
Abstract
Purpose
Superior vena cava (SVC) syndrome is a constellation of symptoms that results from partial or complete SVC obstruction. Endovascular SVC stenting is an effective treatment for SVC syndrome with rapid clinical efficacy and low risk of complications. In this study, we assess the technical and clinical outcomes of a cohort of patients with SVC syndrome treated with the AbreTM self-expanding venous stent (Medtronic, Inc, Minneapolis, MN, USA).
Methods
An institutional database was used to retrospectively identify patients with SVC syndrome treated with AbreTM venous self-expanding stent placement between 2021-2023. Patient demographic data, technical outcomes, treatment effectiveness, and adverse events were obtained from the electronic medical record. Nineteen patients (mean age 58.6) were included in the study. Thirteen interventions were performed for malignant compression of the SVC, 5 for central venous catheter-related SVC stenosis, and 1 for HD fistula-related SVC stenosis refractory to angioplasty.
Results
Primary patency was achieved in 93% of patients (17/19). Two patients (7%) required re-intervention with thrombolysis and angioplasty within 30 days post-stenting. Mean duration of clinical and imaging follow-up were 228.7 ± 52.7 and 258.7 ± 62.1 days, respectively. All patients with clinical follow-up experienced significant improvement in clinical symptoms post-intervention. No stent related complications were identified post-intervention.
Conclusions
Treatment of SVC syndrome with the AbreTM self-expanding venous stent has high rates of technical and clinical success. No complications related to stent placement were identified in this study.
Background
Superior vena cava (SVC) syndrome is a condition characterized by partial or complete occlusion of the superior vena cava, with approximately 15,000 new cases occurring annually in the U.S. 1 Most frequently seen in patients with thoracic malignancy, SVC syndrome is typically caused by SVC obstruction from extrinsic compression by the tumor or enlarged lymph nodes, or direct vascular invasion by cancer cells.2,3 In recent years, non-malignant causes of SVC syndrome have become more prevalent due to the increasing use of intravascular devices such as central venous catheters, hemodialysis catheters, pacemakers, and defibrillators which may cause device-related thrombosis or stenosis.4,5
The clinical presentation of SVC syndrome is highly variable and depends on a number of factors including the degree of vessel obstruction, chronicity of the occlusion, and the presence of collateral flow. 3 Symptoms can include facial, neck, trunk, or upper extremity swelling, with possible signs of cerebral edema including headache, dizziness, blurred vision, confusion, or altered mental status and, in some cases, shortness of breath, hoarseness, and airway compromise. 6
Endovascular stenting is highly effective for treatment of SVC syndrome. 7 Observational studies of endovascular stenting for SVC syndrome have demonstrated a high degree of technical success with a low incidence of complication or restenosis. 3 While there are currently no standardized guidelines for stent selection, factors such as occlusion length, vessel geometry, and etiology of the stenosis play a role in this decision. 7 Uncovered stents such as the Wallstent (Boston Scientific) 1 and Gianturco Z stent (Cook Medical)(8) have commonly been used for the endovascular treatment of SVC syndrome. The Medtronic AbreTM self-expanding venous stent was approved for use by the US Food and Drug Administration in 2020 for use in treating iliofemoral venous outflow obstruction, but has also found utility in treating central venous stenosis.9-11 However, limited case reviews have been presented demonstrating the technical success and clinical outcomes of the AbreTM in the setting of SVC syndrome.
In this study, we retrospectively reviewed the technical and clinical outcomes of 19 patients who presented with clinically significant SVC syndrome and were treated using the AbreTM self-expanding venous stent at 2 academic medical centers in our health care system.
Methods
Patient Selection
The institutional review board approved this Health Insurance Portability and Accountability Act-compliant retrospective study with waiver of informed consent for participation in the study (Protocol #2023P002727). An institutional database was used to retrospectively identify consecutive adult patients with SVC syndrome that underwent endovascular stenting with an AbreTM self-expanding venous stent (Medtronic, Inc, Minneapolis, MN, USA) between 2021-2023. All interventions were performed under the supervision of attending interventional radiologists at 2 academic medical centers between 2021-2023. Patient demographic and clinical data were obtained from the electronic medical record.
