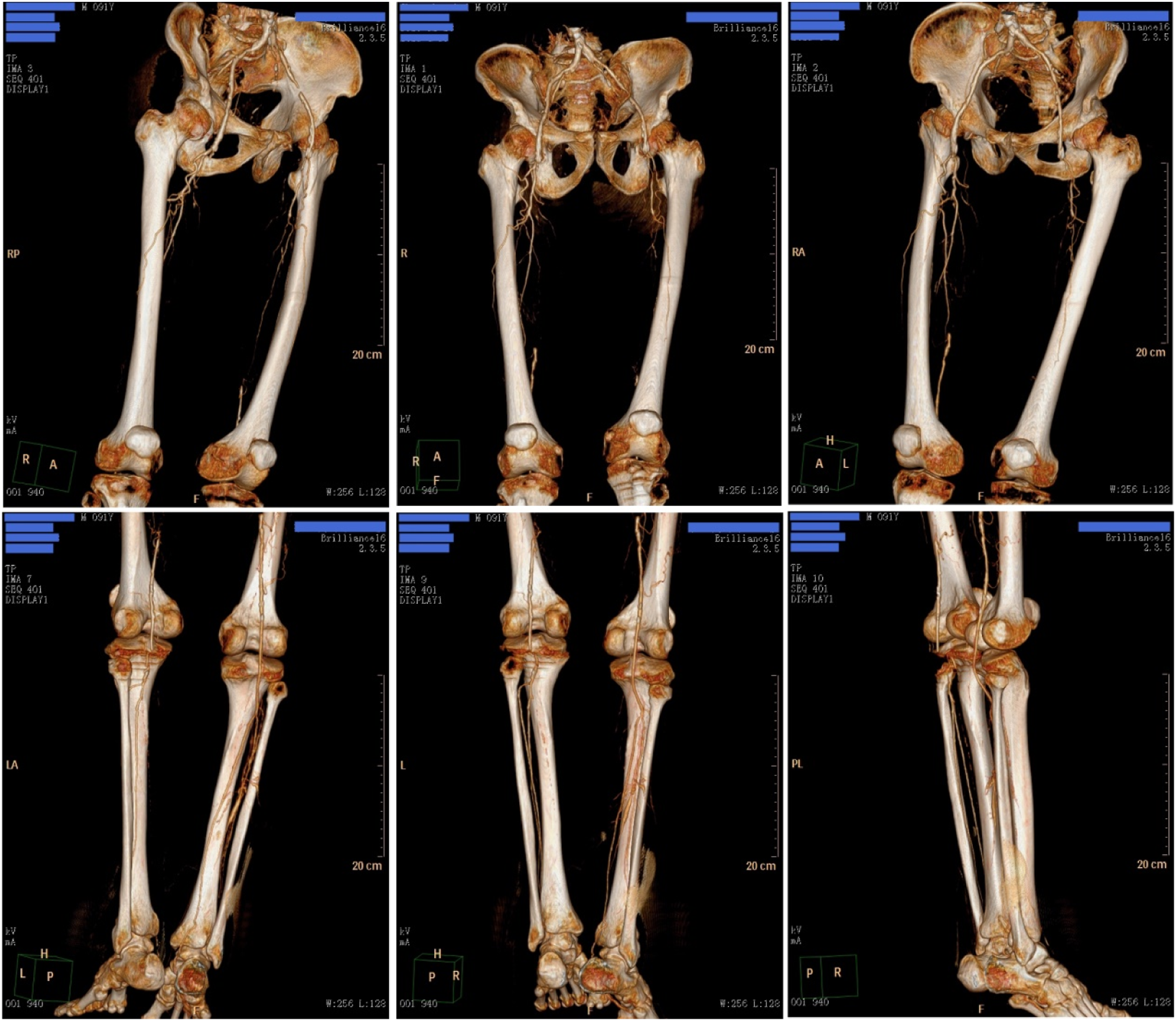
A 91-year-old man with a history of hypertension complained of left foot rest pain, intermittent claudication, and toe necrosis for 20 days, with sleep disturbance caused by the pain. Physical examination revealed an ulcer in the dorsum of left foot, dry gangrene of the 2nd and 3rd toe (Figures 1A and 1B), diminished pulsation of left dorsalis pedis artery with low skin temperature of left foot. The hematological investigation showed blood urea nitrogen (19.01 mmol/L, normal range 2.9-7.5 mmol/L), serum creatinine (261.8 μmol/L, normal range 70-115 μmol/L), cystatin C (3.74 mg/L, normal range 0-1.16 mg/L), and urine β-2 microglobulin (6.87 mg/L, normal range 1.01-2.97 mg/L), indicating renal insufficiency status. The computed tomography angiography (CTA) images demonstrated multilevel arteriosclerosis and stenosis of lower extremity arterial (Figure 2). Based on the above findings, the diagnosis was CLTI. (A and B) Dry skin with an ulcer (1.5 cm in diameter, covered with dark-brown eschar) on the dorsum of left foot, the 1st, 4th, and 5th toe was mild red and swollen, dry gangrene visible on the 2nd and 3rd toe. The computed tomography angiography (CTA) images demonstrated severe stenosis of the bilateral femoral arteries, intermediate stenosis of the left posterior tibial and right anterior tibial artery, arteriosclerosis of the bilateral external iliac, femoral, superficial femoral, popliteal, anterior tibial, posterior tibial, peroneal, and dorsalis pedis arteries.
The tramadol (50 mg 4 times a day) and meloxicam (7.5 mg once daily) were used for treating pain, alprazolam (0.4 mg as needed at night) for the insomnia, intravenously administered cefazolin sodium (1000 mg twice daily) for anti-infection treatment, alprostadil (10 μg once daily) and ginkgo biloba leaf extract (35 mg once daily) to inhibit platelet aggregation and improve peripheral microcirculatory, the toe gangrene was covered with gauze dressing after disinfection, the patient underwent the treatment for 5 days but failure to relieve pain. The patient refused invasive treatment including angioplasty and stenting because of the advanced age. The subcutaneous injections of BoNT/A was performed with the