
Abstract
The effect of changes in bladder volume on the caliber of adjacent veins is underappreciated but essential to recognize to avoid complications such as unnecessary stenting or clot migration causing pulmonary embolism. Here the authors illustrate the importance of this finding in 3 cases using venographic and endovascular sonographic imaging: the first in which BPH-induced chronic bladder outlet obstruction resulted in DVT formation, the second in which the cause was unrecognized and unnecessary stenting performed, and the third in which inappropriate treatment was avoided by decompressing the bladder.
Keywords
Introduction
As mechanical DVT thrombectomy is performed with increasing frequency, distinguishing between normal and pathological findings will be paramount to ensure appropriateness of treatment. One potential pitfall is extrinsic compression of the deep veins of the pelvis caused by distention of the urinary bladder. Failure to recognize this phenomenon can result in unnecessary stenting or migration of clot with possible catastrophic pulmonary embolism. Here the authors illustrate the importance of this finding in 3 cases: the first in which BPH-induced chronic bladder outlet obstruction resulted in DVT formation, the second in which the cause was unrecognized and unnecessary stenting performed, and the third in which inappropriate treatment was avoided by decompressing the bladder.
Cases
IRB approval was granted for this retrospective case series by the Yale Human Research Protection Program Institution Review Board, Human Investigation Committee 2A, Protocol ID 2000032179. Given the retrospective nature of the study, obtaining informed consent was not required.
Case 1
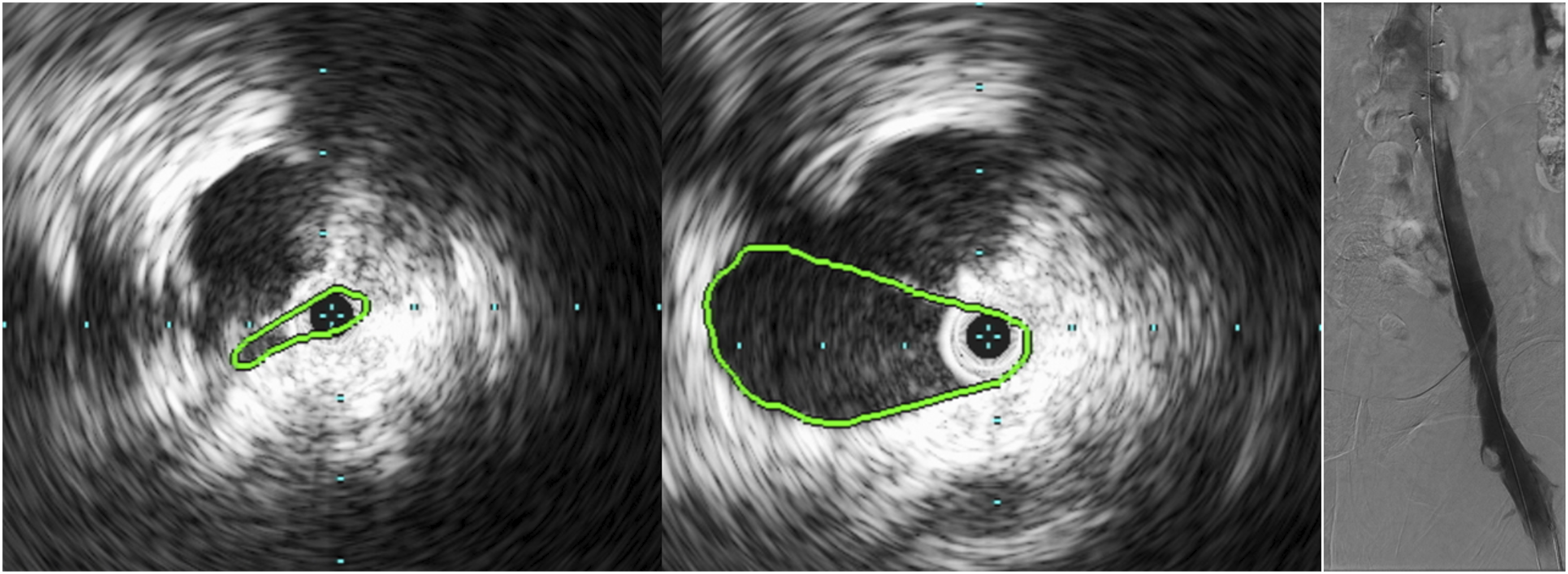