Stenting Technique
SVC stenting procedures were performed under fluoroscopic guidance. Contrast venography was performed to define the severity and length of the stenosis and/or occlusion to be treated. The SVC was then crossed with catheters and guidewires via internal jugular, femoral, and/or upper extremity venous access. Limited angioplasty of the SVC was sometimes performed prior to stent placement. AbreTM venous stents were deployed either as a single stent in the superior vena cava with possible extension into the right brachiocephalic vein or in “kissing” fashion extending from the bilateral brachiocephalic veins into the SVC. Selection of stent diameter and length were at the discretion of the attending interventional radiologist. Post stent placement venography was performed to confirm stent patency and resolution of previously seen stenosis/occlusion and associated collateral veins.
Assessment of Technical Success and clinical Outcomes
Technical success was defined as successful deployment of the AbreTM stent across the SVC stenosis or occlusion with robust in-line flow of contrast material and resolution of previously seen venous collaterals. Fluoroscopic procedural images were retrospectively reviewed and interpreted by an attending interventional radiologist (blinded for peer review) to assess technical success of each procedure included in this study. Primary stent patency was defined as stent patency on follow-up cross-sectional CT imaging, if obtained, in the absence of additional interventions.
Clinical outcomes post-stent placement were assessed based on review of the electronic medical record. Symptoms of SVC syndrome, including facial/upper extremity edema, altered mental status, dyspnea, vision changes, and nausea/vomiting, were identified based on clinical documentation prior to the procedure. Clinical success was defined as resolution of previously described symptoms of SVC syndrome. Additional data including post-procedural complications and mortality were also obtained from the electronic medical record.