patient’s consent, the injection site is in the anterior and middle of the left foot (Figures 3A and 3B), where it was smeared with compound lidocaine cream and covered with transparent dressing for about 1 hour, so as to decrease pain during injection. Multipoint injections with a total dosage of 100 IU (BoNT/A 100 IU was mixed with .9% saline 5 mL diluted to 20 IU/mL concentrations, 50 injection points, 2 IU per injection point, 1-1.5 cm distance per point, the injection depth was 2-3 mm in the dorsum of left foot, 3-4 mm in the plantar). The pain score on the visual analog scale (VAS), decreased from 5-6 (before treatment) to 1 within 3 days after infiltration, keep in 1-2 of VAS during the follow-up period (1 month after treatment, the patient passed away peacefully), with sleep improvement, but the ulcer and gangrene unchanged. (A and B) The injection site is in the anterior and middle of the left foot, excluding the 2nd and 3rd toe, and the areas that cannot be injected (including the gangrene, the ulcer, and the eschar).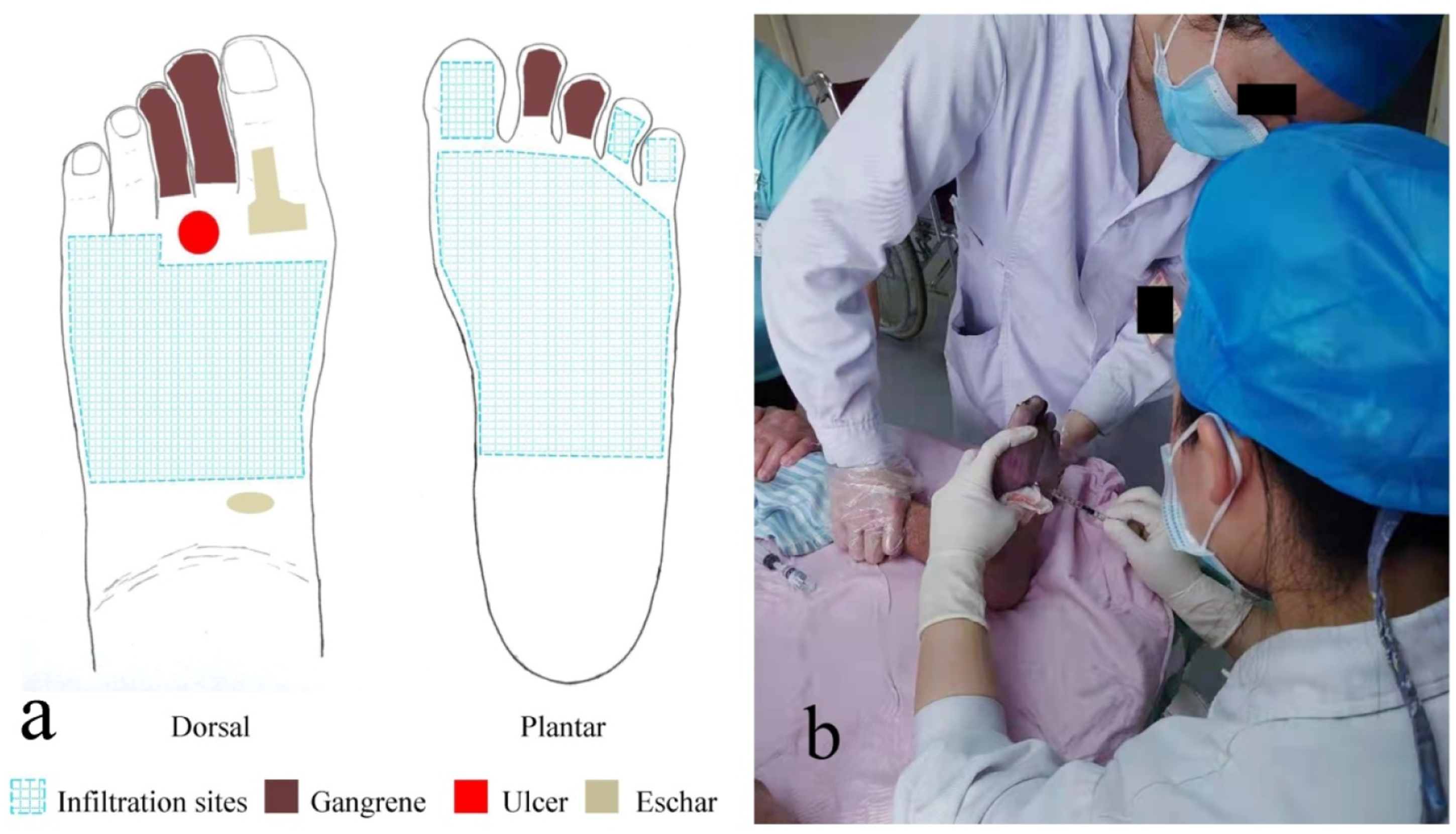
Discussion
CLTI cause by atherosclerosis in peripheral artery, lead to different degrees of stenosis, even complete occlusion that requiring amputation or life-threatening.1,2 The main clinical manifestation of CLTI include rest pain, intermittent claudication, ulcer and gangrene, it can greatly reduce the patients’ quality of life, especially to the psychological frail patients. The prevalence of CLTI increases with age, as the population ages, CLTI became a thorny problem and heavy burden for public health.1,2
The treatment of CLTI include pharmacotherapy (lipid-lowering, antiplatelet, analgesic, antihypertensive, glycemic control, etc.), revascularization (bypass surgery, angioplasty, stent placement, atherectomy, ect.), nonrevascularization therapies, lifestyle modifications (smoking cessation, diet, exercise), wound care, and amputation. 