A 67-year-old man presented with several days of right leg swelling and was found to have right lower extremity DVT; he also noted 3 months of swelling of the left leg which had recently resolved. CT venogram demonstrated marked distention of the urinary bladder due to prostatic enlargement resulting in compression of the bilateral external iliac veins with thrombus extending to the level of the compression on the right (Figure 1). He had no prior episodes of venous thromboembolism, had no history of malignancy, denied recent prolonged immobility, and had never taken blood thinners. Given failure to improve after 3 days of therapeutic anticoagulation, mechanical thrombectomy was performed. A Foley catheter was placed but clamped to avoid inducing embolization from resolution of venous compression. The patient was then positioned prone and Intravascular ultrasound (IVUS) performed, demonstrating marked narrowing of the right iliac vein (Figure 2). After removal of most of the thrombus, the catheter was unclamped, and the bladder decompressed. After over 1 L of urine had drained, venography and IVUS confirmed resolution of narrowing and therefore stenting was not performed. The bladder catheter was left in place after the procedure, and the patient experienced symptomatic resolution. He was discharged on post-procedure day 2 and the foley catheter removed 1 week later. As of 14 months later, he continues to take apixaban and tamsulosin without recurrence. [Case 1] (Left) Sagittal reconstruction contrast-enhanced CT demonstrating marked bladder enlargement due to benign prostatic hyperplasia (arrow). (Right) Coronal oblique contrast-enhanced CT demonstrating compression of bilateral external iliac veins due to bladder distention; thrombus extends peripherally from the level of the right-sided