
Abstract
Background
Abdominal aortic aneurysm (AAA) has a prevalence of 4.8%. AAA rupture is associated with significant mortality, thus surgical intervention is generally required once the aneurysm diameter exceeds 5.5 cm. Endovascular aneurysm repair (EVAR) is the predominant repair modality for AAA. However, in patients with complex aortic anatomy, fenestrated or branched EVAR is a superior repair option vs standard EVAR. Fenestrated and branched endoprostheses can be off-the-shelf or custom-made, which offers a more individualised approach.
Aim
To summarise and evaluate the clinical outcomes achieved by fenestrated EVAR (FEVAR) and branched EVAR (BEVAR), and to explore the role of custom-made endoprostheses in contemporary AAA management.
Methods
A literature search using Ovid Medline and Google Scholar was conducted to identify literature pertaining to the use and outcomes of fenestrated, branched, fenestrated-branched and custom-made endoprostheses for AAA repair.
Results
FEVAR is an effective repair modality for patients with AAA that offers similar early survival, improved early morbidity but higher rates of reintervention in comparison to open surgical repair (OSR). Compared with standard EVAR, FEVAR is associated with similar in-hospital mortality yet higher rates of morbidity, especially regarding renal outcomes. BEVAR outcomes are rarely reported exclusively in the context of AAA repair. When reported, BEVAR is an acceptable alternative to EVAR in the treatment of complex aortic aneurysms and has similar reported complication issues to FEVAR. Custom-made grafts are a good alternative treatment option for complex aneurysms where hostile aneurysm anatomy precludes the use of conventional EVAR and sufficient time is available for the manufacturing of such devices.
Conclusion
FEVAR offers a very effective treatment for patients with complex aortic anatomy and has been well-characterised over the past decade. RCTs and longer-term studies are desirable for unbiased comparison of non-standard EVAR modalities.
Introduction
Endovascular aneurysm repair (EVAR) is a well-established and more effective alternative to open surgical repair (OSR) for the management1-5 of abdominal aortic aneurysm (AAA).6-8 Standard EVAR requires a certain degree of anatomic normality, for example adequate infrarenal aortic neck length and angulation to enable device fixation. 9 Innovation in the field of EVAR has led to the development of more complex endografts. These include both fenestrated and branched devices which has increased the anatomical spectrum of AAAs that can be effectively treated using an endovascular approach. 10
Fenestrated endovascular aneurysm repair (FEVAR) was first performed in 1996 and has since been shown to be a safe and effective treatment modality for AAA.11-14 FEVAR is beneficial where hostile infrarenal neck anatomy would make standard EVAR graft fixation difficult. 10 Fenestrated grafts are mostly described in the context of treating AAA which are supra or juxtarenal (SRAAA, JAAA).15-17 At present, no randomised controlled trials (RCTs) have been performed to compare complex EVAR/FEVAR with OSR. Branched EVAR (BEVAR) is used to maintain perfusion to visceral arteries in those AAA where the origin of the visceral arteries is part of the aneurysm or adjacent to the aortic neck where standard EVAR is not easy to perform. 18 It can also be used as an adjunct to FEVAR, where it is described as F/BEVAR. 19 ‘Custom-made’ FEVAR devices are an effective alternative to ‘off-the-shelf’ endoprostheses and are tailored to the patient’s individual anatomy.20,21 This study aims to summarise the literature on the general performance of FEVAR, BEVAR and F/BEVAR as methods for managing AAA and to evaluate the progressive uptake of “custom-made” approaches in contemporary aortic surgical practice.
Methods
A literature search using Ovid Medline and Google Scholar was conducted to identify literature pertaining to the use and outcomes of fenestrated, branched, fenestrated-branched and custom-made endoprostheses for AAA repair. Key search terms included ‘Fenestrated endovascular aneurysm repair’, ‘FEVAR’, ‘Branched endovascular aneurysm repair’, ‘BEVAR’, ‘F/BEVAR’, ‘F-BEVAR’, ‘Custom-made endovascular aneurysm repair’ and ‘Physician-modified endovascular grafts’. Relevant literature from 2000 till present was evaluated and discussed.
Results
Fenestrated Endovascular Aortic Repair
Fenestrated endografts (see Figure 1) consist of nitinol reinforced fenestrations and scallops which enable blood to continue to flow to the renal and visceral arteries following insertion. This enables a more proximal graft fixation than with a standard EVAR device.
9
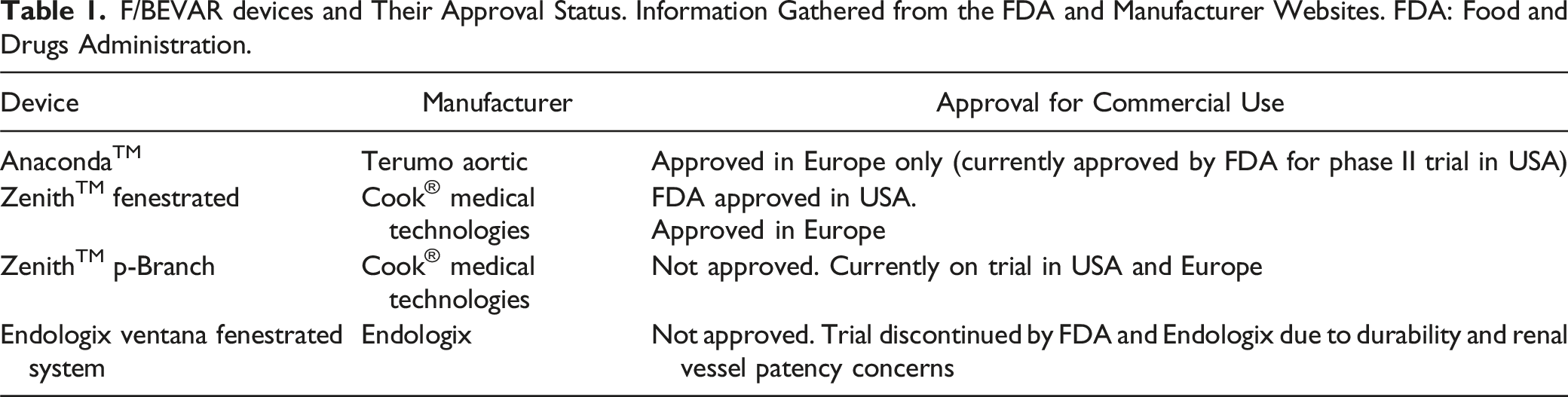
Examples of fenestrated endografts include the AnacondaTM fenestrated graft (Terumo Aortic, USA) which has been used for severely angulated infrarenal neck lengths, and the Zenith® fenestrated graft by Cook® Medical technologies.