1 Although revascularization is the primary treatment for improving perfusion and reducing amputation, but some elderly patients with high risk factors, unsuitable for procedure that have to accept conservative treatment, on the other hand, there are still a few unsatisfactory outcomes, include operative risk, comorbidity, postoperation restenosis or reocclusion, requiring multiple hospitalizations, prolonged care, considerable medical and care costs.1,2 The treatment decision is base on the patients’ option and risk estimation (involves physical condition, periprocedural risk, life expectancy, limb staging, and anatomic pattern of disease, etc.), not every patient with CLTI has the candidacy for revascularization procedures. 1
Current studies reveal that the acute kidney injury cause by contrast is a common postoperative complication in PAD patients undergoing vascular surgery and endovascular therapy, the high-risk factors including advanced age (>75 years), CLTI, pre-existing chronic kidney disease, congestive heart failure, etc.8,9 It makes endovascular treatments and operative treatments more difficult because of the risk of destructing the remaining renal function, especially the pre-existing renal insufficiency among CLTI patients lead to worse outcomes (including the incidence of major adverse cardiovascular events, target lesion revascularization, amputation, and high mortality).8-11 So in our case, the conservative treatment was the most appropriate choice based on the risk estimation and the patients’ option, but it is frustrating that the rest pain did not respond to conventional analgesic drugs and the opiate analgesia was not for prolonged use. In view of the sustained effect and safety have been proven in treating pain with BoNT/A, the patient accepted the subcutaneous injections of BoNT/A, the pain reduced rapidly and maintained a good effect after treatment. Since 1989, BoNT/A was applied in clinical practice with the approval from US Food and Drug Administration, it had rapidly developed and constantly opened up new applications.4-6 BoNT/A injection is an emerging therapy for some pain diseases such as trigeminal neuralgia, headache, postherpetic neuralgia, post-surgical neuralgia, CRPS, and RP, the current studies noted the encouraging result in rapid pain relief, furthermore, favor the healing of skin ulcer in treating RP.3-7
