
Abstract
Neurogenic thoracic outlet syndrome and superior labrum anterior posterior tears are usually treated in a staged manner due to different post-operative therapy needs. This case describes successful combined surgery with expedited physical therapy.
Introduction
Here we have it: double trouble -- the combination of neurogenic thoracic outlet syndrome (nTOS) and superior labrum anterior posterior (SLAP) tear as the etiology of disabling shoulder pain and arm numbness. While these lesions are typically treated as separate entities, we successfully combined surgery and post-operative physical therapy for this patient.
Case Description
In 2018, a 30-year-old male, who was a former baseball pitcher, injured his right shoulder in a car accident. He was right hand dominant and over the ensuing weeks, he developed numbness in his right thumb, index, and middle fingers. This progressed to significant scapular and arm pain, especially while performing overhead activities. He was ultimately diagnosed with nTOS. Physical therapy was prescribed and initially helped, but his symptoms progressively worsened. He was also evaluated by an orthopedic surgeon and was diagnosed with SLAP tear. A glenohumeral injection relieved his periscapular pain and anterior scalene block relieved the pain and numbness in his hand. He was unable to work as a restorative builder or continue playing baseball due to numbness and weakness in the arm.
On physical exam, he had a large, tender, anterior scalene muscle and point tenderness over the long head of the biceps tendon sheath. He had full passive range of motion and intact rotator cuff strength without signs of impingement. His strength was 3/5 in his ulnar distribution and 4/5 in his radial and median nerve distributions. On abduction, he did