
Abstract
A 70-year-old male with a history of 3 prior median sternotomies and on anticoagulation presented with acute chest and back pain associated with a pseudoaneurysm of the ascending and aortic arch in the setting of residual dissection involving the innominate, proximal right carotid, and subclavian arteries. A physician-modified triple vessel fenestrated-branched arch endograft was deployed. The innominate branch stent was deployed from the right carotid cut down, while the left carotid and left subclavian branch stents were placed from a femoral approach. Postoperatively, the innominate branch was found to be deployed in the false lumen of the dissected native innominate artery, leading to continued pressurization of the pseudoaneurysm. This was rescued by placing a Gore Iliac Branch Endoprosthesis (IBE) into the innominate branch through a temporary conduit sewn to the right carotid artery with a right subclavian branch placed via a brachial artery cut down into the internal iliac gate. The use of IBE allowed branch stent extension past the dissected native vessels. The patient had an uneventful recovery without neurologic complications. At 3-month follow-up, the patient remains well with an excluded pseudoaneurysm, and patent bifurcated innominate, bilateral carotid, and subclavian artery branches. A Gore IBE can be utilized in a dissected innominate artery to create an innominate branch device during fenestrated-branched endovascular arch repair.
Keywords
Introduction
Open total aortic arch reconstruction is considered the gold standard for aortic pathologies involving the ascending, aortic arch, or both. While this operation provides the most definitive solution at the proximal extent of the disease, not all patients are physiologically fit to undergo an open repair. Open aortic arch repair with a frozen elephant trunk (FET) is associated with a 30-day mortality up to 15.9%, with aortic dissection, older age, hemodynamic instability, diabetes, and peripheral vascular disease as factors for increased mortality.1-3 Prior history of multiple open aortic operations via median sternotomies resulting in dense scarring can also increase operative risks and mortality.4-6 While thoracic endovascular aortic repair (TEVAR) has become the treatment of choice for descending thoracic aortic pathologies due to low perioperative morbidity and mortality,7,8 endovascular repair of the ascending and aortic arch continues to be refined. The arch branch vessels contribute to the increased complexity of proximal aortic repairs, with dissected branches presenting further challenges in endovascular repair. Investigational arch fenestrated branched devices have been developed for the aortic arch, albeit with limited access in the United States.9-11 Physician-modified endografting (PMEG) technique provides an off-label treatment option for urgent and emergent endovascular