
Abstract
This report demonstrates the successful treatment of a carotid artery pseudoaneurysm using percutaneous thrombin injection. The patient, a 62-year-old woman with multiple comorbidities, experienced a pseudoaneurysm following an unintentional carotid artery puncture during a failed attempt to place a triple lumen catheter in the right jugular vein. Percutaneous thrombin injection was chosen as the treatment method, with Doppler ultrasound monitoring. Follow-up examinations showed no signs of recurrence, and the patient was discharged after nine days without complications.
Keywords
Introduction
Internal jugular triple lumen catheters implantation has been associated with the recognized but uncommon complication of carotid artery arterial puncture. 1 The development of a pseudoaneurysm following such an unintentional carotid artery puncture is extremely uncommon, there is a dearth of literature and few case reports. 2 Both surgical and endovascular treatments can be used in the case of traumatic carotid artery injuries, surgical intervention is the primary choice in the treatment of pseudoaneurysms, however, endovascular percutaneous techniques are increasingly gaining recognition as valid alternatives, specifically using stents.3,4 In recent years, for iatrogenic pseudoaneurysms of the femoral artery, percutaneous ultrasound-guided thrombin injectionhas become the first-choice treatment, considering the absence of guidelines.; this procedure has a high technical success rate, few complications, and low recurrence rates. 5
We describe how the carotid artery pseudoaneurysm was successfully treated using percutaneous thrombin injection.
Case Presentation
A 62-year-old woman was under hemodialysis treatment due to severe chronic kidney disease (stage V) caused by diabetic nephropathy; the vascular access was an arteriovenous fistula (AVF) in the right upper arm, with superficialization of the basilic vein. A native AVF in the radio-cephalic region had already occluded in 2021 despite previous endovascular treatments. She had a