
Abstract
Background
This study’s objective is to evaluate the emotional experiences, coping mechanisms, and support resources for Canadian vascular surgeons and trainees following an adverse patient event or near miss.
Methods
This is a cross-sectional survey study of all Canadian Society for Vascular Surgery (CSVS) members from October to November 2021. We collected data on participant experiences with adverse events, their emotional responses, the coping mechanisms used, and their perceptions on available support resources.
Results
The survey was sent to 233 CSVS members yielding 66 responses. The majority (77%) of respondents had experiences with adverse event causing serious patient harm. The most common negative experience following an adverse event included feelings of negativity towards oneself, general distress, and anxiety about potential for future errors. The most common coping mechanism was seeking advice from a mentor or close colleague. Peers (82%) and senior colleagues (59%) were the most preferred sources of support. Most of the respondents would reach out to a mentor if they had 1, but 30% reported no mentor or close colleague for support.
Conclusion
Adverse patient events and near misses have serious negative impact on the lives of Canadian vascular surgeons and trainees. Peers and senior colleagues are the most desired source for support, but this is not universally available. Organized efforts are needed to bring awareness in our vascular surgery community on the ubiquitous nature and detrimental effects of adverse events.
Introduction
Adverse events occur in almost 10% of hospital visits and are recognized to carry a significant psychological burden on the healthcare providers involved.1,2 In a study of all surgeons at 3 major teaching hospitals in the United States, a third of respondents had experienced at least 1 intraoperative adverse event in the last year. 3 There is a significant emotional toll on a surgeon following an adverse event, with the majority reporting anxiety, guilt, and sadness. 3
As defined by the World Health Organization World Alliance for Patient Safety, an adverse event describes “an injury related to medical management, in contrast to complications of disease. Medical management includes all aspects of care, including diagnosis, medical and surgical treatment, failure to diagnose or treat, and the systems and equipment used to deliver care.” A ‘near miss’ describes “a serious error or mishap that has the potential to cause an adverse event but fails to do so because of chance or because it is intercepted.” 4
Physicians impacted by adverse events have been described as “second-victims”, the often forgotten about individual second to the patient themselves. 5 The physician affected can experience increased rates of burnout, increased medical errors, decreased quality of patient care, and increased risks of depression, substance abuse, and suicide.6-8 While studies have investigated this area among physicians more broadly and in some particular specialties, 9 vascular surgeons represent a unique population with the second highest rate of burnout after trauma surgeons, the lowest level of career satisfaction, and the highest incidence of suicidal ideation among surgical subspecialities. 10 A recent survey of all active Society for Vascular Surgery members found that 41% endorse at least 1 symptom of burnout and 37% had symptoms of depression in the last month. 11 Eight percent of vascular surgeons endorsed suicidal ideation within the last year, with self-report of a major medical error being an independent risk factor for suicidal ideation. 11 A recent wellness survey among Canadian Society for Vascular Surgery (CSVS) members confirmed that burnout, depression, and job dissatisfaction are major issues among Canadian vascular surgeons. 12 The objective of this study is to expand on our current knowledge of vascular surgeon wellness in Canada, with a particular focus on their experiences and coping strategies following adverse events and near misses.
Methods
This study is a cross-sectional online survey of CSVS members using their membership database from October to November 2021. CSVS is a national society that includes vascular surgeons and trainees from all across Canada. An invitation email with an embedded link to the survey was sent to all CSVS members. Follow-up emails were sent at 2 and 4 weeks. To encourage participation among trainees, reminders were made in resident social media groups and other platforms. Participants indicated consent through completing and submitting the anonymous survey. No personal identifiers were collected. Institutional approval was obtained by the University of British Columbia Behavioural Research Ethics Board (H21-02633).
Our survey was adapted from the Health Professional Experience of Error Questionnaire (HPEEQ) which is a survey instrument developed and used in similar studies of physicians in the United Kingdom and United States. 13 The survey in our study included a total of 17 questions collecting data on participant demographics, their experiences with adverse events or near misses, their emotional and psychological responses, the coping mechanisms used, and their awareness and perceptions on available support resources (Appendix A).
A brief 3-question survey was subsequently sent to the program directors of all 9 Canadian vascular surgery residency training programs (Appendix B). Outcome measures from this brief survey included the existence of a formal mentorship program for residents, self-reported rating of the program’s level of support for residents following an adverse event or near miss, and a free-text space for additional comments.
Outcome measures with dichotomous data was analyzed using the χ2 or Fisher exact test and is presented as the frequency with percentage. All analyses were conducted with R version 4.1.2. P-values < .05 were considered statistically significant, and all tests were two-sided.