aortic repair incorporating the aortic side branches in the thoracoabdominal aorta and the aortic arch. 12 In this report, we describe a physician-modified triple vessel arch fenestrated-branched endograft, complicated by inadvertent false lumen placement of the innominate artery branch stent. This was successfully rescued by deployment of an Iliac Branch Endoprosthesis (IBE) (W. L. Gore and Associates, Flagstaff, AZ), which allowed for bifurcated endovascular distal extension to the undissected right common carotid and subclavian arteries. Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Case Report
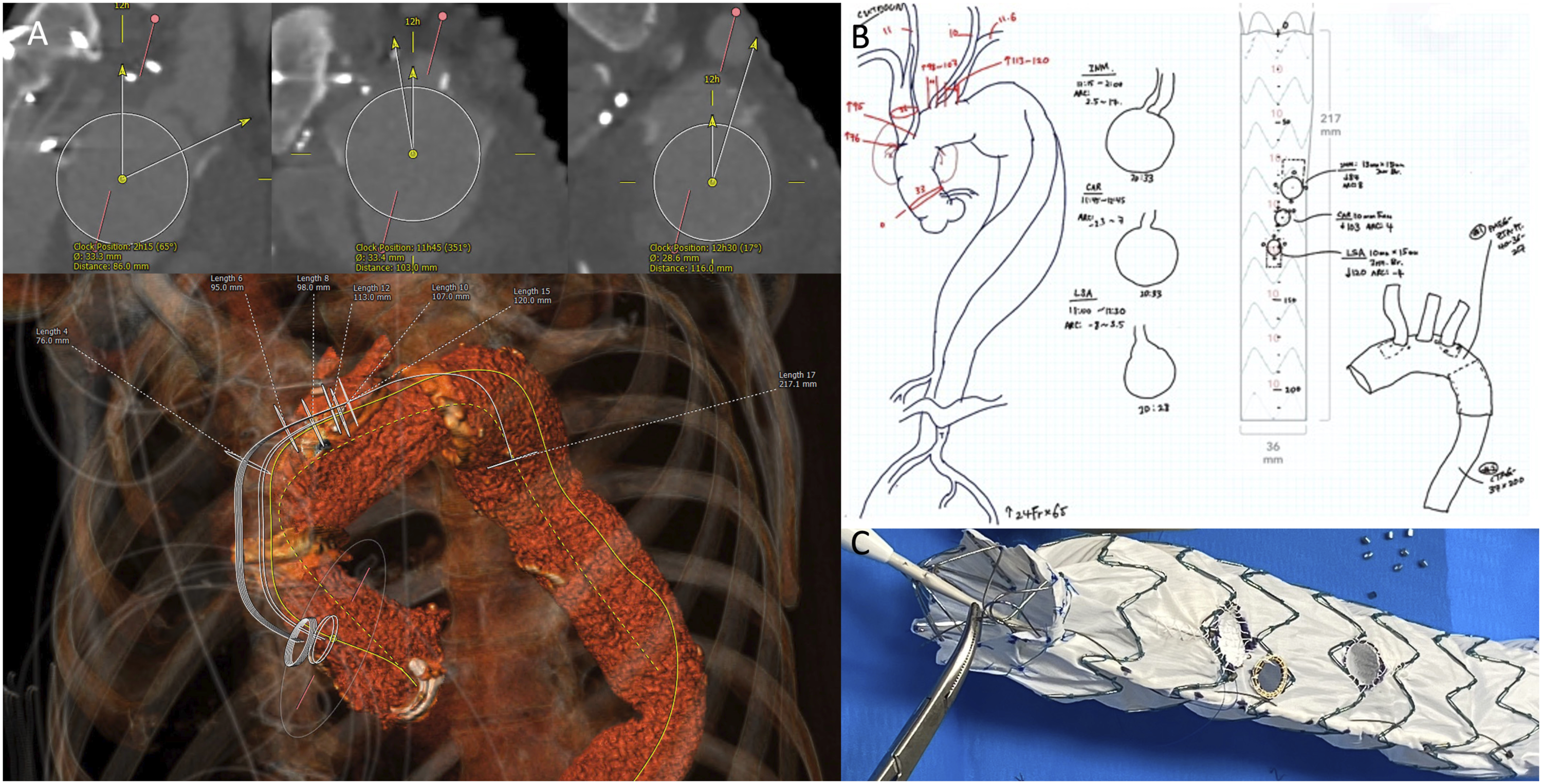
A 70-year-old male with a history of 3 prior median sternotomies, consisting of ascending replacement for a type A aortic dissection 20 years ago, aortic valve replacement for aortic regurgitation a year later, and subsequent total arch replacement with a Carrel patch of all 3 arch branches for an arch aneurysm 10 years ago, presented with acute chest and back pain. The patient also had a history of coronary artery disease, stage 3 chronic kidney disease, and atrial fibrillation on rivaroxaban. Computed tomography angiography (CTA) showed a pseudoaneurysm of the ascending aorta originating at the anastomosis of the prior ascending and arch aortic grafts, and tracking to the arch, dissected arch branches, and abutting the sternum, with residual dissection septum in the innominate artery, the proximal right subclavian and common carotid arteries, and the descending thoracic aorta to the right common iliac artery (Figure 1). Given the multiple previous median sternotomies with loss of the plane between the pseudoaneurysm and the sternum, an endovascular approach was taken. The patient did not meet enrollment criteria for endovascular arch branch trials due to the urgent symptomatic presentation and the innominate artery dissection. Therefore, physician-modified fenestrated-branched arch endovascular repair was performed. Preoperative CTA images were analyzed using a 3-dimensional multiplanar reconstruction software (3mensio, Pie Medical Imaging, Kingdom of the Netherlands). Each of the 3 arch branches was assessed with respect to the longitudinal position measured along the outer curve of the arch, and the arc length measured from the back view of the arch. Based on these measurements, a Zenith Alpha Thoracic proximal tapered endograft (40−36 × 217 mm) (Cook Medical, Bloomington, IN) was modified to include an antegrade inner branch for the innominate artery, a fenestration for the left carotid artery, and a retrograde inner branch for the left subclavian artery (Figure 2). The 2 inner branches for the innominate artery and left subclavian artery are created by suturing beveled self-expanding covered stents to the fenestrations within the lumen of the aortic endograft. This modification technique was previously described.