Statistical Analysis
Statistical analyses were performed with GraphPad Prism 9 software package (GraphPad Software, Inc, La Jolla, CA).
Results
Patient Demographics and Clinical Characteristics.
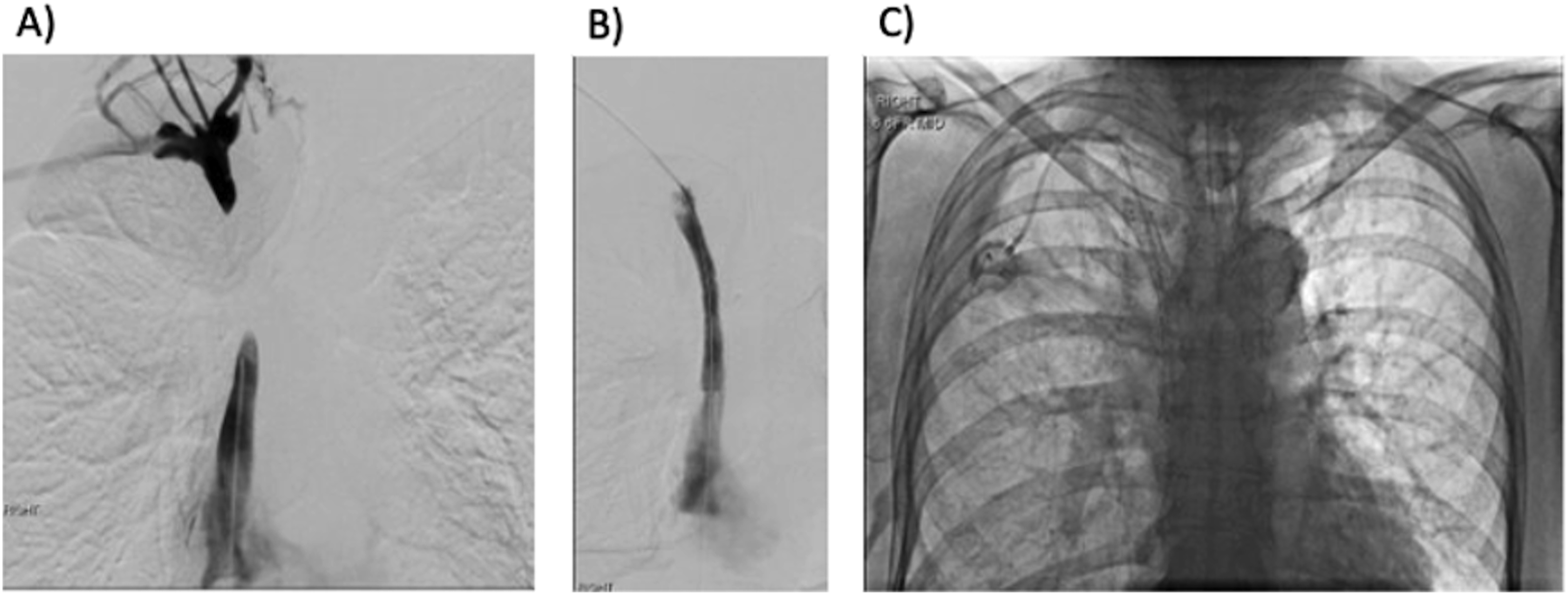
Placement of a single AbreTM venous stent was performed in 12/19 (63%) patients (Figure 1), while 7/19 (37%) underwent placement of 2 “kissing” or overlapping AbreTM venous stents (Figure 2). Stent diameters ranged from 12 to 20 mm and stent lengths ranged from 60 to 120 mm (Table 2). The majority of SVC stenting procedures were performed under general anesthesia (63%). 52 year old female patient with a history of non-Hodgkin’s lymphoma who presented with symptoms of SVC syndrome. (A) Preliminary venogram via right internal jugular access demonstrates complete occlusion of the right brachiocephalic vein at the confluence of the internal jugular and subclavian veins with opacification of numerous collateral veins. (B) Preliminary venogram via left internal jugular vein