Results
A total of 66 surveys were completed from the 233 distributed among all CSVS members (28% response rate). Out of these respondents, 51 were attending-level vascular surgeons (77%), 1 was a fellow (2%), and 14 were residents (21%). Among the attending surgeons, 59% use a fee-for-service billing format, 37% have a group practice plan or salary, and 4% reported other compensation formats. Most respondents reported high levels of support among their local vascular surgery colleagues: 32% feeling “extremely” supported, 27% “quite a lot” supported, 26% “moderately” supported, 9% “a little” supported, and 6% “very slightly or not at all” supported.
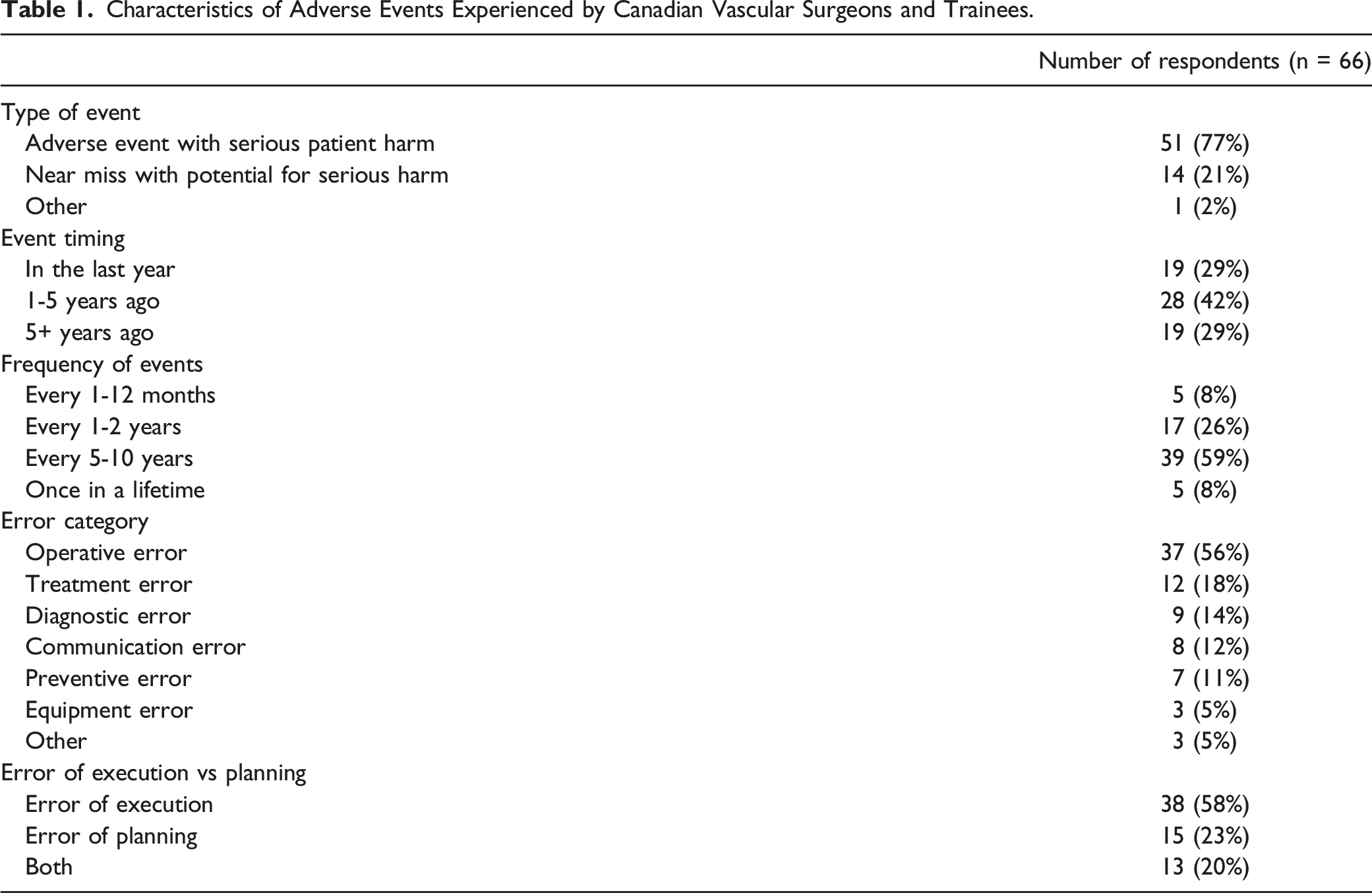
Characteristics of Adverse Events Experienced by Canadian Vascular Surgeons and Trainees.