not have a subclavian bruit, but did lose his radial pulse. At 15 seconds, his elevated arm stress test was positive as exhibited by numbness and weakness. He also had positive O’Brien’s, Yergason, crank, and dynamic labral shear tests. His cervical spine and left arm exam were unremarkable.
Magnetic resonance imaging (MRI) was obtained (Figure 1). His chest X-ray was normal. MRI without contrast of right shoulder: (a) coronal image demonstrating superior labral tear at the long head of biceps insertion on supraglenoid tubercle, and (b) axial image illustrating posterior labral tear.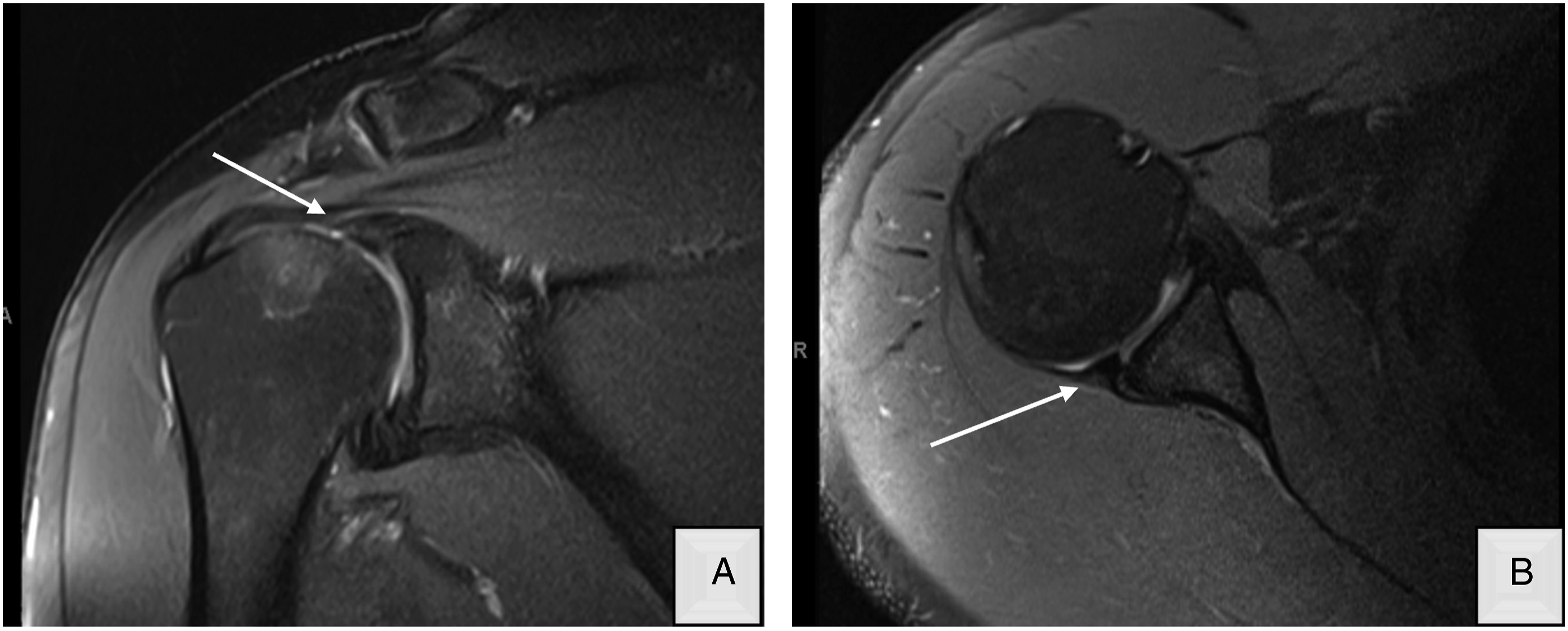
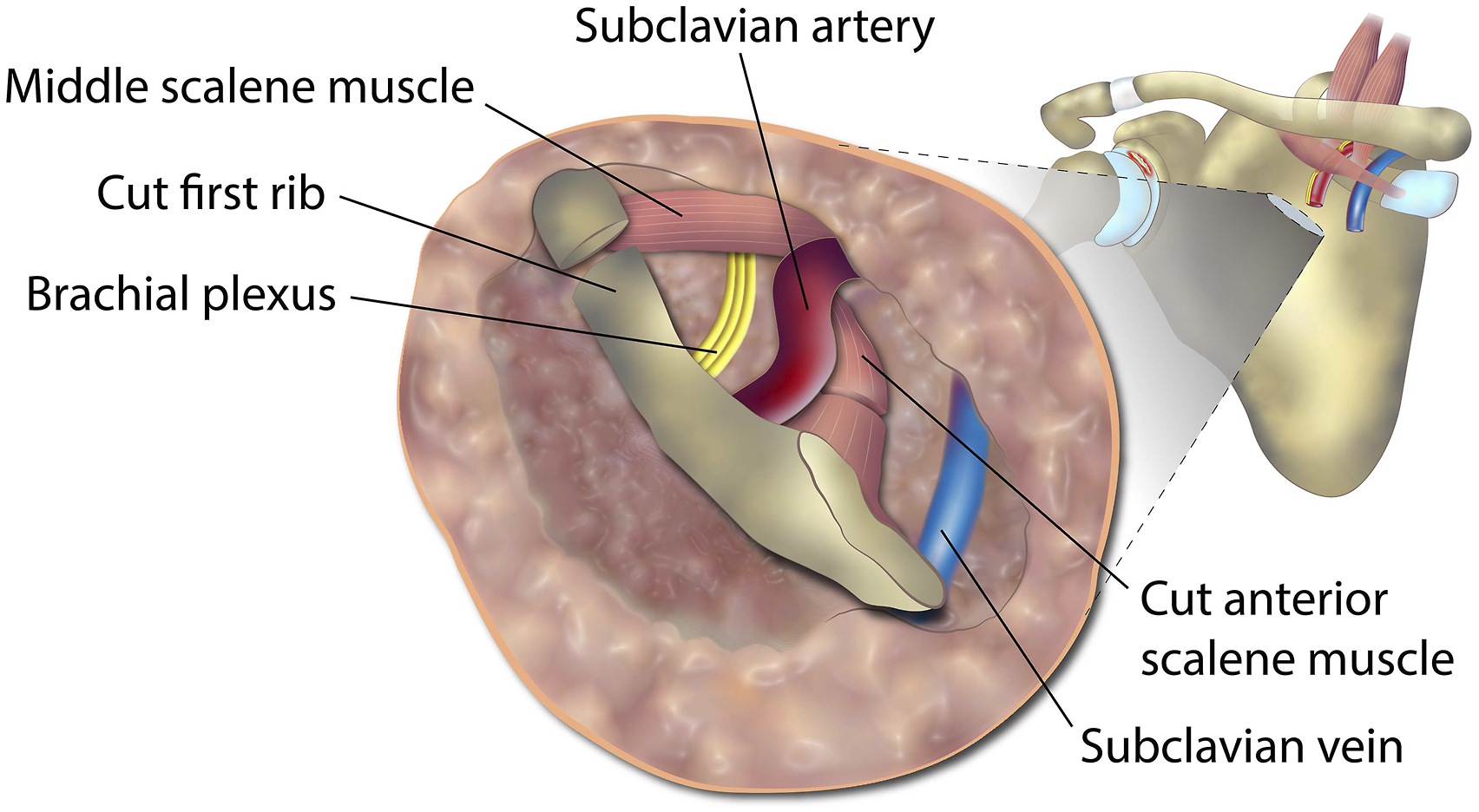
Given our patient’s physical fitness, motivation, and need for simultaneous repair to return to work, we elected to treat both pathologies concomitantly. He underwent transaxillary first rib resection with anterior scalenectomy and shoulder arthroscopy with superior labrum debridement, posterior labral repair, and open subpectoral biceps tenodesis (Figures 2 and 3). Post-operatively, his pain, numbness, hand swelling, headaches and neck pain improved almost immediately. After 4 months, he returned to all activities that he enjoyed pre-operatively. Arthroscopic images of right shoulder (left lateral decubitus position). A and b from posterior portal: (a) type II superior labrum anterior posterior tear tear, (b) superior labrum after debridement and long head of biceps tendon tenotomy. C and d from anterior superior portal: (c) posterior labral tear from 7 to 9 o’clock position, (d) posterior labrum repaired. Transaxillary view of first rib resection and anterior scalenectomy.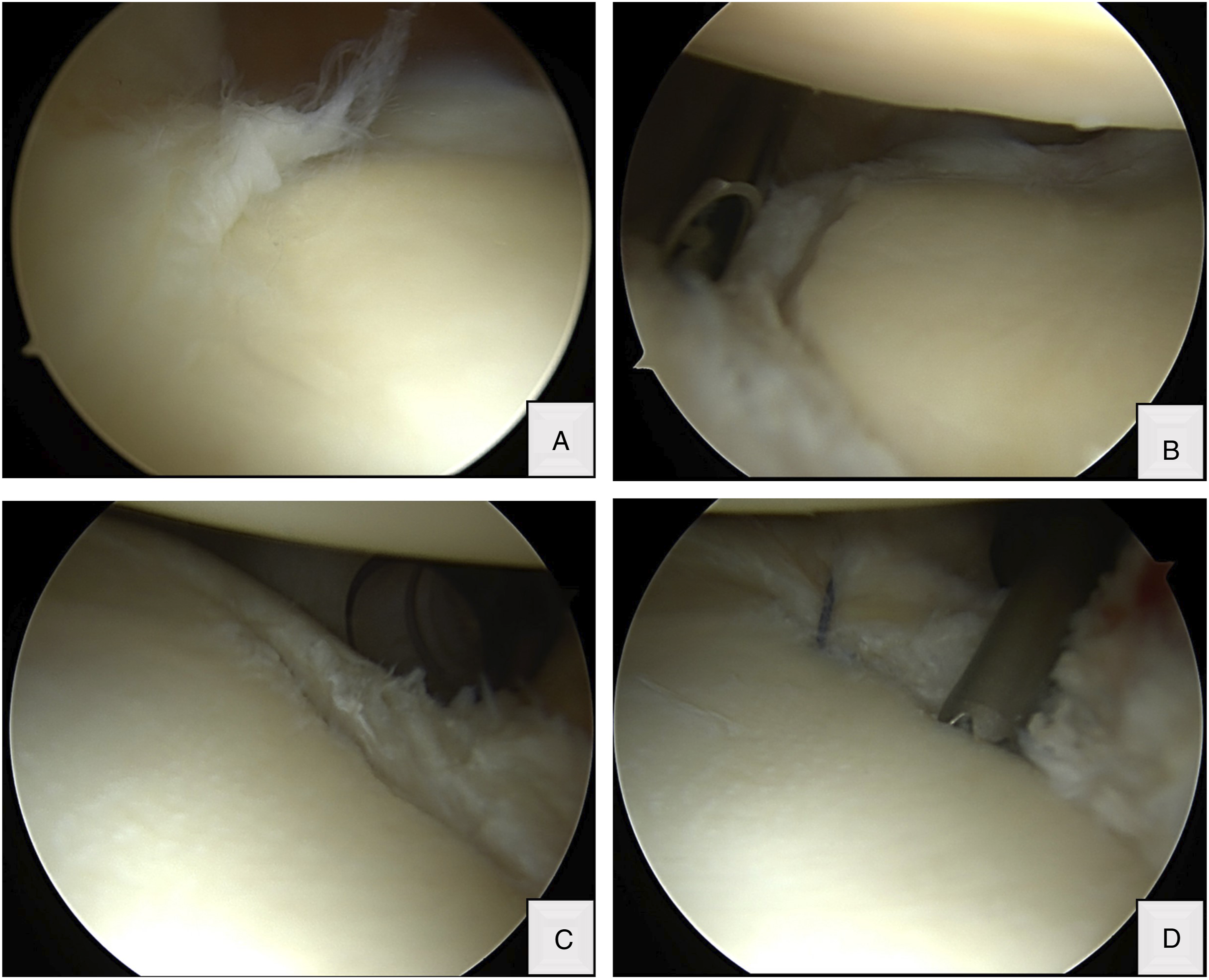
Discussion