Rest pain due to insufficient blood, reduced oxygenation and nutrition in peripheral tissues and sensory nerve, improved peripheral microcirculatory will great help to relieve pain.1,2 Rest pain frequently worse at night, often requires opiate analgesia to control when failure to respond to conventional analgesic drugs, but the adverse drug reactions (tolerance, addiction, constipation, drowsiness, respiratory depression, etc.) will be another trouble to the patient. 1 To date, a lot of studies have demonstrated that BoNT/A is an excellent analgesic drugs in pain management, the mechanisms of action on pain is extremely complicated, relates to the specificity of BoNT/A effect, inhibit the release of inflammatory mediators and peripheral neurotransmitter, cleaves the SNAP-25 molecules, the blocking of ectopic sodium channels, central effects by the retrograde axonal transport of BoNT/A, influence the ascending pain processing pathway, etc.4,5,7 The effect on blood vessel, BoNT/A can relieve arterial spasm and improve blood perfusion in the injection site, so as to alleviate pain and promote ulcer healing.5,6 Base on the above studies, it may be illustrate the mechanisms of pain relief in our case.
Conclusion
As of now, treating rest pain with BoNT/A in CLTI was rarely reported, our case report displayed an unique minimally invasive treatment for the rest pain. The limitation of this case report is 1 sample, the clinical efficacy and safety should be verified in more CLTI patients.
Footnotes
Acknowledgments
The authors wish to acknowledge Wantian Yang, Huaying Lu for their technical support.
Author Contributions
All authors have contributed to the paper. Jiaoxiong Xu: Literature search, wrote and edited the manuscript. Haofeng Lin: Conception of the paper, definition of intellectual content, guarantor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethics committee approval was not required for case report, our institution does not require ethical approval for reporting individual cases.
Informed Consent
The patient was unrecognizable, and the patient’s information and photographs were carefully protected and anonymity. The patient was deceased, the written informed consent has been obtained from the patient’s family for publication of the case report and accompanying images.
Data Availability Statement
The data used for this case report are included in this manuscript.