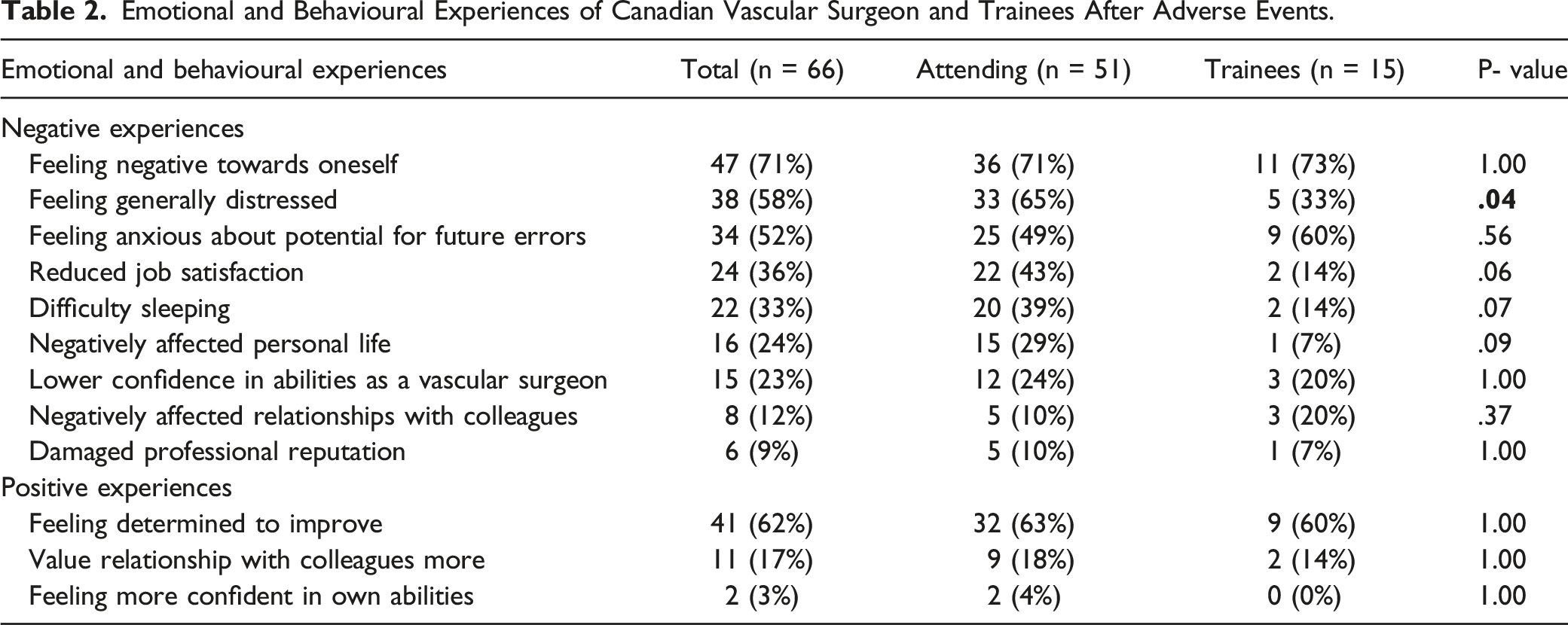
Emotional and Behavioural Experiences of Canadian Vascular Surgeon and Trainees After Adverse Events.
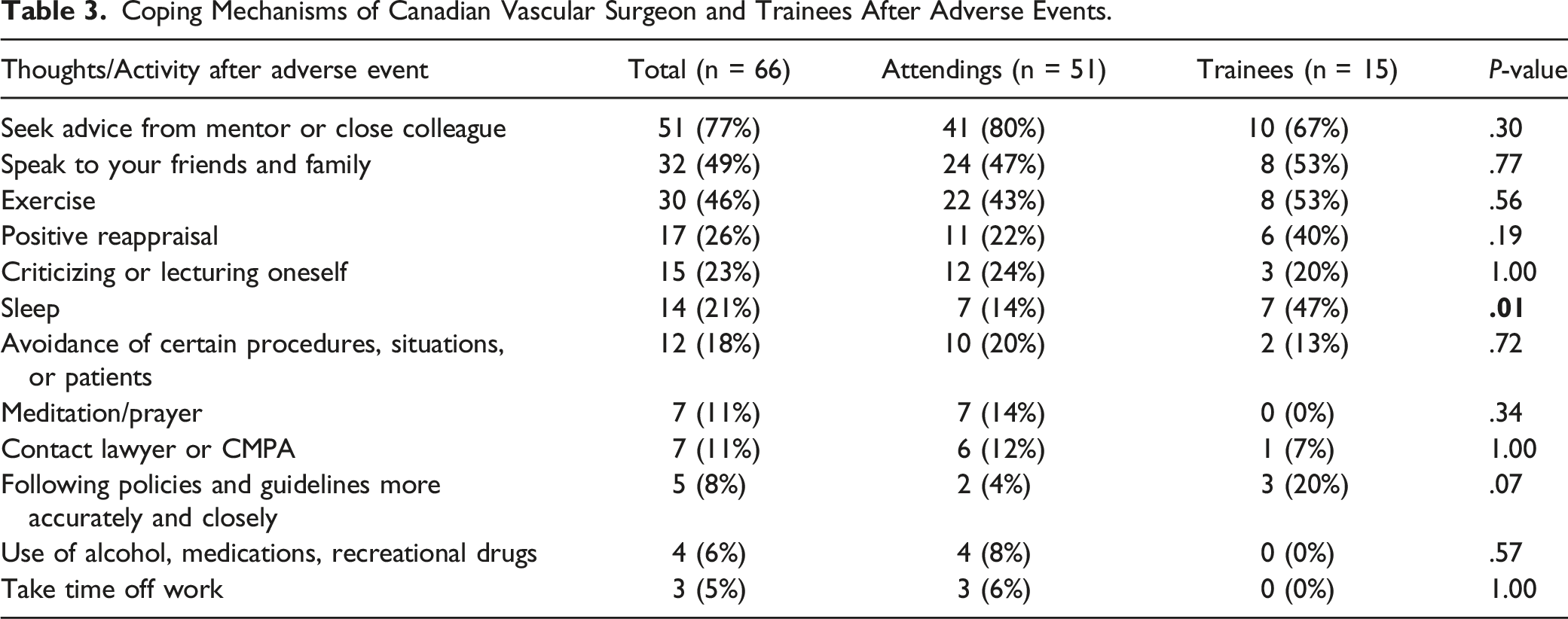