13
The modified endograft was re-sheathed and flushed with carbon dioxide followed by heparinized saline. The patient’s preoperative anatomy demonstrates (A) pseudoaneurysm of the ascending aorta, (B) dissection of the right subclavian and right common carotid arteries, (C) previous repair with pseudoaneurysm abutting the sternum, and (D) aneurysmal dilation and residual dissection of the descending thoracic aorta. (A) Preoperative anatomic measurements in 3-dimensional multiplanar reconstruction software, (B) preoperative design of the physician-modified branched fenestrated graft, and (C) the modified endograft with an antegrade inner branch for the innominate artery, a fenestration for the left carotid artery, and a retrograde inner branch for the left subclavian artery.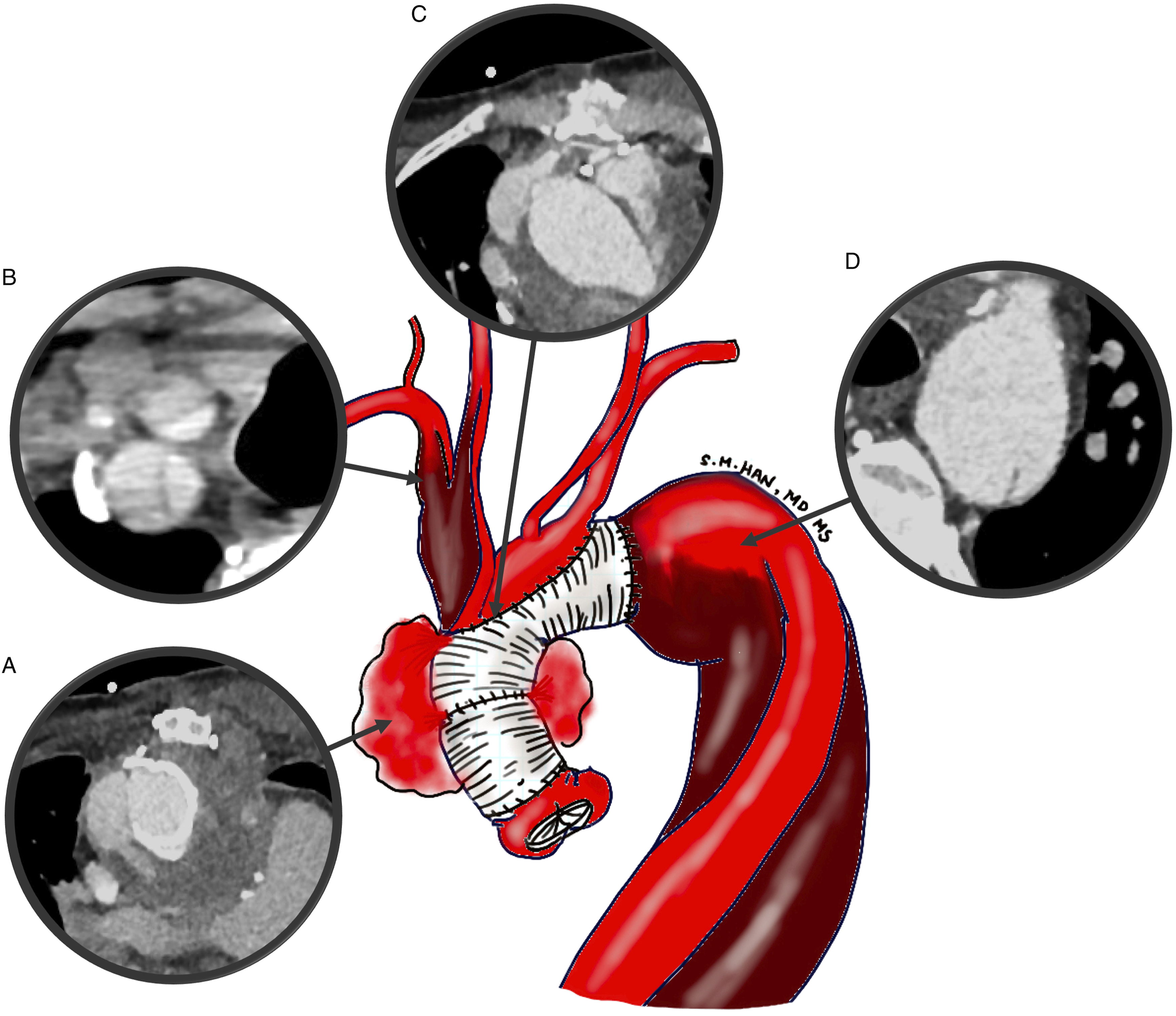
Under general anesthesia, the right common carotid artery was exposed, and percutaneous right common femoral artery access was obtained. Right carotid access was chosen for the innominate branch placement because of the need for a bell-bottom limb. A stiff wire was positioned in the left ventricle, and the physician-modified fenestrated-branched arch endograft was deployed under fusion guidance with rapid ventricular pacing (Figure 3). A distal occlusion clamp was placed on the right common carotid artery, which was then punctured with an access needle in a retrograde fashion. The innominate inner branch was catheterized, and a 20 mm × 10 cm bell bottom EXCLUDER iliac limb (W. L. Gore and Associates, Flagstaff, AZ) was deployed into the innominate artery. The left carotid and left subclavian arteries were sequentially catheterized and stented from the femoral approach using an 8 Fr × 90 cm steerable sheath.