22
Contemporary FEVAR grafts are included with their name, manufacturer, and approval status in Table 1. A fenestrated graft. Superiorly there is a scallop for the superior mesenteric artery whilst inferiorly fenestrations for the left renal artery (small arrow) and right renal artery (see right, lateral aspect of the graft) can be seen. Reproduced from Cross, et al. 9 by permission of Oxford University Press. F/BEVAR devices and Their Approval Status. Information Gathered from the FDA and Manufacturer Websites. FDA: Food and Drugs Administration.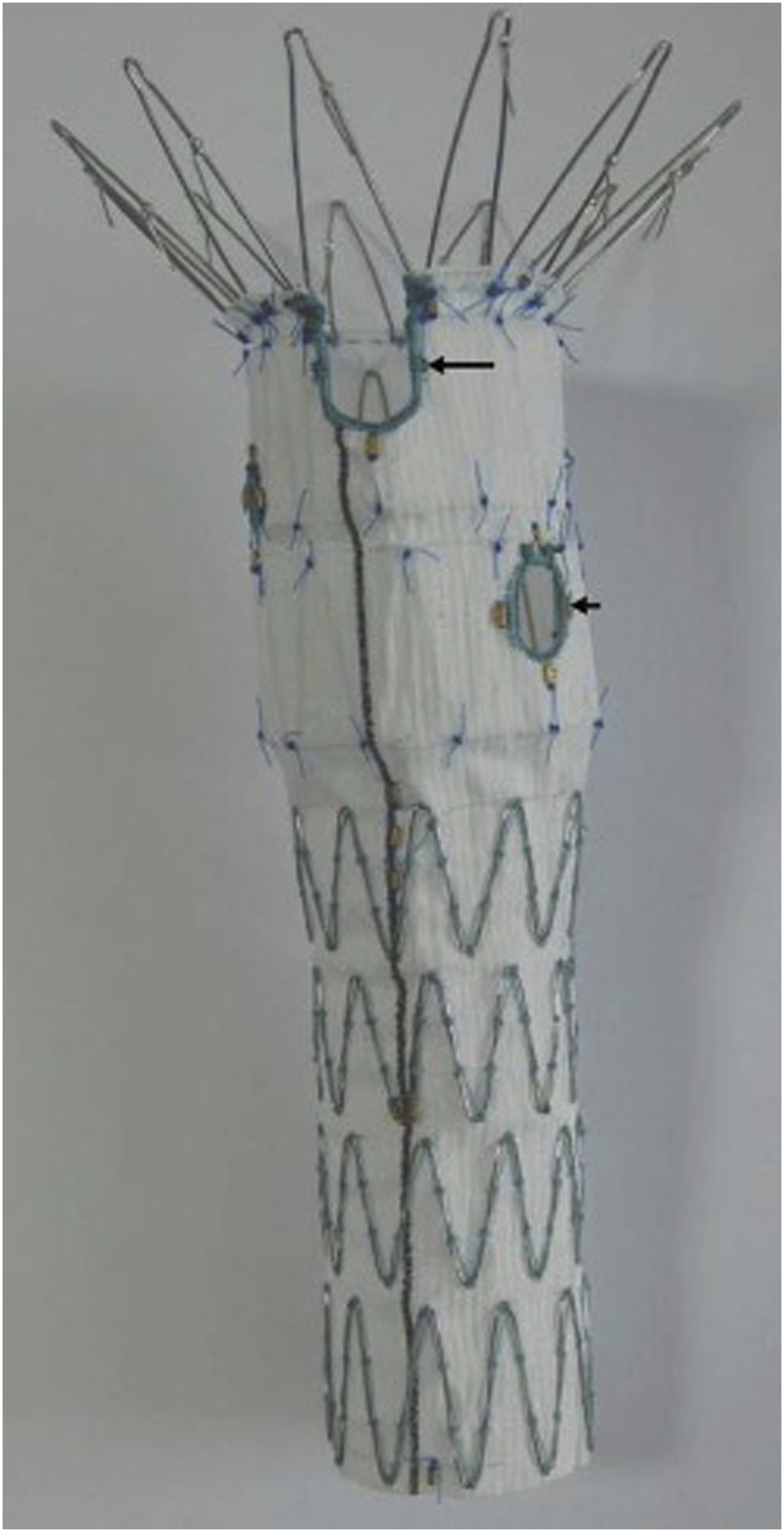
There are crucial steps required to safely deploy a fenestrated, rather than standard EVAR endograft. During stent deployment, the fenestrations are cannulated (usually via the femoral arteries) and then sealed from the origin with a covered stent extending into the respective coeliac/mesenteric and renal arteries (see Figure 2).
9
Risk of long-term graft migration are reduced by ensuring at least 2 fenestrations and stents are placed. Hence, this would mean either 2 renal artery stents or 1 renal artery and 1 superior mesenteric artery (SMA) stent.
23
Other technical points for a visceral artery stent to be durable long term is at least 5 mm of overlap into the target artery from the fenestration.
23
Post-FEVAR angiography is performed to ensure sufficient visceral artery patency and to assess for endoleaks.
