
Abstract
The management of Kommerell’s Diverticulum (KD) has been evolving from open repair to a hybrid of open and endovascular repair. While there is no consensus regarding the optimal strategy, the need for less invasive treatment with less morbidity early recovery, and improved quality of life is a common goal for both the patient and the provider.
In this case report we describe the management of our most recent case of KD where we used the robot to transect the KD and mobilize the subclavian artery to permit a carotid to subclavian artery transposition through a small incision in the neck followed by percutaneous TEVAR (Thoracic; endovascular aortic repair). The incremental benefits of this approach over the traditional approach are; discussed.
We obtained the patient’s permission to send this report for publication.
Case Report
This is a 37-year-old Caucasian female who first presented with embolic lesions to the fingers of the right hand in August 2020. Workup revealed an aberrant right subclavian artery with KD arising from the descending thoracic aorta and coursing posterior to the esophagus. (Figure 1(a) and (b)) The distal subclavian and proximal axillary artery were noted to be aneurysmal. There was no evidence of TOS (Thoracic outlet syndrome) by physical exam or exercise stress testing specifically for TOS. Endovascular and open treatment options were presented to the patient, but she was uninterested. The aneurysmal section of the artery was excluded using an 8-millimeter VBX covered stent. VBX stent was chosen for better apposition to the wall of the excluded subclavian artery to prevent further embolization of the hand. The stent however occluded within 4 to 6 weeks. The reason for the failure of the VBX stent is unclear. However, on account of extensive collaterals, perfusion to the hand remained satisfactory and the patient did not experience ischemic symptoms in the right hand or claudication symptoms involving the muscles of the right arm she was managed conservatively. (a)3D reconstruction of the arch and Aberrant Right Subclavian Artery. (b) Aberrant right subclavian artery.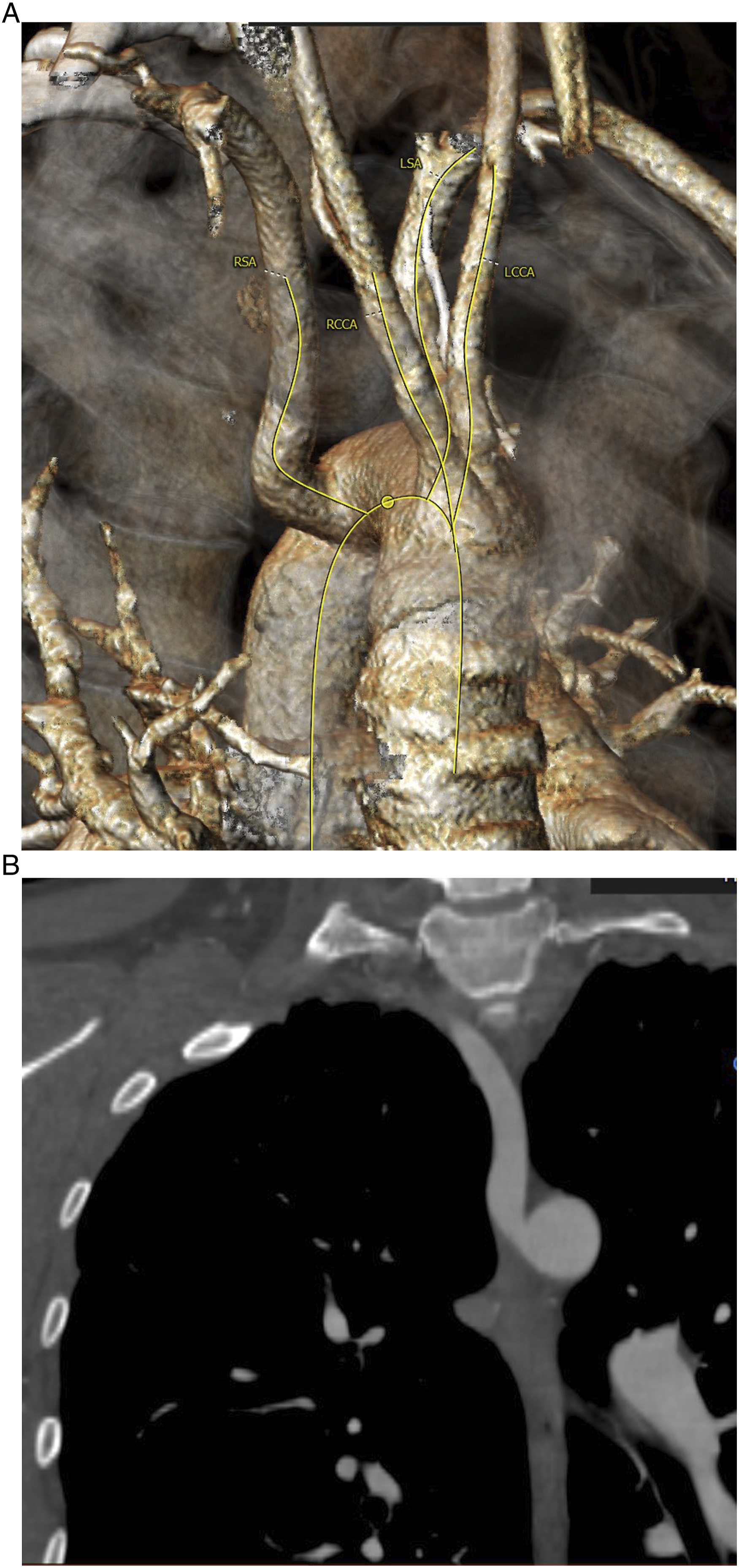
She presented a few months later with a cryptogenic stroke in the right parietal distribution of the brain with left sided weakness. Occlusion of the distal middle cerebral artery was noted on MRA (Magnetic; resonance angiography) examination. Workup revealed the presence of patent Foramen Ovalle (PFO) and atrial septal defect (ASD). She underwent closure of the PFO with good results. She recovered almost completely from the left-sided weakness. No specific genetic testing for connective tissue disorder was done. Since there was no surgical specimen, pathogenic testing of the abnormal arterial segment is not available.