11
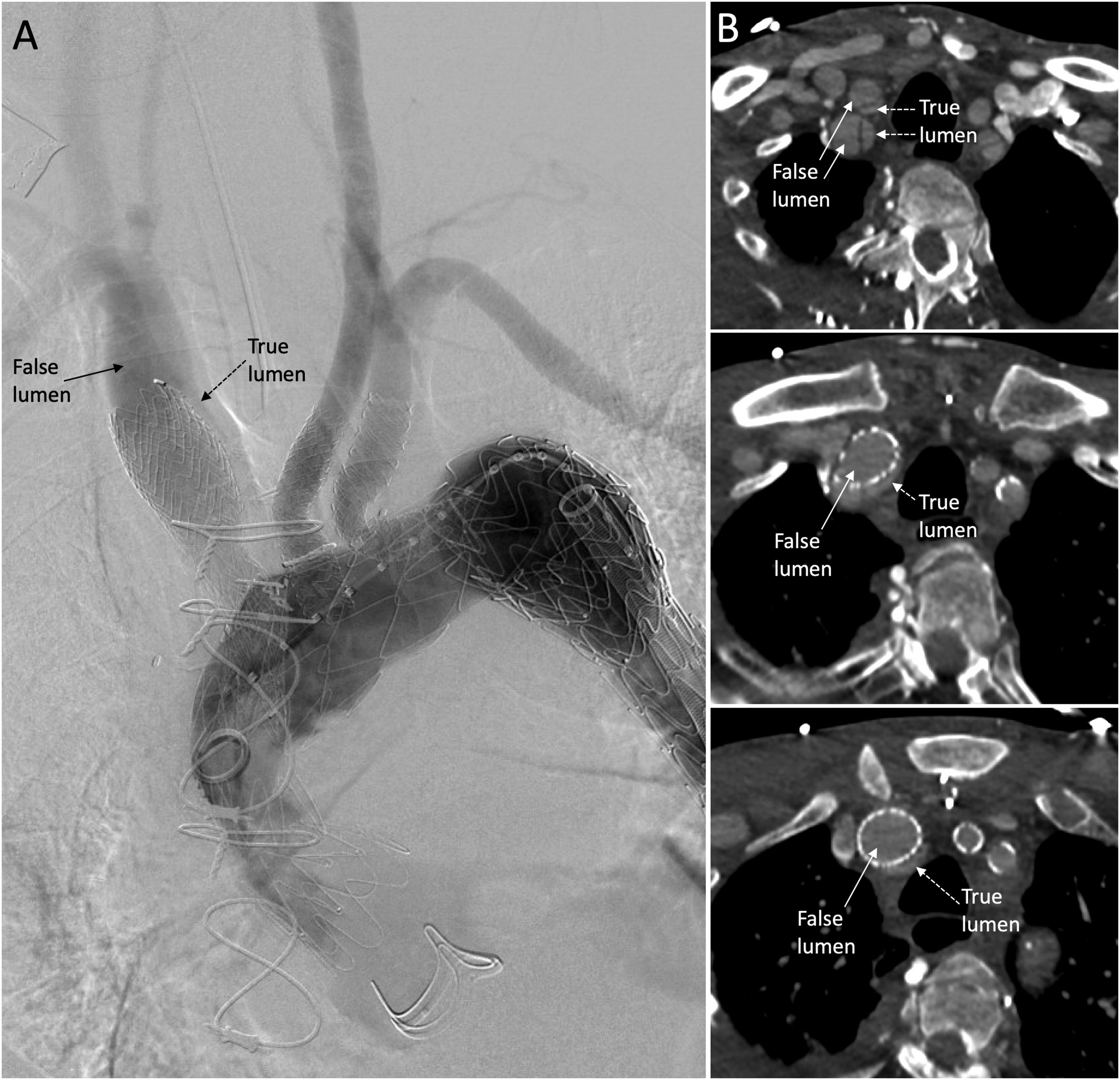
The right carotid artery was flushed prior to primary repair. Operative time was 255 minutes, fluoroscopy time was 55 minutes, and contrast use was 75 mL. The patient awoke from anesthesia without neurologic complications. However, the postoperative CTA showed persistent filling of the pseudoaneurysm due to placement of the innominate branch stent within the false lumen (Figure 4). Deployment of the physician-modified fenestrated-branched arch endograft under fusion guidance with rapid ventricular pacing. (A) Intraoperative fluoroscopy image of the modified branched fenestrated graft with innominate stent in place and filling of the false lumen. (B) CTA series of axial view showing placement of the innominate stent into the false lumen (top-to-bottom moving cranial-to-caudal on the CTA).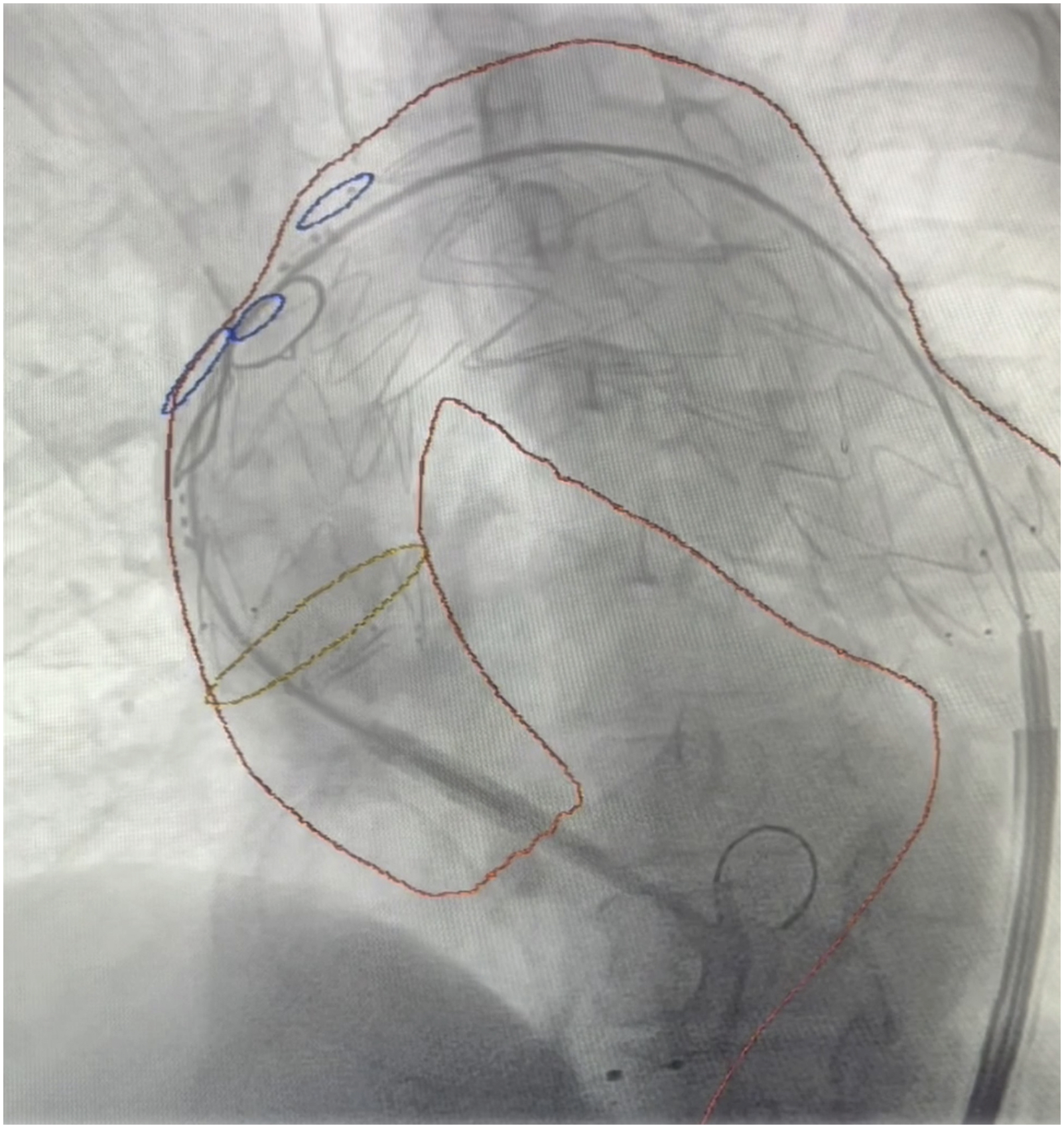
Therefore, the patient was taken back to the operating room with the plan to place an IBE into the innominate artery with the external iliac limb into the common carotid artery and the internal iliac limb into the left subclavian artery. The right carotid artery was re-exposed more distally and open septectomy performed to access both dissection lumens. An 8 mm polyester graft was sewn onto the dissection-free portion of the common carotid artery with an end-to-side anastomosis as a temporary conduit to allow for enough running length for placement of a 14 Fr sheath within the conduit and clamping of the distal right common carotid artery for embolic protection. The right brachial artery was exposed for placement of a 12 Fr sheath for delivery of the iliac limb. The