23
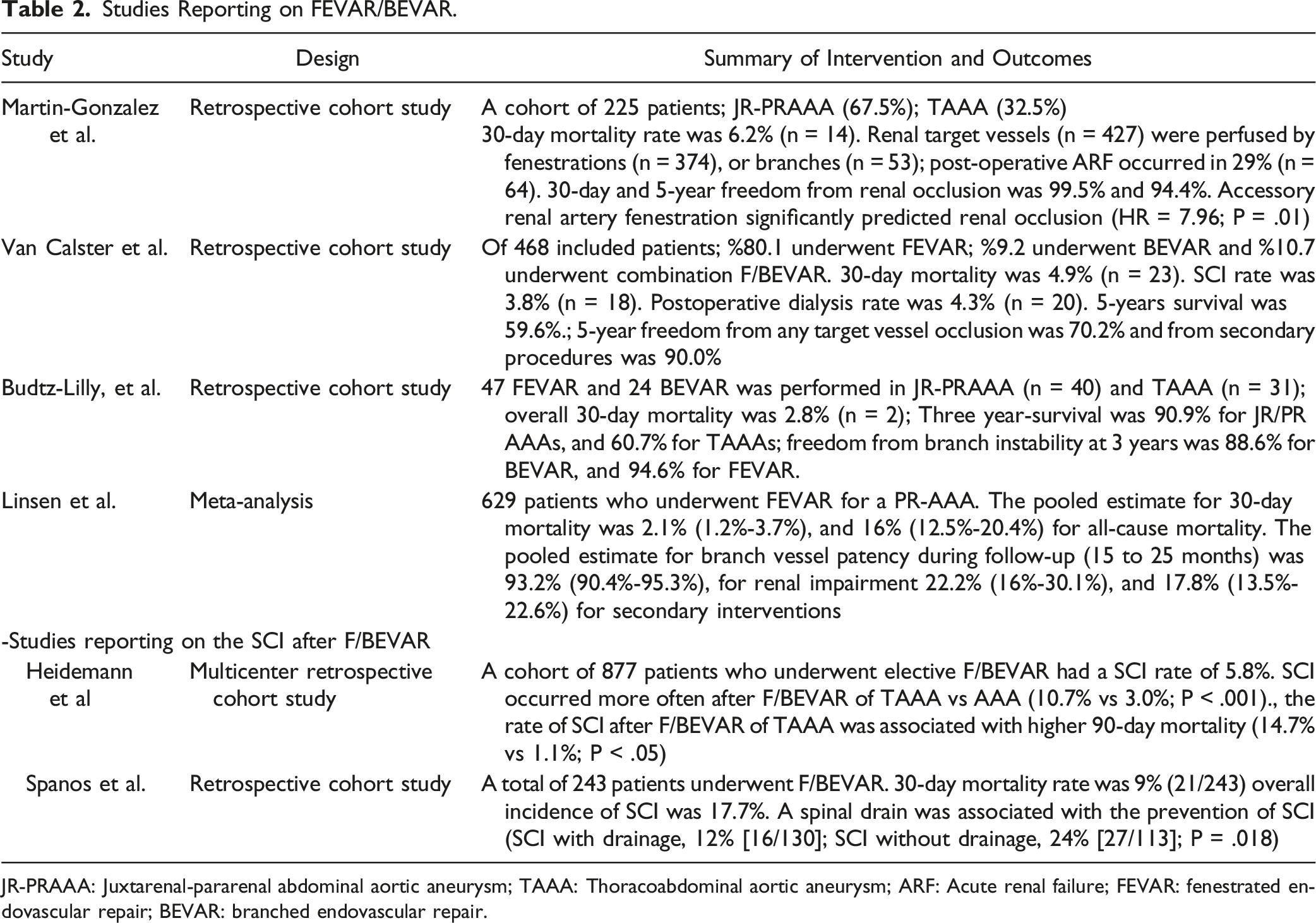
A summary of interventions and outcomes in studies reporting on F/BEVAR is provided in Table 2. Intraoperative imaging showing the cannulation and stenting of the renal arteries during the FEVAR procedure. A stent can be seen in the cannulated left renal artery, whilst a sheathed cannula is seen in the right renal artery. Reproduced from Cross, et al. 9 by permission of Oxford University Press. Studies Reporting on FEVAR/BEVAR. JR-PRAAA: Juxtarenal-pararenal abdominal aortic aneurysm; TAAA: Thoracoabdominal aortic aneurysm; ARF: Acute renal failure; FEVAR: fenestrated endovascular repair; BEVAR: branched endovascular repair.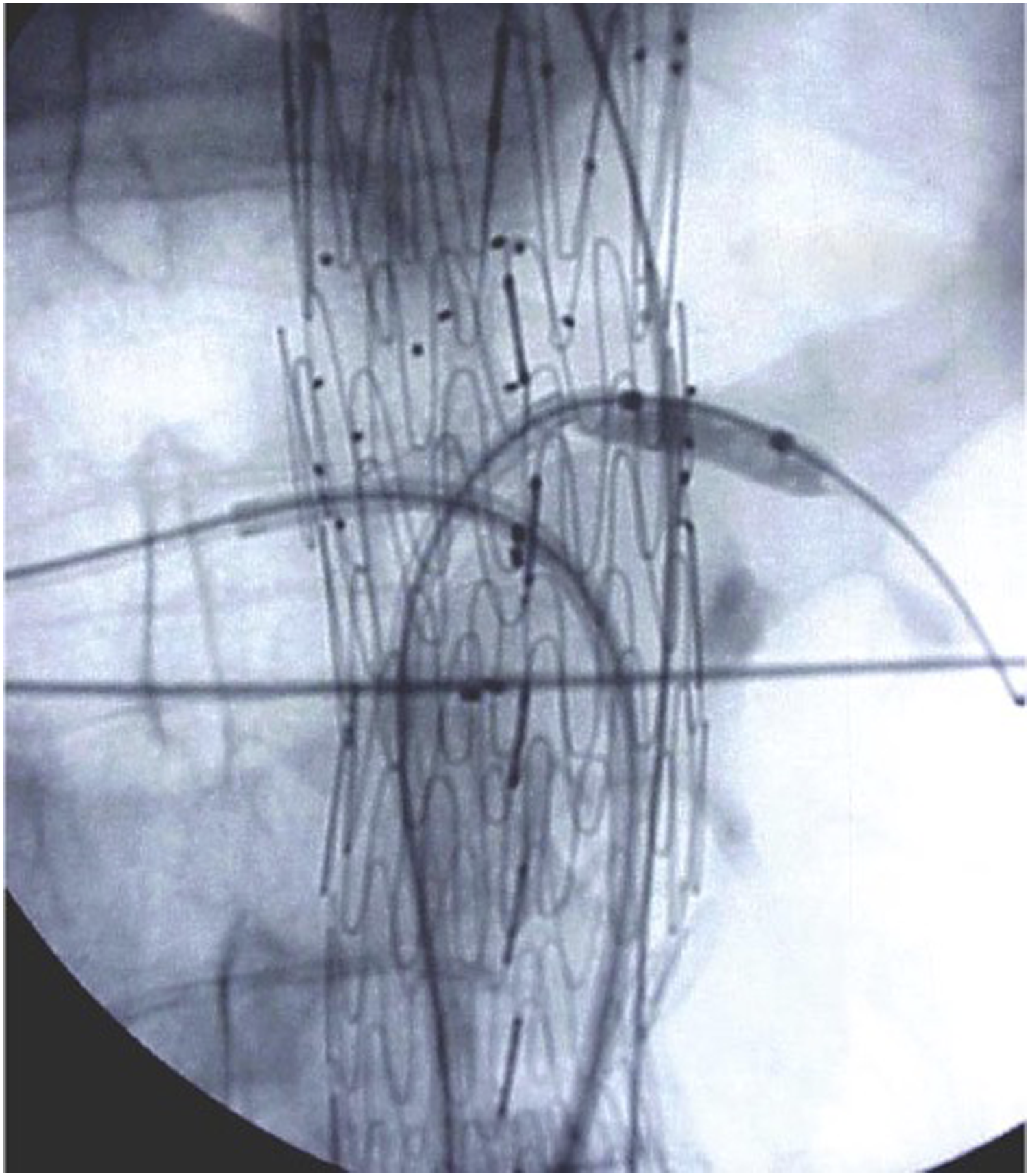
Perioperative Outcomes
Perioperative outcomes are key in defining the immediate success of a surgical intervention. A 2019 meta-analysis including 2974 patients compared outcomes in patients managed with either FEVAR or OSR. 15 This showed no significant differences in 30-day mortality occurred (3.3% for FEVAR; CI 2.0 - 5.0; vs 4.2% for OR; CI 2.9 – 5.7). 15 Lower rates of early morbidity was observed for FEVAR compared to OSR (23.1; CI 16.8 – 30.1; vs 43⋅5; CI 34.4 – 52.8), yet higher late re-intervention rate (11.1% vs 2.0%) was noted for FEVAR. 15 FEVAR therefore seemed to obtain comparable short-term outcomes, despite its use in patients with higher rates of pre-existing comorbidities (double rate of baseline renal dysfunction, higher rates of ischaemic heart disease and pulmonary dysfunction). 15 A medium-sized retrospective review recently defined further benefits of FEVAR (n = 89) vs OSR (n = 195) in patients with pre-existing renal disease. Inclusion criteria were adults with eGFR <60 mL/min, but not requiring dialysis, who underwent elective, non-ruptured JAAA repairs between 2012-2018. 24 No significant difference in 30-day mortality was seen but FEVAR was associated with comparatively less renal dysfunction (3.4% vs 11.8%; odds ratio .24; 95% CI [.07 - .86]; P = .029), significantly shorter ICU stay (0 days vs 3 days, P < .0001) and overall hospital length of stay (3 days vs 8 days, P < .0001). 24 Also, FEVAR showed no statistically significant difference in in-hospital mortality, though the incidence of major complications with FEVAR was higher compared to EVAR. 16
Renal Outcomes
Renal function decline (RFD) post-OR or post-EVAR is well described.25-27 Locham and colleagues 16 retrospectively reviewed renal outcomes in both EVAR and FEVAR. After adjusting for patients’ demographics and comorbidities, FEVAR was associated with a greater than 40% odds of acute renal complications compared to standard EVAR. 16 This study however was non-randomised and the adverse renal outcomes observed in the FEVAR group possibly a reflection of the more complex anatomy that necessitated FEVAR. 16 Other studies have also reported adverse renal outcomes following FEVAR.28-30 Poor renal outcomes following FEVAR may be due greater degree of graft manipulation, increased use of contrast media, and risk of thrombosis or vessel injury during renal artery manipulation and stenting.16,31 The most ominous outcome following FEVAR is renal artery occlusion which can result in permanent haemodialysis. 32
The lack of consensus in the literature which defines chronic renal decline makes it difficult to compare long term outcomes between the various AAA repair techniques. 30 Linsen, et al conducted a meta-analysis (629 patients, follow-up 15-25 months) and concluded the pooled incidence of renal impairment following FEVAR for JAAAs to be 22.2% (95% CI, 16%-30.1%). 33 The reason for renal dysfunction is likely to be loss of target vessel patency over time because of endograft migration, component separation, fracture or in-stent stenosis. 33 Linsen, et al published a graft patency rate of 93.2% at follow up whilst a systematic review by Rao, et al found renal vessel patency to be 95.8% by 5-year follow-up.33,34 However, the observed renal decline at follow up in these 2 studies was 22.2% and 19.7% respectively which suggests a disproportionate relationship between loss of vessel patency and renal function decline. This provides evidence for a multifactorial aetiology for long-term renal decline post-FEVAR.