history of type II diabetes, chronic ischemic heart disease and bronchitis. The patient presented to the hemodialysis unit for her regular dialysis session but experienced a dysfunction of the vascular access with circuit loss. The following day, a complete occlusion of the fistula was confirmed; an emergency attempt to perform mechanical thrombectomy of the fistula failed, and the patient was subsequently admitted for appropriate care.
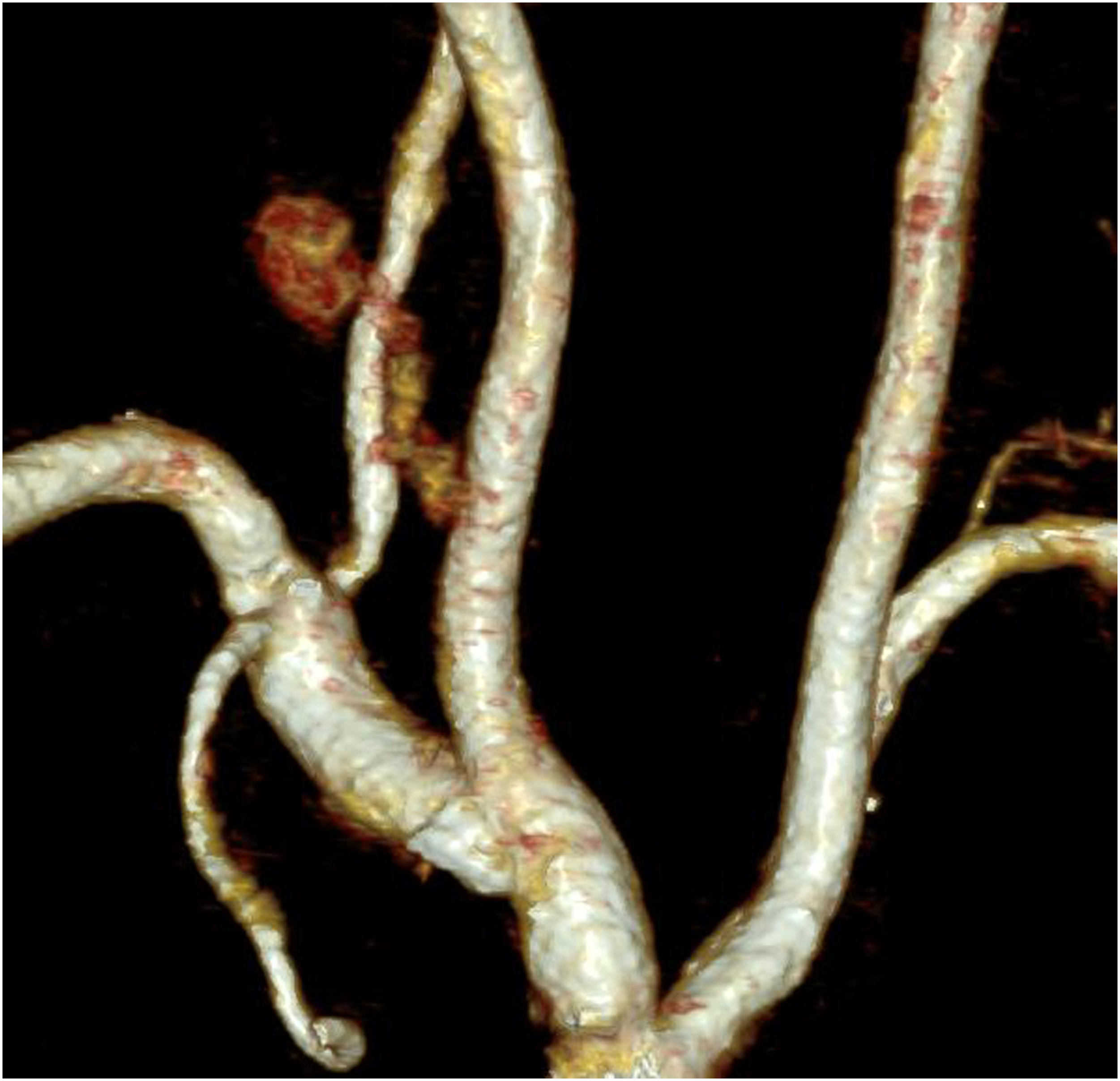
During the patient's hospital stay, an attempt was made to place a triple lumen catheter (CVC) in the right jugular vein, unsuccessful due to bleeding from the puncture site. After applying prolonged manual pressure to the puncture site, which stopped the bleeding, a CVC was subsequently inserted in the right femoral region. Following this, a color Doppler ultrasound of the neck vessels revealed the presence of a pseudoaneurysm connected to the proximal right common carotid artery. The patient lost almost 2 points in hemoglobin over 48 hours (from 8.9 g/dL to 7 g/dL), so 2 units of frozen red blood cells and 2 bags of fresh plasma were administered. In addition, an increase in the size of the aneurysm during was noted at the 48 hours ultrasound check. After a cardiological evaluation, it was decided to temporarily suspend dual antiplatelet therapy in favor of a single medication. On the same day, a CT angiogram of the supra-aortic trunks confirmed the presence of a pseudoaneurysm of the right common carotid artery and a hematoma within the muscular belly of the right sternocleidomastoid muscle, where contrast medium extravasation was visible (Figures 1 and 2). The distance between vessel wall lesion and carotid bifurcation was 54 mm. Maximum diameters of the pseudoaneursym were 10 × 12 mm; the neck had a maximum caliber of 3 mm. Since the pseudoaneurysm appeared to have limited blood supply, in accordance with vascular surgeons, the case was managed by the interventional radiology unit. Due to the low-flow bleeding and small pseudoaneurysm neck, identified during