Coping Mechanisms of Canadian Vascular Surgeon and Trainees After Adverse Events.
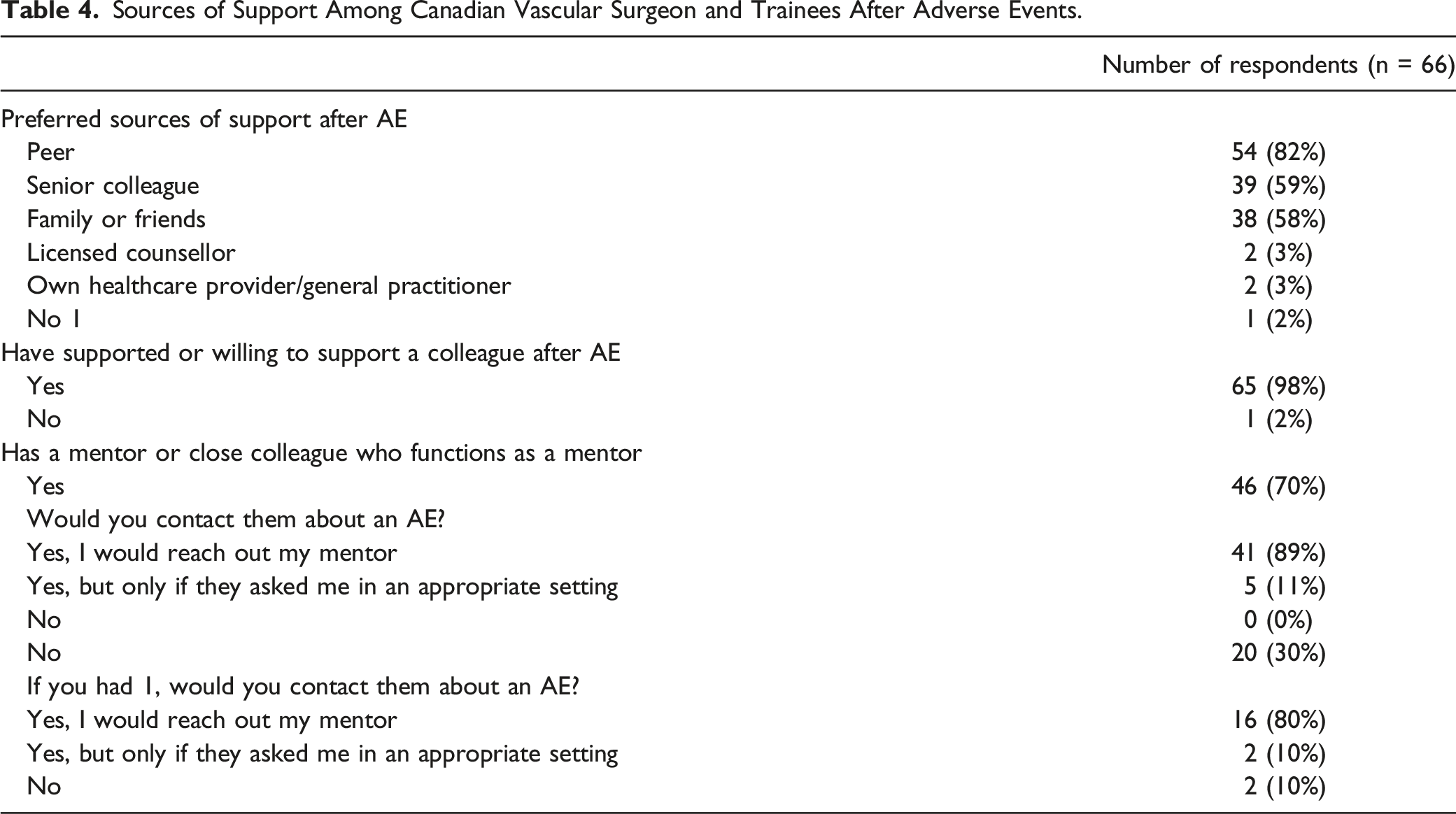
Sources of Support Among Canadian Vascular Surgeon and Trainees After Adverse Events.