FEVAR has been shown to be associated with improved perioperative renal morbidity in those with chronic renal insufficiency compared to open surgical repair. 24 Haddad, et al.’s study of 72 patients who underwent FEVAR found a significantly greater incidence of adverse renal events (renal artery stenoses, occlusions and haemodialysis) in patients with baseline renal insufficiency (P = .04; odds ratio = 3.3). 32 However, deterioration of >30% from baseline GFR was not significantly different between patients with and without preoperative renal insufficiency. 32 It may well be patients with pre-existing renal dysfunction are susceptible to long term renal decline as a result of FEVAR-induced acute kidney injury (AKI). 35 Therefore, AKI prevention in patients with renal insufficiency is of great importance as considerable morbidity may occur associated with prolonged hospital stays.
Interestingly, Tran, et al.’s study of 110 JAAAs treated with FEVAR found baseline kidney disease to be a significant protective factor against renal decline (hazard ratio .29, P = .032). 30 This counterintuitive finding may have occurred because FEVAR restored any reduced blood flow to the renal arteries (previously compromised by the aneurysm). Also, FEVAR may have also relieved renal artery stenosis and improved perfusion. 30 Further research and haemodynamic modelling are required to explore any impact of AAA anatomy on haemodynamic changes and renal perfusion.
Neurological Complications
The development of neurological injury following FEVAR for AAA repair remains low. Spinal cord ischaemia (SCI) and transient ischaemic attack (TIA) occur infrequently with 1 study of 318 patients finding an incidence of 1.6% and .9% respectively. A further study finding a 0% postoperative incidence of SCI amongst 245 patients treated with F/BEVAR for JAAA. 36 However, Locham, et al 16 found neurological injury to be more common following FEVAR than EVAR (.7% vs .4%, P = .02). The exact mechanism of SCI following FEVAR is likely multifactorial but may be due to occlusion of the intercostal vessels, thromboembolism and perioperative hypotension. 37 1 possibility for the greater incidence of SCI following FEVAR, compared to EVAR, may be because the longer proximal graft fixation in FEVAR is more likely to occlude the artery of Adamkiewicz. This originates from the aorta between the 8th thoracic and 1st lumbar vertebral level in 89% of the population. 38
Graft-Related Outcomes
Long-term durability of EVAR is dependent on the seal between the endograft and proximal and distal aspects of the excluded aneurysm sac. 39 Aortic neck dilatation (AND) is the process where the diameter of the aortic neck where the stent graft is fixed either proximally or distally increases. This is associated with a significantly increased risk of reintervention as type 1a endoleak or graft migration may occur if intervention is not performed. 39 The incidence and impact of AND following FEVAR is not widely reported though it has been evaluated by some recent studies.40-42 Tran, et al report a follow up of 30.3 months and a mean AND at the proximal stent fixation of 3.6 mm. Zettervall, et al similarly report follow up at 3 years with a mean AND of 3.2 mm at the inferior-most renal artery and 2.4 mm at the SMA with no endoleaks seen.40,41 Whilst Tran, et al report no significant late graft failure or any association between AND and type Ia endoleaks, there were only 25 patients followed up for more than 2 years.40,41
The findings of larger studies concerning standard EVAR with long-term follow up data demonstrates the risk of reintervention does not seem to plateau with time. The absence of significant early endoleaks and reintervention following FEVAR should not be interpreted as no ‘late graft failure’ or a reduced need for follow up, regardless of AND status.40,43,44 Interestingly, a third study by Li, et al addresses the incidence of AND, and any impact on outcomes, in patients managed with FEVAR compared with standard EVAR. 42 Device migration, endoleak, mortality and re-intervention was similar between the 2 groups. However, they found a significantly greater degree of suprarenal aortic segment dilatation in patients managed with FEVAR. This might be expected due to the proximal aortic disease that necessitates a FEVAR device to be inserted. Interestingly, there was a significantly less dilatation of the infrarenal aortic neck. 42 They hypothesised that the suprarenal seal zone in FEVAR may be protective for infrarenal AND and could improve remodelling of the excluded aortic sac. 42 Whilst their study did only compare 20 FEVAR and 20 EVAR cases, their findings with respect to AND are consistent with those of Teter, et al who’s comparison of 30 FEVAR and 90 EVAR cases similarly showed a greater suprarenal aortic segment dilatation but significantly less dilatation of the infrarenal neck following FEVAR.42,45 Ultimately, further studies with long term follow up are needed to more accurately characterise and compare long term aortic remodelling following both FEVAR and EVAR.