She presented 2 years later complaining of numbness and tingling in the fingers of the right hand, pain in the right clavicular region, and dysphagia. Monophasic waveforms were noted in the right axillary, brachial, radial, and ulnar arteries on duplex ultrasound examination. The right wrist to brachial; index was .79 vs 1.01 on the left. CTA (Computed tomography angiography) off the chest showed a; retropharyngeal course of the proximal subclavian artery with occlusion of the right subclavian artery; between the right clavicle and the right first rib. There was a reconstitution of the distal subclavian artery via collaterals with patent axillary, brachial, and distal vessels of the arm. We presented her case to our multispecialty team and came up with a treatment plan. This plan was discussed with the patient who wished to proceed as recommended.
She underwent robotic right chest exploration with mobilization and ligation of the aberrant right subclavian artery. General anesthesia was induced with a double-lumen endotracheal tube and the patient was positioned in the left lateral decubitus position with the right side up. Three robotic arm incisions and an additional port incision for the assistant were made. The robotic portion of the procedure was done by a thoracic surgeon with robotic training. The lung was isolated, and the robot was docked. The aberrant right subclavian artery was readily apparent and using blunt dissection and electrocautery it was mobilized completely from the level of the Aortic arch all the way to the thoracic inlet. A small side branch was ligated with clips. The thoracic duct was visualized running anterior to the; aberrant vessel and was clipped. The aberrant subclavian artery was completely mobilized and divided; using an endo GIA stapler above the aortic arch. The previous retro-esophageal course of the artery was no longer the case. This left a long segment of the divided subclavian artery available for reimplantation onto the side of the common carotid artery. A 24 French chest tube was inserted, and the incisions were closed.
The patient was repositioned in the supine position and re-prepped and draped in the usual sterile fashion. A 3-centimeter incision was made above the right clavicle and the right common carotid artery was dissected out. The right subclavian artery which had been mobilized was likewise dissected out taking care not to disrupt the large collateral vessels that were supplying her right arm. The subclavian artery was tunneled behind the jugular vein and both the carotid and subclavian arteries were clamped and opened. A running end-to-side anastomosis was performed between these 2 vessels. The anastomosis was de-aired and opened. There was no change in near-infrared spectroscopy (NIRS) used for cerebral oximetry during the period of carotid clamping. The incision was closed in layers and there was no evident complication. (Figure 2) Transposed right subclavian artery to the side of right common carotid artery.