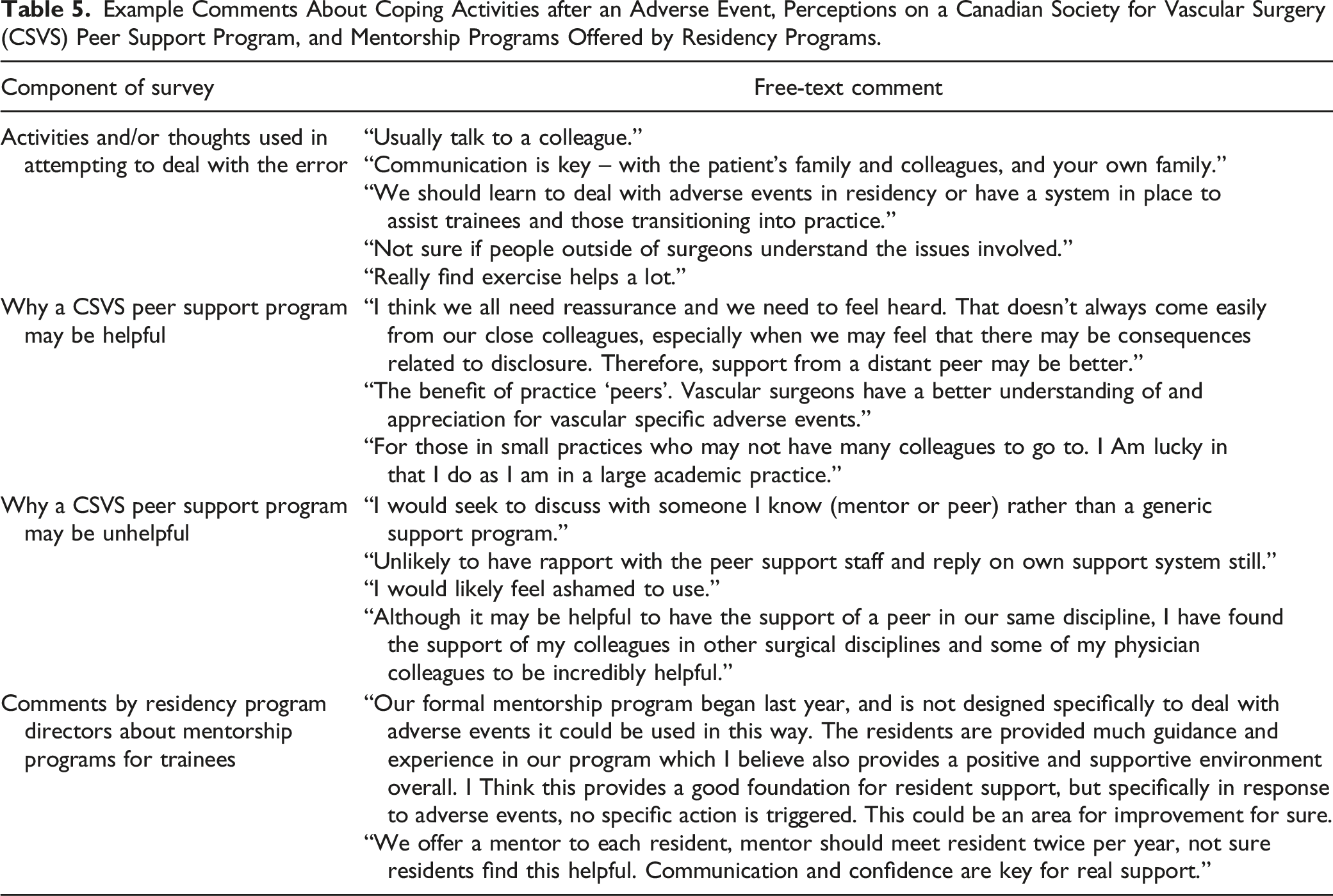
Example Comments About Coping Activities after an Adverse Event, Perceptions on a Canadian Society for Vascular Surgery (CSVS) Peer Support Program, and Mentorship Programs Offered by Residency Programs.