access with complete occlusion of the left brachiocephalic vein and collateral flow via the hemiazygos vein. (C) Post-stenting venogram with contrast flowing via “kissing” brachiocephalic vein/SVC stents with resolution of previously seen collateral veins. 73 year old male with a history of lung cancer and SVC syndrome secondary to bulky mediastinal lymphadenopathy. (A) Preliminary contrast injection via right internal jugular and right common femoral vein accesses demonstrates occlusion of the SVC. (B) Post-recanalization and stenting venogram demonstrates free flow of contrast through the SVC stent into the right atrium. (C) Chest X-ray demonstrating a port catheter placed through the SVC stent at the end of the procedure for chemotherapy access. Procedural Factors and Stent Properties.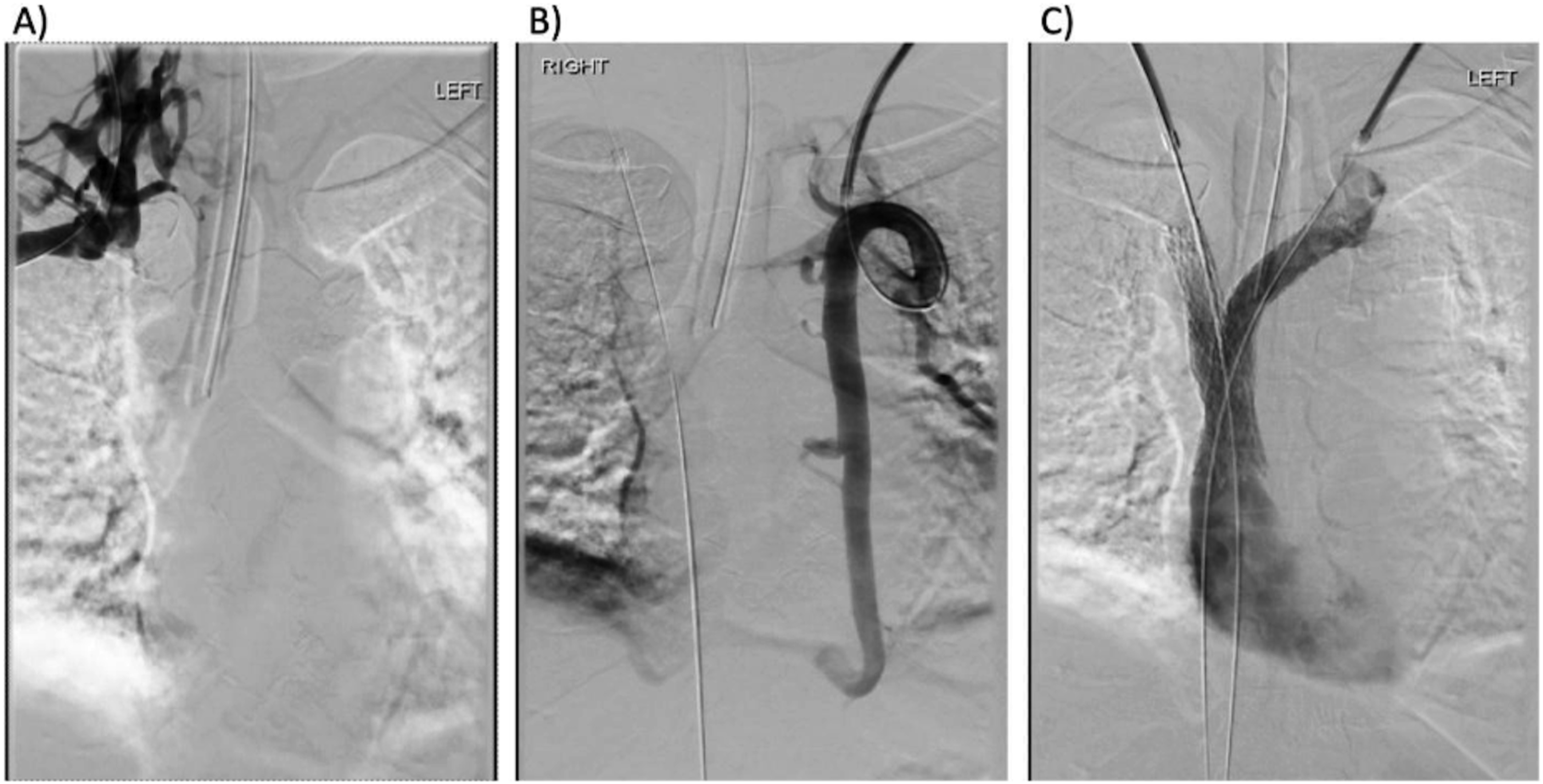
Outcomes and Patient Follow-Up.
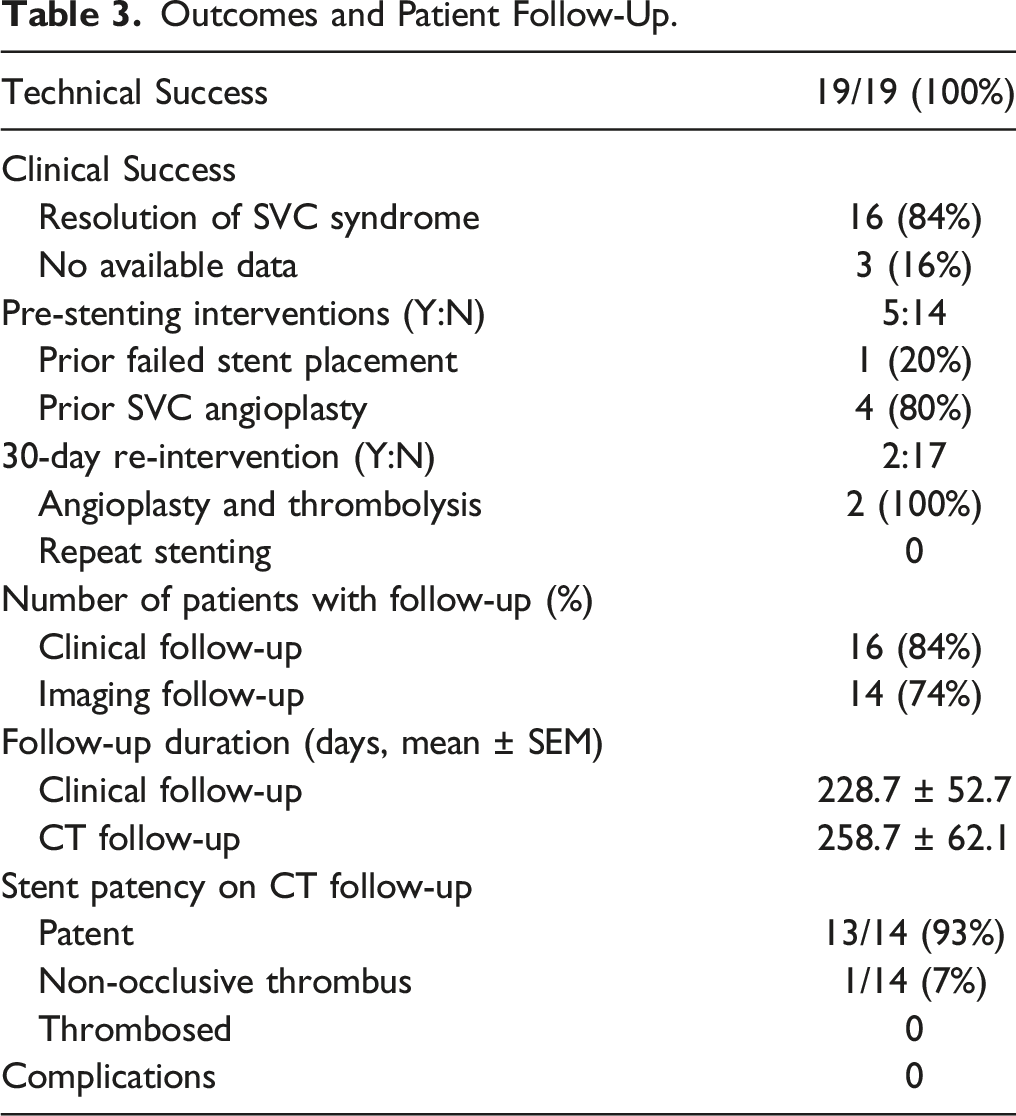
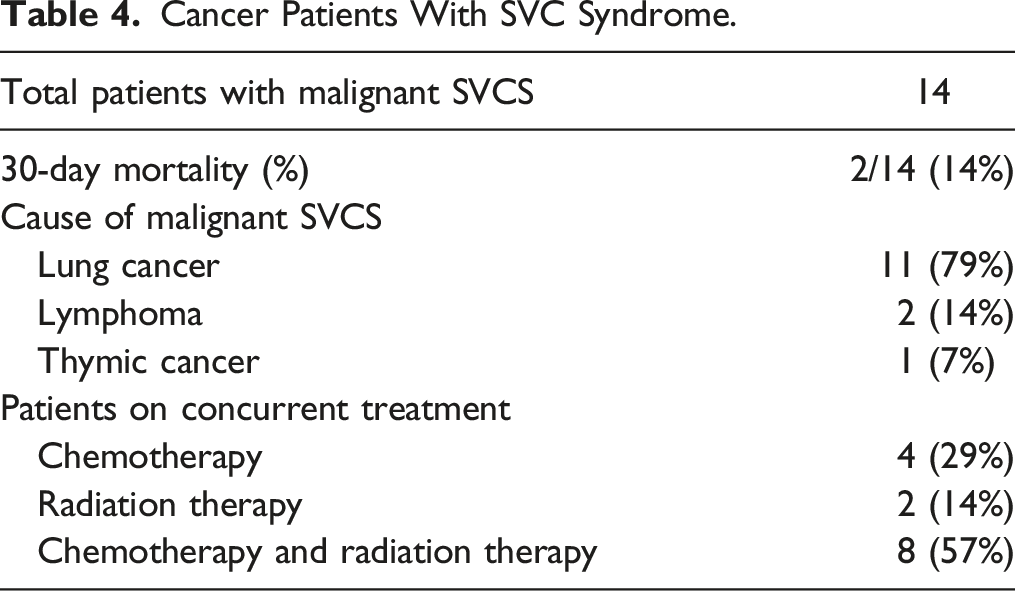