the pre-procedural ultrasound examination, direct percutaneous thrombin injection was selected as the best treatment option. With the help of a 20 G needle and a regular Luer Lock Tip Syringe half filled with saline, the center of the pseudoaneurysm sac was reached. Two-dimensional ultrasound projection was used to validate the needle's proper location (Figure 3); the filling of the syringe with arterial blood confirmed the position. Doppler ultrasound monitoring was used to track the drug injection: thrombin component of the Floseal kit (Baxter, Deerfield, Illinois) diluted in the provided ampoule of 10 mL saline was slowly administered; after injection of 4 mL healing of the pseudoaneurysm was achieved. The gelatin matrix included in the kit was not used. This operation did not involve the use of a distal protective device. Axial CT angiogram of the neck showing contrast extravasation (arrow) from the right common carotid artery. 3D volume rendering CT image of the pseudoaneurysm of the right common carotid artery. Color Doppler ultrasound showing flow into the pseudoaneurysm sac before the procedure.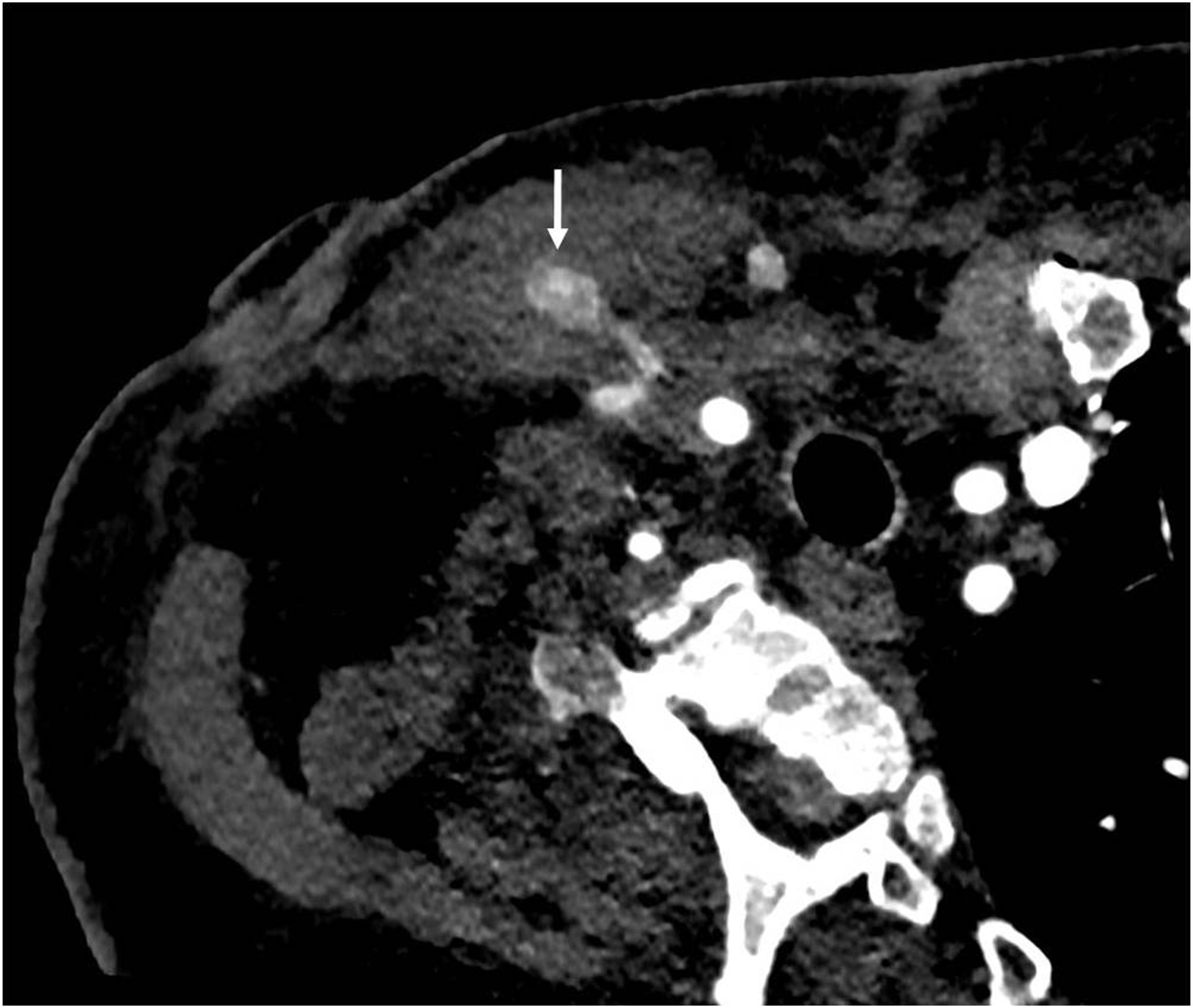

The patient underwent several ultrasounds and a CT angiography in the days following the procedure, and there were no signs of recurrence. She was discharged after 9 days without any further complications. A CT angiography repeated 1 month after the procedure confirmed the successful treatment (Figure 4). Axial CT scan of the neck 1 month after the procedure showing no sign of recurrence of the pseudoaneurysm.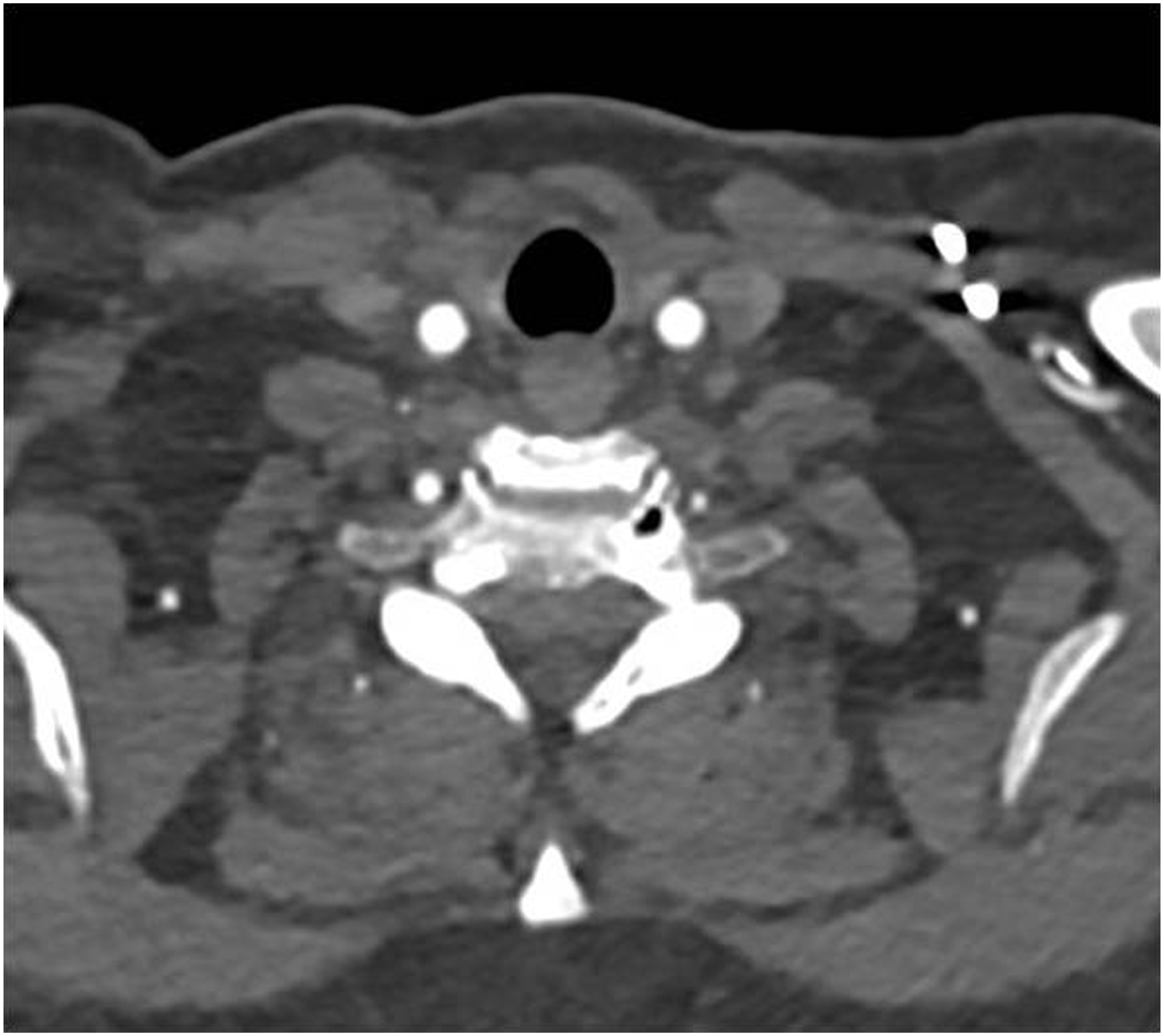
Discussion
The formation of a pseudoaneurysm of the common carotid artery following the placement of a central venous catheter (CVC) is indeed a very rare event, as described in the medical literature. 