The incidence of endoleak following FEVAR is of clinical importance owing to the possibility of aneurysm pressurisation occurring after exclusion. Meta-analysis has estimated the incidence of type I and III endoleaks is 4.9% (95% CI, 2.6%-7.9%) following FEVAR. 15 Whilst endoleak is a common reason for reintervention in the long-term, 15 Swerdlow, et al.’s evaluation of 52 FEVAR cases identified type I or III endoleaks in 54% of cases on post-FEVAR angiography yet found that 96% had resolved spontaneously by the time of post-procedure imaging. 46 Whilst this suggests immediate reintervention for endoleaks may not always be necessary, Swerdlow, et al.’s findings have been criticised. Upchurch warned against patients leaving the endovascular suite after intervention with a known and uncorrected type I or III endoleaks. 47 The incidence of graft migration is not well reported in systematic reviews of outcomes, though it is a recognised cause of reintervention following FEVAR. 15
The need for reintervention is significantly higher post-FEVAR compared to post-OSR (11.1% vs 2.0% late reintervention rate). However, there is a notable bias in both the definition and recording of late reinterventions in both FEVAR and OSR. 15 Long-term follow up of patients post-OSR is significantly less common compared to FEVAR and may lead to possible under-reporting of long-term complications. 15 Furthermore, the wider sequelae of OSR are not insignificant. Incisional hernias and small bowel obstruction may necessitate further surgical intervention following OSR even if this is not classified specifically as aneurysm-related. 15
Limitations of FEVAR
FEVAR depends on easy availability of an endograft with the estimated manufacturing time being 10-12 weeks for custom-made devices. 48 Long term durability of FEVAR is also yet to be fully elucidated. BEVAR, either with internal or external branches, or in combination with fenestrations as F/BEVAR, could theoretically allow deployment of the bridge stents through brachial access after endograft deployment. 18 This would circumvent certain procedural limitations of FEVAR, such as the cumbersome catheterisation of the caudally inclined visceral vessels. 18
Branched Endovascular Aortic Repair
BEVAR stent-grafts (Figure 3) are deployed either as 1 single graft or as modular units with the branches for the visceral arteries either positioned external to the main body of the graft and then catheterised into the visceral arteries or they can be within the lumen of the graft, and then deployed outward into the visceral arteries using a catheter.
18
Branched stent-grafts have been developed in order to overcome the distance between the graft fenestrations and the branch vessels which may arise from within the aneurysm sac.
49
The branches within the stent-grafts enable perfusion directly into targeted vessels thereby excluding the aneurysm sac.
50
Contemporary branched endografts are included with their name, manufacturer, and approval status in Table 3. (A) Custom-made device with helical branch (solid arrow) and fenestration branch (dotted arrow); (B) Helical branch intended for the provision of perfusion for the celiac artery; (C) Nitinol-reinforced fenestrated branch. Reproduced from Soltesz, et al.