Overall, 30 day mortality post-procedure was 10.5% (2/19), with both cases occurring in oncology patients with acute presentations of SVC syndrome with associated airway compromise. Survival curves for all patients and oncology patients post-procedure are presented in Figure 3. There were no immediate complications identified post-stenting. Survival curves for all patients (overall) and cancer patients treated with the AbreTM venous self-expanding stent for SVC syndrome.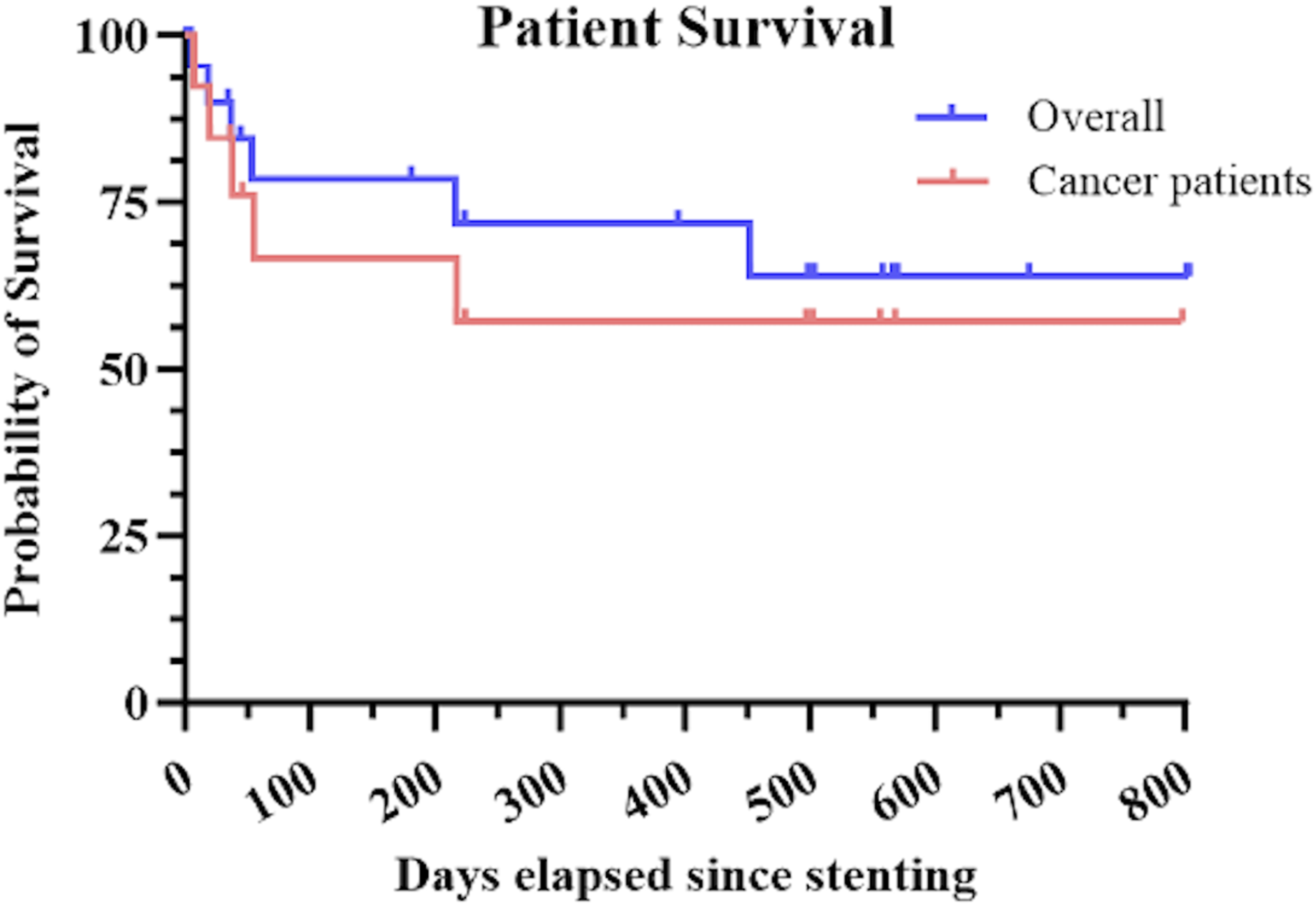
Cancer Patients With SVC Syndrome.
Discussion
The results of this study demonstrate that the AbreTM self-expanding venous stent is safe and effective for treatment of SVC syndrome. Although the use of the AbreTM stent has predominantly been described in the setting of iliofemoral venous outflow obstruction, 12 a small number of recent case studies have also described its use in treating central venous occlusion.9-11 Here, we present an analysis of the AbreTM stent in treating SVC syndrome, with an emphasis on technical success, clinical outcomes, and procedural complications.