nTOS is the most common form of thoracic outlet syndrome and is often diagnosed in patients with a history of head and neck trauma. 1 The brachial plexus nerve roots are impinged as they pass through the interscalene triangle (formed by scalenus anticus and medius muscles and the first rib). 2 In SLAP injuries, the biceps attachment to the supraglenoid tubercle and superior labrum is disrupted. Multiple injury mechanisms have been proposed for SLAP injuries, including forceful traction or compression of the arm in acute traumatic events or repetitive microtrauma as seen in overhead throwing athletes. 3
nTOS is a clinical diagnosis without a single specific history, physical exam, or imaging finding. Symptoms include pain, paresthesia, and weakness in the hand, arm, or shoulder. Neck pain and occipital headaches may be reported as well as Raynaud’s phenomenon. Raynaud’s phenomenon is observed because of overactive sympathetic nervous fibers found on the nerve roots of C8, T1, and the lower trunk of the brachial plexus. Patients have tenderness over the scalene muscle and symptoms provoked by tilting their ear to shoulder. There are several special tests that may assist in making the diagnosis including the modified upper limb tension test of Elvey, Adson’s test, and elevated arm stress test. 2 Similar to nTOS, multiple physical exam findings are described for SLAP lesions, but no single maneuver is sensitive or specific.4,5
Work-up includes a chest xray to evaluate for a cervical rib or anomalous first rib. In athletes, shoulder MRI is obtained, however diagnostic arthroscopy is the most reliable modality to identify SLAP tears and should be reserved for conservative treatment failure. 5 Injection of neuromuscular blocking agent alone, or in combination with, lidocaine or botulinum toxin A into the anterior scalene muscle at its attachment to the first rib is a reliable diagnostic method that can also provide symptom relief.2,6