Comparison of Survey Responses Between Attending Vascular Surgeons and Trainees, and Those With a Mentor/Close Colleague Equivalent and Those Without.
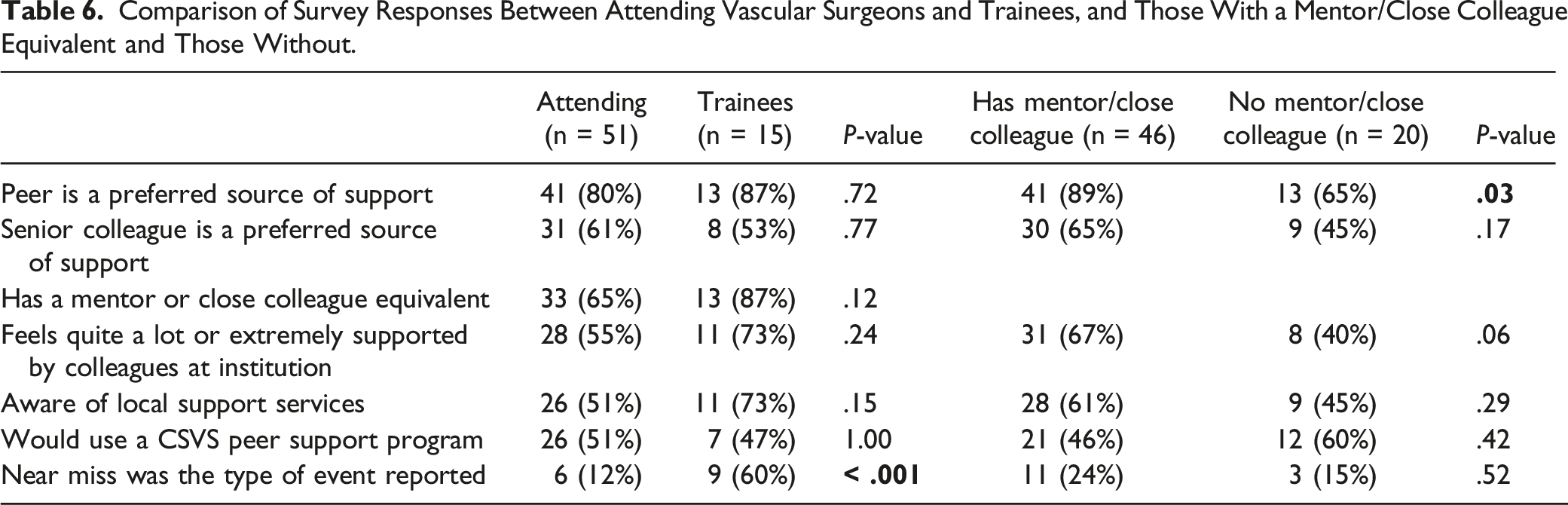
Responses were also analyzed for any differences between those who indicated that they have a mentor or close colleague equivalent, compared to those that do not. Those with a mentor or close colleague equivalent had a greater preference for peers as a source of support (89% vs 65% among those without a mentor, P = .03). Otherwise, there were no statistically significant differences in emotional and behavioural experiences, coping mechanisms, or other responses. Additionally, an analysis was performed among staff surgeons with fee-for-service (n = 30) compared to group practice plan or salary (n = 19) compensation formats. There were no statistically significant differences in any of the analyzed items including preference for peer or senior colleague support, having a mentor, feeling quite a lot or extremely supported by colleagues, being aware of local organized support services, or willingness to use a CSVS Peer Support Program.
Among the 9 vascular surgery residency training programs in Canada, 6 program directors completed the supplemental brief 3-question survey (67% response rate). Four programs (67%) indicated that they have formal mentorship support programs for residents. The level of support provided to residents for dealing with the stress of adverse events were reported to be “extremely supported” by 1, “quite a lot supported” by 3, and “moderately supported” by 2. Comments about the mentorship programs and level of support for residents are provided in Table 5.