right common carotid and right subclavian artery false lumens were catheterized from each access site, respectively, to access the bell-bottom innominate stent in the false lumen. A 23 mm × 12 mm × 12 cm IBE was introduced from the right carotid conduit and deployed into the previous bell-bottom innominate stent, extending into the right carotid artery through the septectomy and into the true lumen. The right carotid was black bled and flushed prior to removal of the conduit and closure. The internal iliac gate was catheterized from the right brachial access and bridged into the right subclavian artery true lumen with a 14 mm × 10 cm EXCLUDER limb without difficulty (Figure 5). The patient had an uneventful recovery. Postoperative CTA showed patent branch stents and successful exclusion of the pseudoaneurysm. Three-month follow-up CTA demonstrates an excluded pseudoaneurysm and patent bifurcated innominate, bilateral carotid, and subclavian artery branches. (A) CTA coronal view demonstrating extension of the IBE into the right subclavian and right common carotid arteries. (B) 3D reconstruction of the modified endograft and IBE, and (C) illustration of the implanted endografts.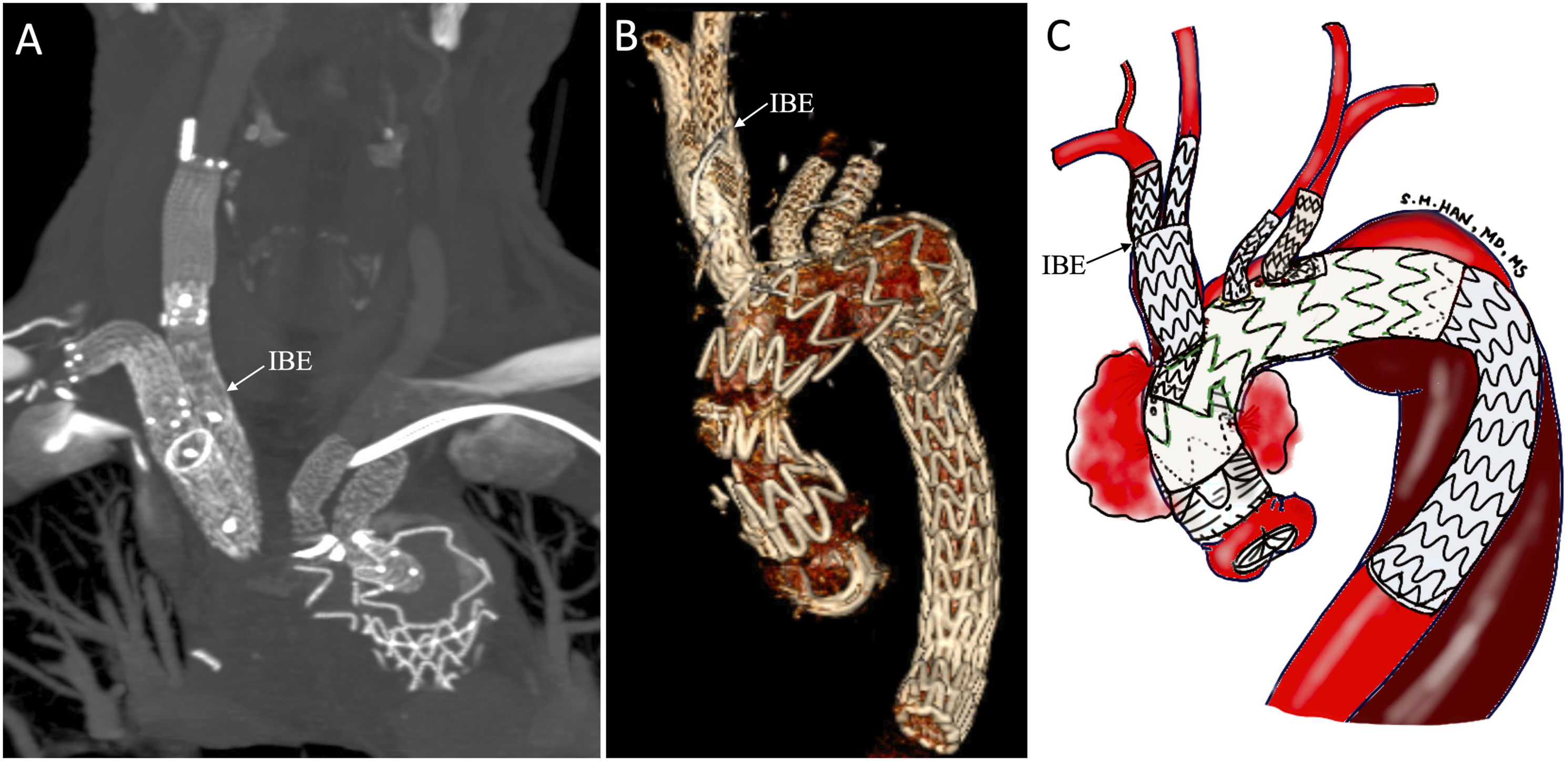
Discussion
Our case illustrates that a physician-modified fenestrated-branched arch stent graft can be utilized to repair an aortic arch with chronic dissection extending into the entire innominate artery. While open arch repair remains the standard of care for aortic arch disease for patients with an appropriate risk profile and a redo repair can be safely performed at high volume centers including ours, this patient was deemed high risk by a team of cardiac surgeons with extensive aortic experience. 