compression (arrow). [Case 1] IVUS images of the right external iliac vein obtained before (left) and after (middle), allowing the bladder to decompress, demonstrating marked enlargement of the vessel lumen (green outline) following bladder evacuation. (Right) Fluoroscopic image showing final appearance of the deep veins.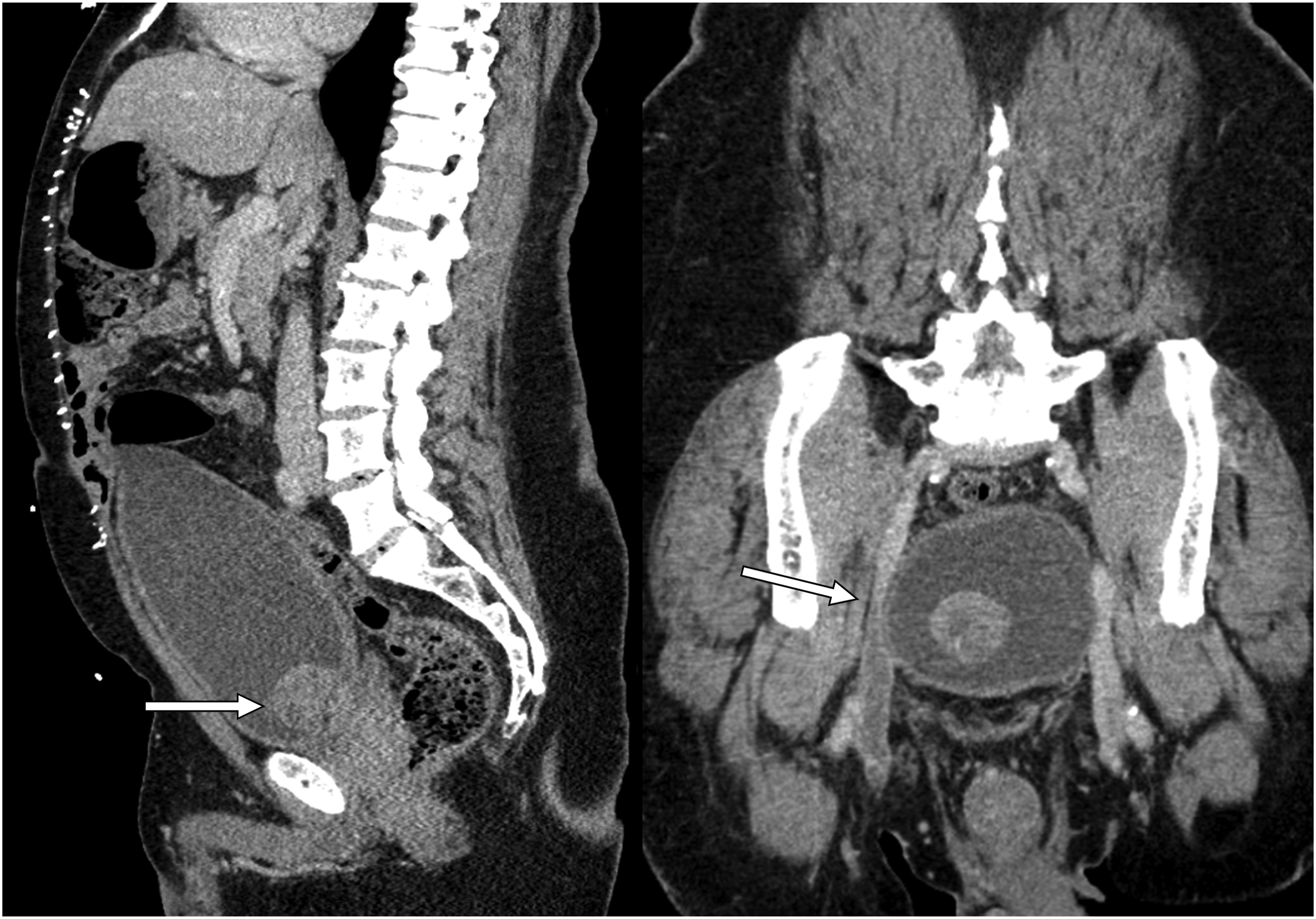
Case 2
A 56-year-old male presented 1 month after right hip arthroplasty with calf pain and was found to have right lower extremity DVT extending centrally to the level of the external iliac vein. Mechanical thrombectomy was performed following which the pelvic veins appeared widely patent. The patient was started on anticoagulation but, despite adherence, he developed recurrent thrombosis 1 month later necessitating repeat thrombectomy. During this procedure there was new narrowing of the external lilac vein which recoiled after angioplasty (Figure 3). Given concern for external compression, a cone beam CT was performed (Figure 4). Although no mass was identified, given persistent narrowing a stent was placed with improvement in vascular caliber. Retrospective review of the cone-beam CT demonstrated a distended bladder displacing pelvic soft tissues which in turn compressed the vein. [Case 2] Right iliac venography demonstrating wide patency of the external iliac vein during the first procedure (left) and new narrowing of the vein after angioplasty during the second procedure 1 month later (right). [Case 2] Cone beam CT obtained during the second procedure demonstrating narrowing of the right external iliac vein (arrow) by the distended bladder.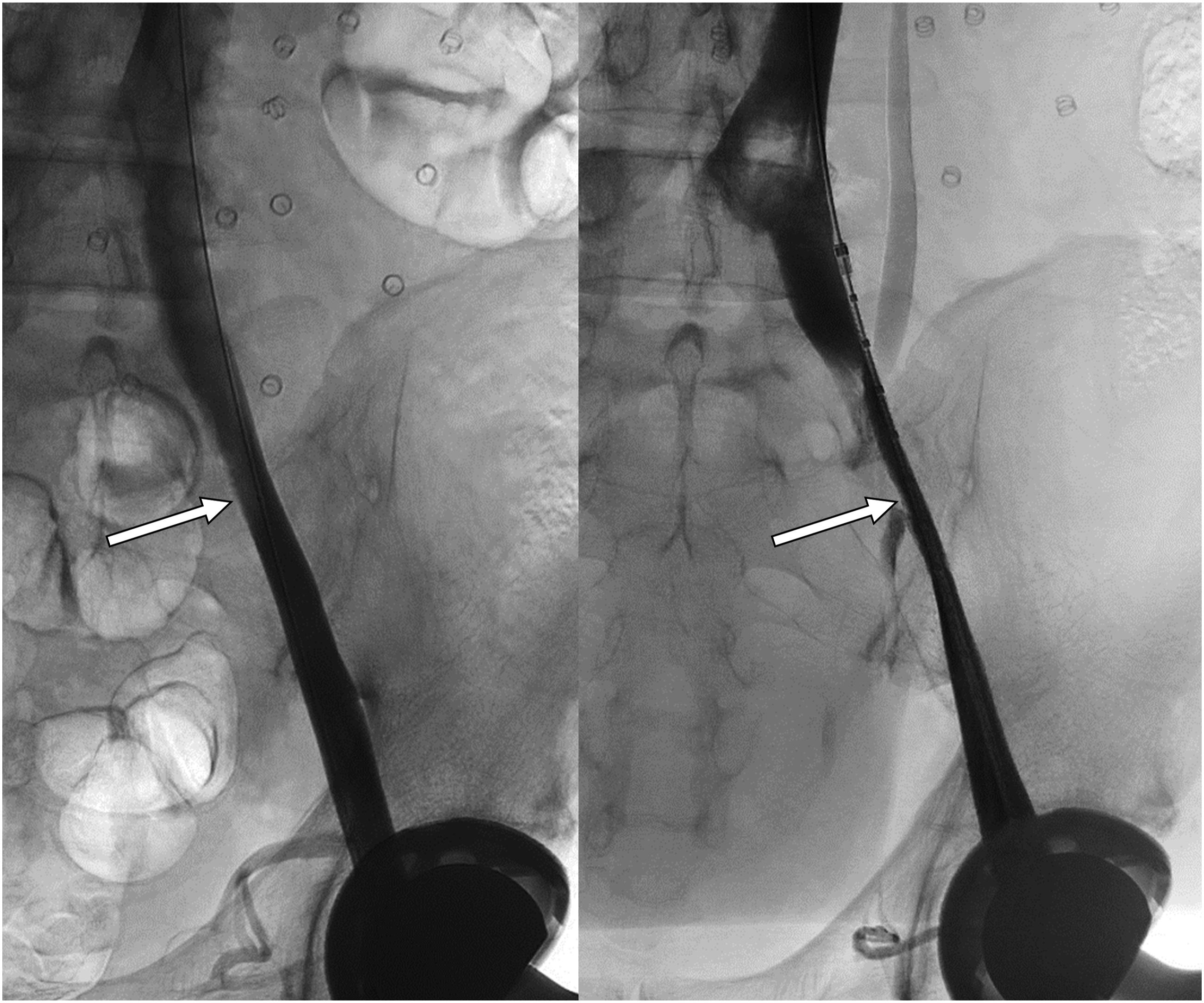

Case 3