1 The rarity of this complication can make management a limited topic of discussion in the Literature, where 3 main options are typically considered: surgical treatment, endovascular management and percutaneous treatment. Traditional surgical treatment is generally considered the gold standard; it includes graft interposition or primary suturing of the carotid artery wall. 2 Endovascular treatment, on the other hand, involves the use of a metal stent to repair the leakage and keep the damaged artery open. This procedure is preferred for less severe injuries or for patients who are not eligible for traditional surgery.3,4 The decision on which procedure to use will depend on many factors, including the extent of the injury, the location of the affected artery, the overall condition of the patient, and comorbidity. Percutaneous thrombin injection is currently among the preferred methods for treating femoral artery pseudoaneurysms due to its lower complication rate. Several studies have demonstrated its high effectiveness, good patient tolerance, and low recurrence rates. 6 Complications are infrequent, ranging from 0% to 4%, and are mainly associated with thrombin leakage into the local circulation, leading to embolization of distal structures. The use of endovascular protection devices placed downstream of the aneurysm can help prevent this complication. 5 The use of percutaneous US guided thrombin injection has primarily been focused on treating common femoral artery, and its application for other types of iatrogenic pseudoaneurysms has limited reported cases. These reports include treatment for pseudoaneurysms in various locations, such as the pancreatic head, superficial temporal artery, subclavian artery, with a several focusing on brachial artery pseudoaneurysms. 7 Sheiman et al 8 and Clark et al 9 successfully treated patients with brachial pseudoaneurysms by injecting thrombin into the periphery of the pseudoaneurysm. They propose that when a well-defined neck of a brachial artery pseudoaneurysm is visible on sonography and can be externally compressed, performing this compression during thrombin injection may reduce the risk of thrombin entering the native artery. These techniques may be beneficial when performing percutaneous thrombin injection for pseudoaneurysms originating from smaller peripheral arteries.