14 This was based on the pseudoaneurysm abutting the sternum in the setting of 3 prior sternotomies. Open repair would have required circulatory arrest prior to a fourth-time median sternotomy with potentially lengthy dissection time, which has been associated with higher risk of mortality.4,6 Furthermore, the patient wished to avoid another open aortic operation based on the prolonged and difficult recovery from his last repair. Total endovascular aortic arch repair contains a small but rapidly growing experience that is still largely utilized for patients that are too high risk for open arch repair. 15 Novel devices for hybrid and total endovascular aortic arch repair are being studied in clinical trials, and at the time of this operation, our center was participating in 2 zone zero arch branched device trials; however, the patient’s innominate artery dissection and urgent presentation precluded enrollment in these trials. Device and trial-specific inclusion and exclusion criteria for Gore Thoracic Branch Endoprosthesis and Terumo Relay Branch trials have been previously published.9,16
While dissection of target branch vessels is generally considered a contraindication for fenestrated-branched endovascular repair in both thoracoabdominal and aortic arch repairs,16-18 our initial plan was to place a bell-bottom iliac limb from the carotid approach and perform balloon rupture of the septum, similar to the Knickerbocker technique, while clamping the right common carotid artery for embolic protection. 19 The technical mistake of false lumen deployment of the bell-bottom limb into the innominate artery could have been avoided by paying closer attention to the distal extent of dissection along the right common carotid artery, as well as the use of intravascular ultrasound along the innominate wire prior to branch stent deployment.