Discussion
We describe the experiences of Canadian vascular surgeons and trainees following a medical error, with all respondents reporting either an adverse event resulting in serious patient harm or a near miss with the potential for serious harm. In a study of over 1.4 million vascular surgery procedures, 5.2% of patients experienced an adverse event during their hospital stay. 14 Vascular surgery encompasses a wide variety of procedures with the high potential for periprocedural complications or serious patient harm, placing providers in a uniquely vulnerable position to be impacted as “second victims.”
The study of emotional and behavioural responses following adverse events among physicians and healthcare providers generally are well-documented. In a cross-sectional survey of 265 physicians and nurses from the United Kingdom and United States, negative emotions such as anxiety, distress, guilt, and self-doubt were prevalent. 13 A third of the respondents reported that their personal lives were affected as a result of the medical error, and that the event also strained colleague relationships at work. 13 A recent meta-analysis of 18 studies reporting on the psychological and psychosomatic symptoms of over 11,000 physicians as “second-victims” found that more than two-thirds of respondents experienced troubling memories, anxiety, anger, remorse, and distress. 2 Unsurprisingly, our cohort reported similar detrimental emotional and behavioural experiences with more than half feeling negative towards themselves, generally distressed, and anxious about potential future errors. In comparison to the survey from the United Kingdom and United States, 13 our sample reported slightly lower rates of negatively affected personal lives and relationships with colleagues (24% and 12%, respectively).
Positive experiences such as a determination to improve were reported by 62% of respondents, reflecting a motivating factor that can be harnessed to learn from one’s experiences given the appropriate mindset. This positive outlook, as well as other experiences such as feeling more attentive or more confident, have been demonstrated among other similar studies.9,13,15 Following an adverse event, the literature describes the natural history of recovery for a healthcare worker consisting of 6 stages. 16 The last stage, “moving on”, has 3 possible paths: dropping out, surviving, or thriving. Effective coping mechanisms and support systems are necessary in facilitating healthcare workers to thrive in the aftermath of adversity.
The findings of our survey in the vascular surgery community support the notion that the most preferred coping mechanism is peer support. A study of surgeons, emergency physicians, and anesthesiologists from an American tertiary-care centre demonstrated that 88% identified talking to another physician as the preferred source of support over traditional mechanisms such as employee assistance programs or mental health professionals. 17 Among a sample of 240 anesthesiologists from Australia and New Zealand, 92% reported peers as the predominant source of support after an adverse event. 9 Similarly, 92% of respondents in our survey reported a colleague (peer or senior) as their most preferred sources of support, and seeking advice from a mentor or close colleague was the most common coping mechanism used.
Nevertheless, a study of more than 3000 physicians in Canada and the United States across a spectrum of specialties (internal medicine, pediatrics, family medicine, surgery) demonstrated that 90% think that hospitals and healthcare organizations do not adequately support their recovery after an adverse event. 6 Compared to physicians in other specialties such as emergency medicine or anesthesia, surgeons are less likely to seek support in the workplace. 17 In our cohort of vascular surgeons, more than half of respondents indicated that they are aware of local support services offered by their institution or healthcare organization, however this may not directly correlate with their real-world use or adequacy in providing support. Provincial physician health programs were commonly cited among the services respondents were aware of, but only 3% indicated interest in speaking to a licensed counsellor as a preferred source of support. This concept is not unique to vascular surgeons, as it is well-documented that conventional hospital or healthcare organizational supports such as employee assistance programs are infrequently utilized and that most physicians would prefer to speak with a peer rather than with a counsellor.18,19
Support among peers is a natural phenomenon, but its success relies heavily on the availability of a mentor or close colleague, their training and skill set in facilitating effective conversation, and the individual’s comfort in asking for help. Our study found that while all but 1 (99%) of the respondents have supported or are willing to support a colleague after an adverse event, almost a third do not have a mentor or close colleague to reach out to. Those without a mentor or close colleague equivalent were less likely to prefer peers as a source of support; whether this reflects a lack of availability in having collegial support, or lack of desire to reach out to a peer supporter is unclear. Among those with a mentor or close colleague equivalent, 1 in ten reported that they would only speak with them about an adverse event if asked first by the peer in an appropriate setting. Other groups have recognized this need for organizational support in caring for the well-being of clinicians as “second victims,” creating formalized peer support programs with this specific mission in mind. 20 The first of its kind originated at the Brigham and Women’s Hospital in 2009, providing one-to-one confidential and non-judgemental support by trained volunteer peers using an outreach approach. 21 Since the development of this model, peer support programs have been adopted by centres across the United States and internationally.19,22,23
In Canada, organizations like the Canadian Medical Association have launched a Peer Support Program for all residents and staff across the nation using a different approach of group peer sessions led by trained facilitators. Additionally, a few of the resident wellness offices among Canadian institutions are in the initial stages of launching programs for their trainees utilizing the evidence-based one-to-one peer support model developed at the Brigham and Women’s Hospital. 21 Still, there is a gap in providing these much-needed support services among particular groups and there is uncertainty as to whether such programs would be readily transferable or appropriate for all medical disciplines. Our findings show that half of Canadian vascular surgeons and trainees would utilize a discipline-specific peer support program if offered through a national organization like the CSVS. Cited advantages to such a program include how some vascular surgeons in smaller centres may not have colleagues to turn to locally, as well as the fact that “vascular surgeons have a better understanding of and appreciation for vascular specific adverse events.” This concept of matching supporters from a similar specialty is 1 of the considerations used by the Brigham and Women’s Hospital model, particularly when the adverse event is unique to a discipline. 21 However, there is insufficient literature on this consideration for discipline specificity. Concerns of confidentiality, lack of rapport with distant peers, or feeling ashamed were identified among those opposed to a nationally organized program tailored to a relatively small community like vascular surgery. For individuals that expressed these concerns, support from a colleague from another discipline may help lessen the associated judgement and stigma.