Initial treatment of nTOS and SLAP lesions should be conservative. Non-operative therapy, followed closely for 8 weeks, is successful in 60-70% of patients. 2 After failure of non-operative management, first rib resection and scalenectomy is successful in providing long-term pain relief and improved quality of life. 7 Treatment of SLAP tears is controversial and often dictated by tear pattern, patient age, and activity level. 8 Multiple studies demonstrate superior results with biceps tenodesis compared to SLAP repair in type II SLAP lesions refractory to non-operative treatment.9,10 Combining first rib resection with posterior labral repair and open subpectoral biceps tenodesis is unique as the post-operative physical therapy regimen is quite different. Briefly, patients undergoing first rib resection begin early mobilization on post-operative day 1. Formal therapy begins 2 weeks post-operatively. Following posterior labral repair and open subpectoral biceps tenodesis, patients are typically immobilized in a sling for 3 to 4 weeks. For this patient, an expedited protocol was used, and he began progressive range of motion exercises after post-operative week 2.
Conclusion
This is an unusual cause of shoulder pain secondary to SLAP tear and nTOS from a car accident, highlighting the value of a broad differential diagnosis and partnership between specialists.
Ethical Statement
Informed Consent
Informed consent has been obtained from the patient for publication of the case report and accompanying images.
Footnotes
Acknowledgments
Artwork created by Jacob Thomas.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board
Institutional review board approval provided by the Wake Forest Institutional Review Board.