48 hours later, the patient underwent percutaneous TEVAR without left subclavian artery coverage using Cook Alpha 24 × 24 × 105-millimeter endograft deployed immediately distal to the left subclavian artery with good effect. There was an adequate proximal landing zone distal to the origin of the right subclavian artery to the aorta to reliably exclude the KD by the TEVAR graft. This has been documented in the follow-up CTA. Post-deployment angiography demonstrated brisk filling of the left subclavian artery and complete exclusion of the KD remnant. The femoral access vessels were closed using closure devices without any problems. The patient was discharged from the hospital 2 days later in good condition. CTA following the repair shows satisfactory exclusion of KD by the TEVAR with no endoleak. The Carotid to Subclavian transposition is patent with occlusion of the distal Subclavian artery as previously seen. Large collaterals reconstitute the distal Subclavian and Axillary arteries. She continues to do well 3 months following the repair and has not complained of ischemic symptoms in the right upper extremity. (Figure 3). No non-invasive vascular lab study has been done. Large collaterals that have matured over time perfuse the right hand and upper extremity; the patient remains free of ischemic symptoms on antiplatelet therapy. She remains on Aspirin mg OD antiplatelet treatment and will undergo annual CTA of the repair as per our follow up protocol. TEVAR for exclusion of kommeralls diverticulum.
Discussion
At our institution we have adopted a multidisciplinary approach to the management of KD with cardiac surgery, vascular surgery, and Interventional Radiology involved in the delivery of care for all patients with KD. Our aim is to individualize the treatment to the patient under consideration. The factors taken into consideration are the presenting symptoms, anatomy of the lesion, physiologic status of the patient, and discussion of the treatment choices with the patient. In this instance, we solicited help from a thoracic surgeon with robotic skills for resection of the KD. All possible treatment choices including carotid-axillary bypass were presented to the patient; she opted for robotic resection of KD with carotid-subclavian transposition.
We have recently published our experience with the management of KD which has been a hybrid strategy of Carotid- Axillary artery bypass, followed by endovascular occlusion of the central abnormally situated subclavian artery and TEVAR to exclude the origin of the KD with good results. 1 We have not recommended open repair for the past 5 years and have had the opportunity to correct a failed open repair done at an outside institution by endovascular means.
Patients who present with dysphagia lusoria have in the past have preferentially undergone open repair involving resection of KD to eliminate the extrinsic compression of the esophagus by the diverticulum. 2