Once recognized, the false lumen deployment of the innominate branch required urgent correction since the false lumen was directly pressuring the pseudoaneurysm. We discussed a right carotid to subclavian artery bypass, combined with relining of the innominate branch to the right carotid artery was considered, however, this would have required embolization of the dissected subclavian artery. Also, cervical debranching carries additional risks of complications that are not present during total endovascular repair. 20 The combination of his ectatic innominate artery with the previously placed 20 mm EXCLUDER bell-bottom iliac limb of sufficient length allowed us to consider IBE as a secondary bifurcated bridging stent to the right carotid and subclavian arteries.
Currently, our center has a robust experience of open total arch repair through redo sternotomy with excellent outcomes. Given this, total endovascular arch repair is offered to only a subset of high-risk open surgical patients determined by a multi-disciplinary aortic team consisting of cardiac and vascular surgeons dedicated to aortic pathologies. Open surgical risk is estimated based on advanced age, frailty, multiple prior sternotomies, and severe cardiopulmonary comorbidities such as congestive heart failure, chronic pulmonary disease, and renal failure. Risk of total endovascular repair, particularly of stroke, is assessed based on the aortic tortuosity, arch atheroma or thrombus burden, and integrity of aortic and branch seal zones. Stroke is a major component of morbidity for total endovascular aortic arch repairs, with a stroke rate of 29% demonstrated in a recent study of the Vascular Quality Initiative. 21 Postoperative mortality and endoleak are the next most common complications, while retrograde dissection is a possible but uncommon risk. 22 Device and technique selections are determined with the priorities given for company-manufactured investigational protocols. However, at this time, access to company-manufactured arch branch devices dedicated to total endovascular arch repair remains limited. Physician-modified endografting technique can provide a treatment option in urgent settings for high-risk open surgical patients. Care must be taken to confirm true lumen catheterization of not only the aorta but also for dissected arch branch vessels. Iliac branch endoprosthesis provides a potential secondary bridging stent for the dissected innominate artery during total endovascular arch repair.
Conclusions
Our case illustrates the importance of true lumen catheterization of branch vessels during total endovascular repair of a dissected aortic arch. Furthermore, IBE can be utilized to incorporate the dissected innominate artery by achieving distal seal at the undissected right carotid and subclavian arteries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sukgu M. Han is a consultant for W. L. Gore and Associates, Cook Medical, Terumo, and Vestek, and is on the scientific advisory board for W. L. Gore and Associates and Vestek. Fernando Fleischman is a consultant for W. L. Gore and Associates, Cook Medical, Terumo, and Artivion.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.