In this study, there was a 100% technical success rate for deployment of the AbreTM self-expanding stent to treat SVC syndrome. This finding is consistent with prior literature which demonstrates high technical success for endovascular stenting for SVC syndrome across a variety of stent types.7,9-11,13 For example, a meta-analysis published in 2022 by Aung et al 14 identified 54 studies where SVC syndrome was treated with endovascular stenting and reported a pooled technical success rate of 96.8%. Note that the approach to stenting may differ in the setting of malignant and non-malignant causes of SVC syndrome, as bilateral brachiocephalic vein stents are typically not necessary in patients with malignant SVC syndrome and limited life expectancy. Unilateral re-establishment of venous blood return is typically sufficient to relieve acute clinical manifestations of SVC syndrome in these patients.
There was also clinical improvement and resolution of symptoms of SVC syndrome in 100% of patients in this study that had clinical follow-up available in the medical record. These results are consistent with high degrees of clinical effectiveness observed in numerous other studies utilizing endovascular stenting to address SVC syndrome.7,15 Both dedicated venous stents and conventional peripheral stents have demonstrated efficacy in the setting of SVC syndrome. A study by Matthaiou et al demonstrated no significant difference in primary patency rates for venous and non-venous-dedicated stents in the setting of malignant SVC syndrome in 156 patients. 16 However, there is currently limited clinical outcome data supporting the specific use of the AbreTM stent for SVC syndrome. Few studies have reported clinical improvement in the management of central venous occlusion in hemodialysis patients using the AbreTM stent, 9 while studies reporting use of the AbreTM for SVC syndrome have limited clinical follow-up.10,13,17
We further analyzed the overall post-procedure survival of this group of patients. Notably, 74% of our patient cohort had SVC syndrome secondary to malignancy, which is widely recognized as the most common cause of SVC syndrome. 2 The majority of these patients had not previously undergone SVC stenting, except for 1 patient who underwent AbreTM stent placement due to occlusion of a previously placed Wallstent in the SVC. While the overall survival of the 19 patients in this study was greatly influenced by the lower survival rate among oncology patients, the 5 patients with non-malignant SVC syndrome (catheter- or dialysis-related) achieved a 100% survival rate at 15 months post-procedure, with just 1 of these patients passing away at that time due to causes unrelated to stenting.
The AbreTM stenting procedures reported in this study had no immediate complications. While SVC stenting can potentially lead to severe complications, such as stent migration or SVC rupture, such events are rare, with studies reporting an average rate of significant complications at 2% and stent-related deaths at 1%–2%.15,18 When more minor complications, such as pain at the access site, are taken into account, the overall complication rate is estimated to be approximately 5%–8%.6,14 Regarding long-term patency, the AbreTM stent exhibited a high primary patency rate, with only 1 out of 14 patients who underwent imaging follow-up demonstrating non-occlusive thrombus, and only 2 patients requiring re-intervention. The low rates of re-occlusion and re-intervention seen in this study align with those reported in the literature3,7,14 highlighting the effectiveness of the AbreTM stent for SVC syndrome.
There were several limitations to this study. The retrospective design limits comparison between the AbreTM venous stent and other types of stents, as stent selection, sizing, and positioning were at the discretion of the attending interventional radiologists involved in the procedures. Clinical follow-up to assess for resolution of symptoms of SVC syndrome post-stenting were also not standardized and limited to available documentation in the electronic medical record. In addition, the study is limited by its small sample size, which did not allow for comparison of stent efficacy between malignant and non-malignant causes of SVC syndrome. In addition, the small sample size may have been insufficient to assess the risk for complications related to the AbreTM stent given that complications are uncommon at baseline.
In summary, the results of this study suggest that the AbreTM venous self-expanding stent is safe and effective for treatment of SVC syndrome. Our study provides an initial assessment of a cohort of SVC syndrome patients from 2 academic medical centers and demonstrates excellent technical and clinical success in using the AbreTM stent to alleviate SVC obstruction, maintain SVC patency, and improve clinical symptoms.
Footnotes
Author Contributions
TJA and SLM collected the data. TJA, AA, OZ, AC, MSS, YE, EB, KD, and SK performed the procedures. TJA and SLM wrote the manuscript. All authors reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Consent for publication was not obtained due to the retrospective nature of the study.