While our findings may not show definite support for such an initiative through a national society, it is clear that the Canadian vascular surgery community is affected by adverse events and that there is an appetite for peer support. As evidenced in our residency programs survey, some formalized mentorship programs are in place to support learners to address adverse events when they arise. But for those without such mentors, or staff surgeons without organized supports, an intermediate approach may include educating our vascular surgery community on the detriments of adverse events and empowering surgeons with skills to engage in these sensitive conversations with colleagues when adverse events happen. In a study among American pediatric surgeons, a prominent theme was that many surgeons mean well but lack the tools and the awareness to effectively support their colleagues in the wake of a medical error or death. 24 National organizations and professional societies are in a position to provide this awareness and education through established avenues such as continuing medical education events, sparking conversation among local teams and providing them with the means to implement formal or informal supports best suited to its members and groups.
Among trainees, the support and comfort provided from a peer of similar training level may be different from that of a senior or staff colleague. In our cohort, 87% of vascular surgery trainees selected peers as a preferred source of support, whereas only half indicated senior colleagues as a preferred option. Fostering a culture for mutual support early as a the tools for resilience may be important during training, as described by 1 of our survey respondents: “We should learn to deal with adverse events in residency or have a system in place to assist trainees and those transitioning into practice.” In the Emergency Medicine literature, initiatives such as Ice Cream Rounds have gained popularity. 25 These sessions are led by residents trained in peer-support facilitation, following a semi-structured format that allows residents to share stories, emotions, and challenging experiences such as medical errors. Additionally, the notion of a “wellness curriculum” has also been proposed to combat burnout during residency training, focusing on wellness topics such as establishing mentorship programs, hands-on sessions on tactical breathing, and mental rehearsal of complex tasks. 26 Providing residents with the time and tools to help themselves and their peers will create the foundation for a cultural shift in physician wellness.
Our study is not without its share of limitations. First, it is limited by its cross-sectional design relying on retrospective recall by participants of events which may have impacted them from many years ago. Despite anonymity, the sensitive nature of our topic may preclude respondents from reporting outcomes such as maladaptive coping mechanisms (ie, use of alcohol, medications, or drugs). Our sample was broadly representative of the CSVS membership, with similar proportions of staff and trainee responses compared to the general membership, but a 28% total response rate must be interpreted with caution. Lastly, due to the inherently lower proportion of residents and fellows, our sample size was limited when making statistical comparisons between attending vascular surgeons and trainees.
Conclusion
Adverse patients events and near misses have serious negative impact on the lives of Canadian vascular surgeons and trainees. Peers and senior colleagues are the most desired source for support, but this is not universally available. Organized efforts are needed to bring awareness in our vascular surgery community on the ubiquitous nature and detrimental effects of adverse events. The health of vascular surgeons is dependent on meeting our mutual needs for peer support.
Supplemental Material
Supplemental Material - The Emotional Impact and Coping Mechanisms Following Adverse Patient Events Among Canadian Vascular Surgeons and Trainees
Supplemental Material for The Emotional Impact and Coping Mechanisms Following Adverse Patient Events Among Canadian Vascular Surgeons and Trainees by Sally HJ. Choi, MD, Tyler D. Yan, MD, Jonathan Misskey, MD, MHPE, and Jerry C. Chen, MD, MSc in Vascular and Endovascular Surgery
Footnotes
Acknowledgments
We thank Dr Jo Shapiro (Harvard Medical School) and Dr Reema Harrison (School of Public Health and Community Medicine, University of New South Wales) for their collaboration in providing the HPEEQ survey which led to our own adapted survey tool.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.