In the medical Literature, there have been fewer than ten reported10-14 cases of using percutaneous thrombin injection to treat pseudoaneurysms of the common carotid artery. Some of these techniques, such as the 1 described by Holder et al, 10 involve using a balloon positioned proximally or distally to the aneurysm as a protective device to manage potential thrombin leaks. In contrast, others, like the method by Moller et al, 12 do not require the use of a balloon. Both procedures have shown excellent outcomes without complications.
In our specific case, the patient’s underlying medical conditions, the anatomical characteristics of the pseudoaneurysm (neck diameter less than 5 mm), and its size led us to select percutaneous thrombin injection without either proximal or distal protection as the treatment method. While some of the previously mentioned cases imply the potential use of a protective balloon, there is a scarcity of clinical studies examining the role of distal protection during thrombin injection to mitigate the risk of stroke during the procedure. Furthermore, its effectiveness in preventing thrombin micro-aggregates remains unclear. Considering the absence of reported complications without the use of a protective device and the patient's comorbidities, the current patient received thrombin treatment without balloon protection.
Given the limited number of cases reported in the literature, the use of thrombin injection within pseudoaneurysms in arteries other than the femoral artery remains a subject of controversy. Specifically, the current challenge is to determine whether the use of protective balloons or manual compression (depending on the anatomical site) are necessary measures to prevent ischemic complications.
Conclusion
This case highlights the successful use of percutaneous ultrasound-guided thrombin injection to treat a carotid artery pseudoaneurysm, emphasizing its effectiveness in locations other than the femoral artery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.