52
with permission from Elsevier. Branched Devices and Their Approval Status. Information was Gathered from the FDA and Manufacturer Websites. FDA: Food and Drugs Administration.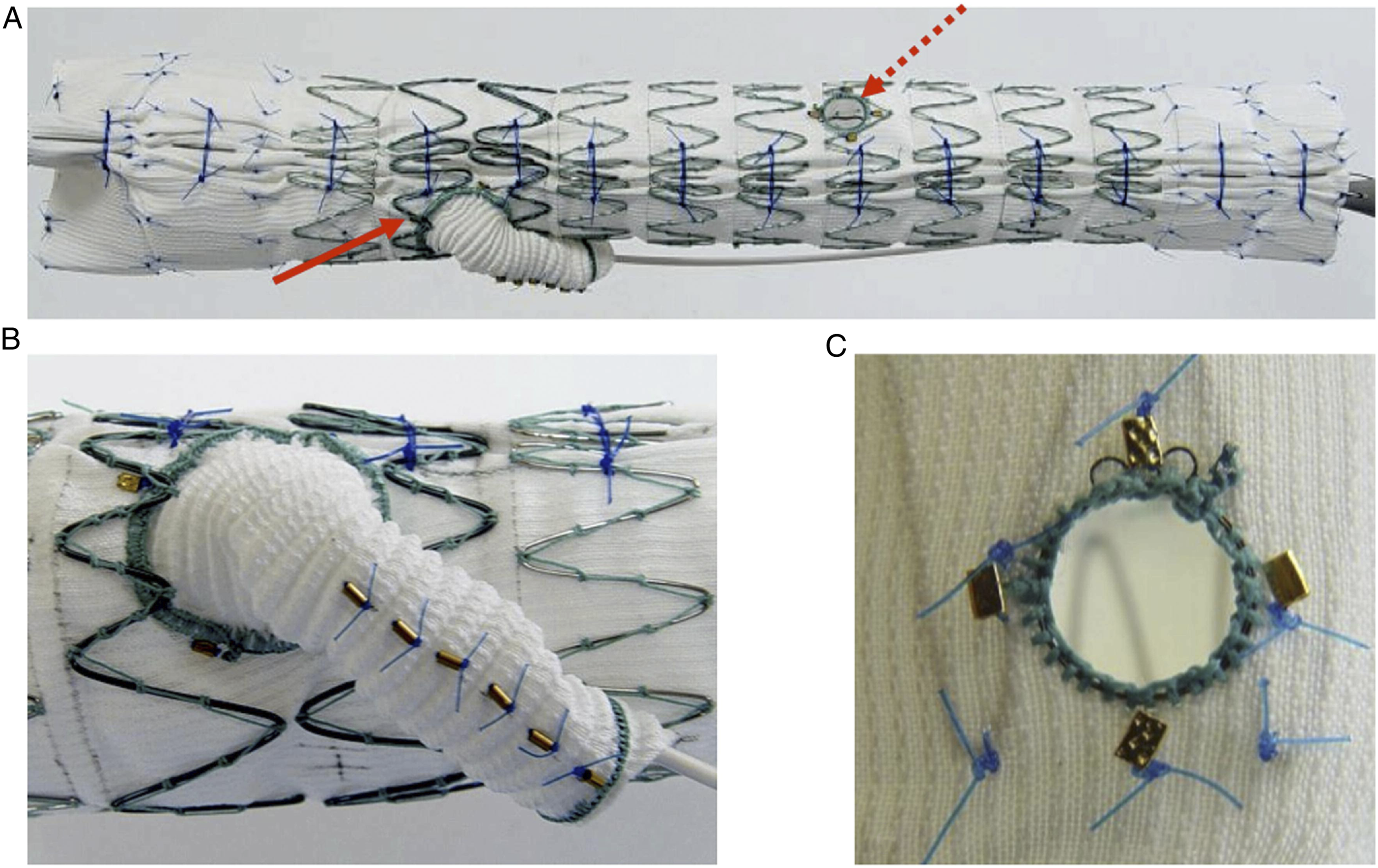
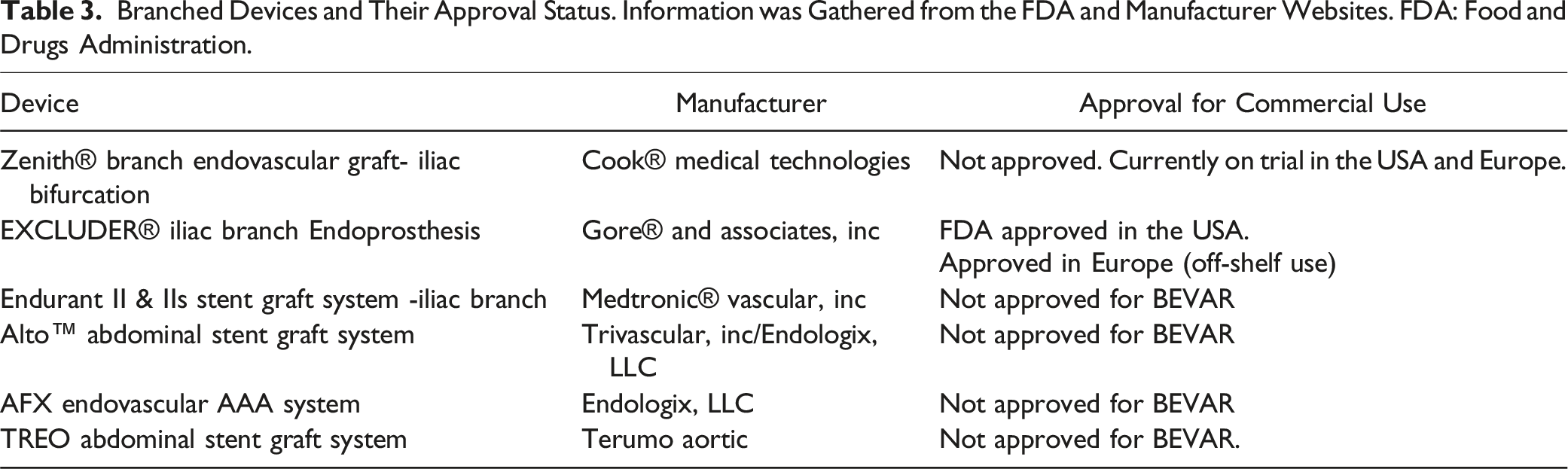
The main indication of BEVAR is thoracoabdominal aortic aneurysms (TAAAs), where 1 or more of the visceral artery origins are included within the aneurysm sac.18,49,51 However, the use of BEVAR is not limited to TAAAs and it has been successfully used to manage suprarenal, juxtarenal and aortoiliac aneurysms.18,49,50 The current literature concerning BEVAR use for AAA is limited as most studies report on BEVAR and FEVAR concurrently, with little focus on the discussion of the differences in clinical outcomes between the 2 modalities. Many studies also discuss the use of both FEVAR and BEVAR for a combination of TAAAs and AAAs, further complicating the analysis of BEVAR. Therefore, the literature reviewed in the section will also include studies which report on F/BEVAR (FEVAR and/or BEVAR), which is relevant to the scope of this paper. A summary of interventions and outcomes in studies reporting on F/BEVAR is provided in Table 2.
Perioperative Outcomes
Budtz-Lilly, et al studied the outcomes of 71 patients who received FEVAR (n = 47) or BEVAR (n = 24) for juxtarenal, pararenal and TAAAs. 53 The 30-day mortality was 2.8% and 90-day mortality 9.9%. 53 However, mortality rates were not available specifically for patients who had undergone BEVAR for AAA. 54 The results are similar to another study which reported a F-BEVAR 30-day mortality rate of 4.9% (23/468) among patients with TAAAs and pararenal aneurysms. 55 Elsewhere, 30-day mortality was lower at only .8% (2/264) in patients undergoing F/BEVAR for juxtarenal/pararenal aneurysms and TAAAs. 19 In a study of Medicare patients in the USA, BEVAR (n = 2143) had an in-hospital mortality of approximately 3%, whilst standard EVAR (n = 16,362) had an in-hospital mortality of approximately 2% (of 16,362 patients). 56
Renal Outcomes
It is known that post F/BEVAR, a decline in renal function occurs in a minority of patients, specifically eGFR decrease and AKI development. 57 A monocentric study by Martin-Gonzalez, et al compared 225 patients undergoing both FEVAR (n = 187) and BEVAR (n = 38). The majority of the aneurysms were juxtarenal or pararenal (67.5%),. 57 Out of a total of 427 renal target vessels, 53 were perfused by branched grafts and the rest by fenestrated grafts. In both FEVAR and BEVAR groups, a significant decrease in mean eGFR was observed post-operatively at 1, 2 and 3-years during follow-up (19.9%, P < .0001; 21.1%, P < .0001; 14.3%, P = .02; respectively). Four 30-day renal events (1.9%) were observed (intraoperative), all in the FEVAR group. Moreover, 29% of patients were observed to have post-operative acute renal failure (decrease in eGFR >25% 48-72 hours post-procedure); (FEVAR = 29.7% vs BEVAR = 37.8%; P = not significant). However, there was no significant difference, overall, between renal outcomes in FEVAR and BEVAR groups, except for renal artery angulation.