A 34-year-old male with traumatic brain injury and recurrent venous thromboembolism post placement of an Optease filter (Cordis, Hialeah, FL, USA) 16 years prior presented with bilateral lower extremity swelling and pain. Imaging revealed thrombosis of the filter extending into both lower extremities so, after failure to improve after 3 days of therapeutic anticoagulation, mechanical thrombectomy was performed. As the filter was extensively fractured it was left in place; however, the bilateral lower extremity veins were widely patent. The patient was noncompliant with anticoagulation and 5 months later presented with recurrent thrombus extending through the filter. Repeat thrombectomy was performed, after which a stent was placed across the filter and a new suprarenal filter deployed. During the procedure, progressive narrowing of the left external iliac vein was noted. As this was thought to be due to bladder distention, a Foley catheter was placed, and the bladder decompressed. Intravascular ultrasound images obtained during decompression revealed progressive increase in vascular caliber as urine drained (Figure 5). The thrombectomy was then completed without iliac vein stent placement. [Case 3] IVUS images of the left external iliac vein demonstrating progressive increase in vessel lumen from the initial (left) to after drainage of 350 mL urine (middle) to after drainage of 500 mL urine (right).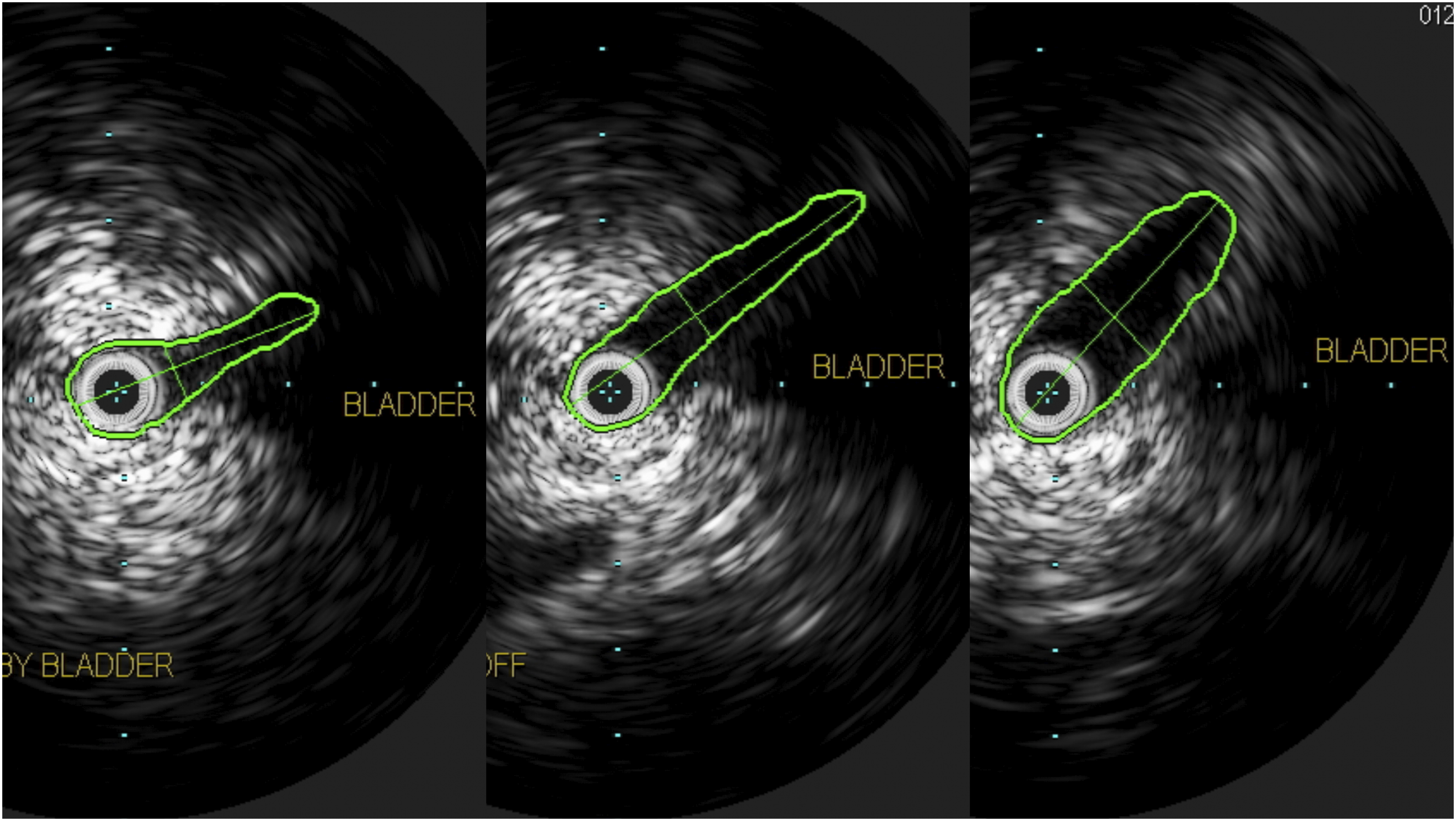
Discussion
It has long been recognized that a chronically distended urinary bladder can compress the adjacent iliac veins, increasing venous pressure and causing lower extremity edema.1,2 Similarly, though rare, deep venous thrombosis resulting exclusively from bladder-induced venous compression has been reported.3,4 By contrast, progressive venous narrowing caused by increasing bladder distention over the course of a single case has not to the authors’ knowledge been described but has significant implications for treatment. Here the authors provide venographic and IVUS imaging confirming this phenomenon and illustrate the consequences of failure of recognition.
The first case illustrates the feasibility of chronic bladder distention in causing compression and thrombosis adjacent veins. Although thrombus was present only on the right, the history of left-sided swelling suggests that resistance to flow was present bilaterally. The second case demonstrates a similar phenomenon but occurring acutely, as well as the consequences of failure of recognition with unnecessary stent placement. Retrospective assessment of the CT scan confirmed both bladder distention and veinous narrowing; importantly, however, the bladder did not directly compress the vein but rather displaced adjacent soft tissues which themselves impinged upon the vessel. The third case exemplifies the appropriate approach when this phenomenon is suspected, with imaging confirming a cause-and-effect dose response relationship between bladder volume and venous caliber.
In venous interventions that may be prolonged, preemptive placement of a Foley catheter should be considered for patient comfort and accurate assessment of venous caliber. If increasing extrinsic-appearing venous stenosis is observed during a case, consideration should be given to bladder distention as the cause. In those cases where thrombus is present, bladder decompression prior to thrombectomy should be avoided given the possibility of inducing embolization.
Conclusion
Recognition of bladder distention as a cause of acute iliac vein narrowing is essential given the alterations in management it necessitates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.