Depressurization off the diverticulum by the placement of coils or vascular plugs in the aberrant subclavian artery carefully placed to not compress the esophagus has been successful in relieving the symptoms of dysphagia lusoria. The decreased morbidity of a Hybrid repair compared to the traditional open repair via thoracotomy, Aortic cross-clamping, cardiopulmonary bypass, or circulatory arrest is preferred by most patients. Several authors have reported comparable outcomes with similar complication rates over the intermediate term when reporting the results of open repair vs hybrid repair.3-5
In the case described above, the right common carotid artery to subclavian artery transposition was completed through a small neck incision. (Figure 4) The Carotid artery to Axillary artery bypass using an 8-millimeter externally supported PTFE graft was not required. Carotid- subclavian transposition accomplished through a small neck incision.
This case report is also unique in that resection of the aberrant subclavian artery from the aorta with subsequent transposition to the ipsilateral carotid artery eliminates the need for closure of the aberrant subclavian artery. By eliminating the presence of the retropharyngeal KD by robotic resection, esophageal compression symptoms are not longer valid. Concerns off the placement of coils or vascular plug behind or close to the esophagus causing continued compression of the esophagus and therefore symptoms of dysphagia have been eliminated. This must be a major advantage over the hybrid technique since all possible complications associated with the embolization of the aberrant subclavian artery is no longer a consideration. Figure 5 Cartoon of port placements for robotic resection of KD.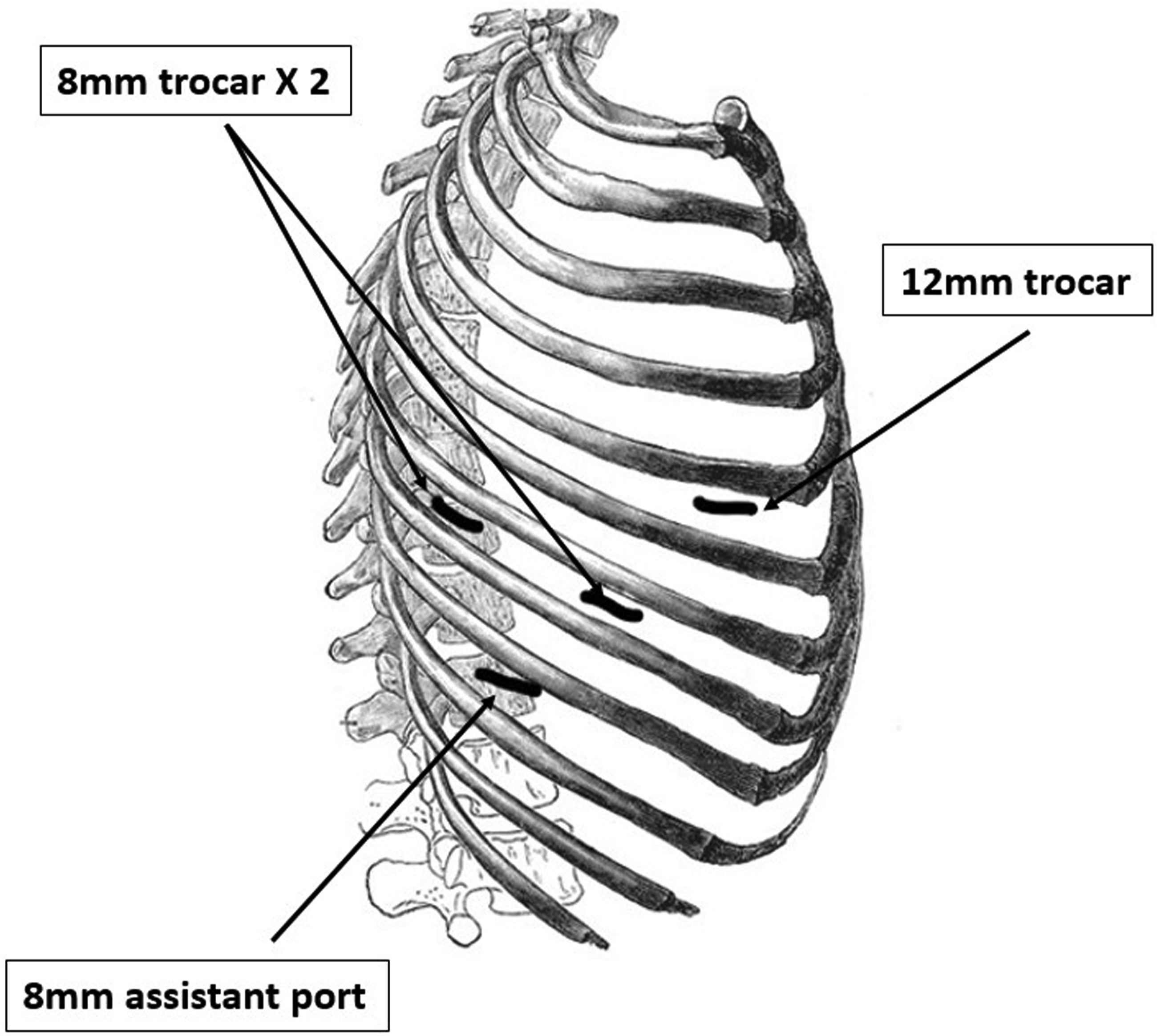
There have been reports of resection of vascular rings and KD in children using VATS (Video-assisted thoracoscopic surgery) as well as the robot.(6–9) La Regina, Prouse et al have reported a two-step treatment of Carotid- Subclavian bypass followed by robotic-assisted resection of the aberrant right subclavian artery.9,10 However, the combination of resection of the KD using the robot with Carotid- Subclavian transposition and TEVAR to exclude the origin of the KD from the Aorta, has not been reported to the best of our knowledge.
Histological analyses of resected KD have demonstrated a high prevalence of cystic medial necrosis. 5 Recognition of this finding explains the aneurysmal degeneration of any remaining remnant of the KD left behind following surgical resection. Covering the origin of the KD from the Aorta by TEVAR therefore should be an integral part of the treatment.
Finally, patient satisfaction which is an important metric with regards to any intervention was extremely high. This is especially true as the alternatives were major open thoracotomy with graft replacement of the involved section of the descending thoracic aorta or the three-step hybrid procedure.
We offer this technique for consideration to the readers of the journal as an elegant less invasive technique for the management of a patient with symptomatic Kommerell’s Diverticulum.
Footnotes
Acknowledgment
Jaimie Keith NP and Melissa Lirag PA helped out with management of this patient and obtained consent from the patient for publication of this report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.