Sailer, et al reported that, among 157 patients who had received F/BEVAR for the management of complex aortic aneurysms (juxtarenal, suprarenal and TAAAs), 28% developed post-EVAR AKI which is similar to the results reported by Martin-Gonzalez, et al. 58 Post-EVAR AKI was found to be associated with a significantly increased risk of decreased eGFR at both discharge (P = .001) and at follow up (P = .001) when compared to those not developing post-EVAR AKI. Long procedure times and accessory renal artery occlusions were independent risk factors for post-EVAR AKI but there was no distinction between the patients managed with fenestrated and branched grafts This meant the possible impact of the stent graft used could not be elucidated from this study. 58
Graft-Related Outcomes
Specific technical complications of F/BEVAR include type 1 and 3 endoleak, stent-graft migration and target vessel occlusion. 59 Tsilimparis, et al reported that the F/BEVAR had a significantly decreased risk of overall postoperative complications compared with OR (OR: 42%; F/BEVAR: 19%; P < .001). 19 However, the F/BEVAR group showed a significantly decreased risk of cardiovascular (P < .001) and renal complications (P = .001).
Stent-graft migration and instability is a concern in F/BEVAR grafts, Budtz-Lilly, et al found 88.6 ± 6.4% freedom from branch instability at 3 years in the BEVAR group vs 94.6% for FEVAR. 53 Another study focusing on component separation of the stent-grafts found that 13% (14/106 total) of patients who had undergone either FEVAR or BEVAR were identified as having component movement. This was defined as a movement of a graft component by more than 10 mm. 60 Twelve fenestrated and 2 branched were identified, which appears to contradict the results from Budtz-Lilly, et al. It is also noteworthy that endoleak events occurred in 50% (7/14) patients that had component movement, whilst 22 occurred in patients which had no evidence of component movement (n = 92).
Budtz-Lilly, et al 53 found all of the occlusions occurred in the BEVAR group. Of the 62 patients who participated in imaging during follow-up, 12 cases of type 2 endoleak were identified at 1 month (8 FEVAR; 4 BEVAR). The follow-up period was 46 months and the cumulative branch patency was 92% with all occlusions occurring within the first year post-EVAR. One type 1 endoleak and 7 type 2 endoleaks were also observed. Konstantinou and colleagues found that 10 of 38 patients (26%) presenting with post-F/BEVAR renal artery occlusion went on to require permanent haemodialysis. 61
Limitations of BEVAR
Spinal cord ischemia is a risk factor for all aortic-stenting procedures, particularly when grafts are positioned suprarenally. 59 Spanos, et al studied 243 patients who were treated 62 with FEVAR (67%, n = 163) or BEVAR (33%, n = 80) for TAAAs (n = 126) and pararenal aneurysms (n = 117). 63 In total, 43 patients were identified as developing SCI, 60% of whom were managed with FEVAR and 40% with BEVAR. Though no statistically significant association between EVAR and SCI incidence was seen, there was a higher tendency for SCI for the BEVAR group (21.5% vs 16%, P = .27) within a period of 30 days post-operatively. Similarly, a tendency between SCI incidence and aneurysm type (pararenal: 12.8% vs TAAA: 22.8%, P = .65) was observed. This finding is further supported in a study of 877 patients admitted with TAAAs, AAAs or aortic dissections by Heidemann et al. who found that the incidence of SCI was higher in patients treated using F/BEVAR for TAAA than in patients treated with F/BEVAR for AAA (10.7% vs 3.0%, P < .001). 64
Endograft Categories
Current FEVAR and/or BEVAR endografts can be classified into 3 categories: Off-the-shelf endografts, Physician-modified devices (PMDs) or Custom-made devices (CMDs).
51
The 10-12 week manufacturing time for FEVAR CMDs means that in the acute setting of impending or ruptured AAA, surgical options of patients with complex infrarenal aortic trunk anatomy are limited.
48
However, this group may benefit from physician-modified FEVAR devices (PMD), which are non-fenestrated endografts. However, they have been modified into fenestrated endografts to enable intervention in those who would otherwise be managed palliatively.48,65-67 CMDs are individualised according to the patient’s anatomy. The fenestrated Anaconda stent-graft (Terumo Aortic, Inchinnan, UK) (See Figure 4) has been used with excellent technical success to treat complex AAA. The development of such fenestrated stent-grafts expands the use of EVAR as it addresses the common issues which prevents the use of standard stent-grafts. These are specifically aneurysms with proximally angulated or short necks, visceral artery involvement and poor vessel access.
18
Customised fenestrated Anaconda cuff with augmented proximal ring configuration. Reproduced from de Niet, et al.
73
with permission from Elsevier.
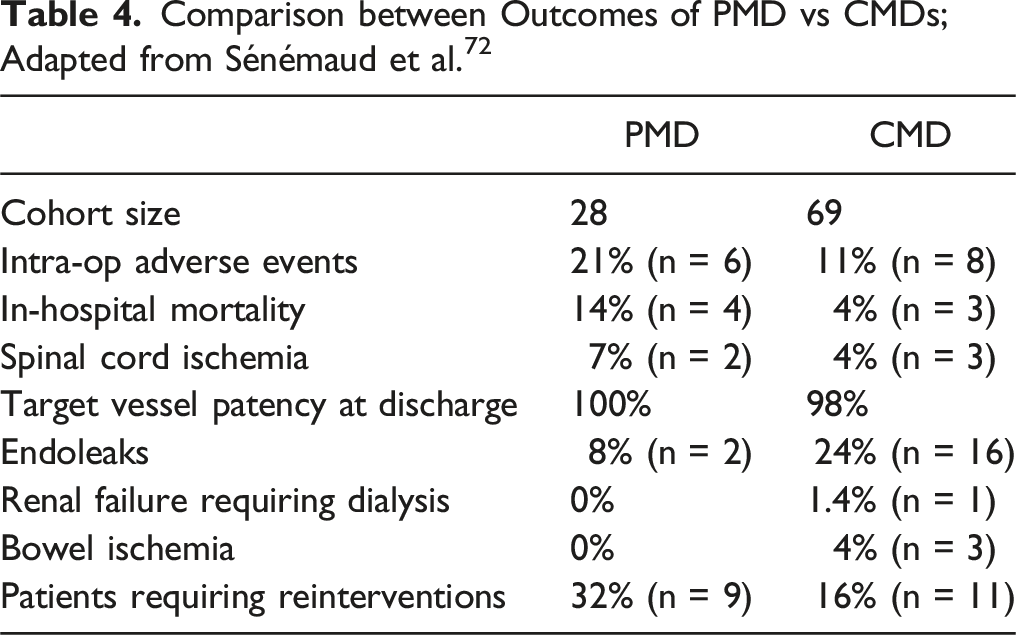
The use of PMDs for certain aortic pathologies appears safe and effective, especially in acute clinical scenarios. 68 A recent systematic review on the application of F/BEVAR (23 studies, 308 patients) for pararenal aneurysms or TAAAs reported that only 24 cases (12.8%) of major adverse events occurred in patients with PMDs (95% CI 8.6% - 18.7%). Overall, treatment success rate was 91.4% amongst patients treated with PMDs. 69 A further systematic review (20 studies) evaluated the clinical outcomes of PMDs for multiple aortic conditions (TAAAs, aortic arch pathologies, complex abdominal aneurysms). 70 For AAA, there was a 30-day mortality of 7.7% with a technical success rate of 87.5-100%. A similar systematic review (20 studies) found comparable clinical outcomes of PMDs for TAAAs and complex AAA. 135 cases of major adverse events out of a total of 832 cases were reported (15.5%; 95% CI 10.8% - 20.8%). Specifically, for type IV TAAAs and complex AAA, 30 day mortality rate was 1.6% (95% CI 0.2% – 4.0%) and the technical success rate was 99.4% (95% CI 97.5% – 100%). 70 These findings validate the use of PMDs in clinical scenarios where other modes of treatments are unavailable. Technical success was also 100% in another 2021 study by Branzan, et al, 71 which included 19 high-risk patients who had undergone FEVAR with PMDs for pararenal aneurysms (n = 8) and TAAAs (n = 11). 30-day mortality was reported at 0%. 71 Reintervention rates were also minimal; only 1 non-aneurysm related death was observed, and the rate of all-cause reinterventions was 10.6% (n = 2) over the 14.4 months mean follow-up period (1-52 months). Nonetheless, evidence seems to suggest more favourable outcomes when using CMDs over PMDs.
Comparison between Outcomes of PMD vs CMDs; Adapted from Sénémaud et al.72
Summary of Results Reporting on the Clinical Outcomes of PMD and CMD.
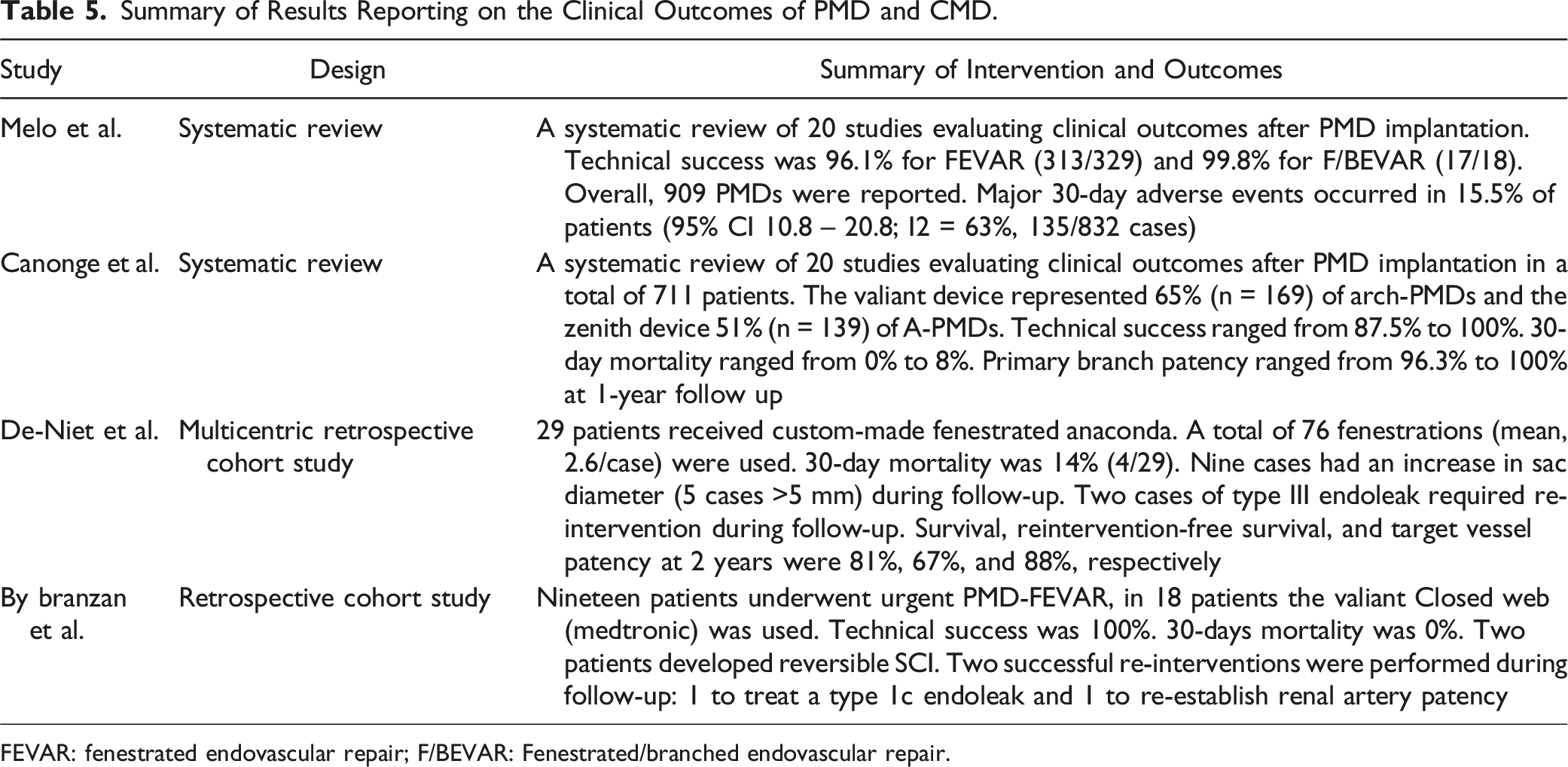
FEVAR: fenestrated endovascular repair; F/BEVAR: Fenestrated/branched endovascular repair.
Conclusion
FEVAR has been well-described over the past decade and offers an effective alternative treatment for patients with complex aortic anatomy who would otherwise be managed with OR or even treated conservatively. At present, the largely unexplored long-term device durability and development of renal complications are the primary concerns for FEVAR. The evidence on BEVAR for AAA is less clear as reported outcomes are usually combined with TAAA repair, which is the most common indication for BEVAR. There is little data comparing outcomes of FEVAR and BEVAR, possibly due to different anatomical indications and surgical preference. F/BEVAR is well defined, representing a progressive uptake of individualised approaches to complex AAA. Custom made devices, particularly Anaconda, are appropriate treatment options which share low short-midterm morbidity and complication rates. In future, RCTs are desirable for unbiased comparison of FEVAR and BEVAR. Longer term studies are also warranted to better understand the durability of these independent strategies. CMDs seem to yield optimal immediate and midterm outcomes and these endografts are expected to increase in popularity as costs and manufacturing times are progressively reduced.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.