
Abstract
The current state of the literature for a bullet embolization to the heart and/or pulmonary vasculature indicates the occurrence is rare but could increase due to the rise in civilian low-kinetic-energy firearm acquisition and use. We present the case of an older teenage male who sustained a gunshot wound to the left flank. The bullet entered the iliac vein, travelled through the heart and lodged in the pulmonary artery. Successful relocation of the bullet to the internal iliac vein was performed by the interventional radiologist. This article highlights the advancement of interventional radiology as a successful non-invasive endovascular technique for bullet embolus removal.
Background
The occurrence of U.S. civilian shootings has risen dramatically in the 21st century.1-9 Since 2014, gun related injuries have risen on average 1000 occurrences per year.
10
(See Figure 1) Alarmingly, firearm related fatalities increased 58% from 2000 to 2020.1-5,9 Until recently, penetrating firearm injuries were more associated with military situations. However, as the occurrence of civilian shootings has increased, without the use of body armor, the incidence of fatal and non-fatal firearm related injuries have increased.6-8,11 The younger adult population aged 17 to 25 are associated with the majority (80%) of firearm related homicides which affects a disproportionally larger amount of the African American male population.1,3 In the U.S., nonfatal firearm related injuries rose approximately to half a million (422,907) incidents in the 5 years between 2010 and 2015.3,4,10 Graph of yearly gun related deaths and injuries.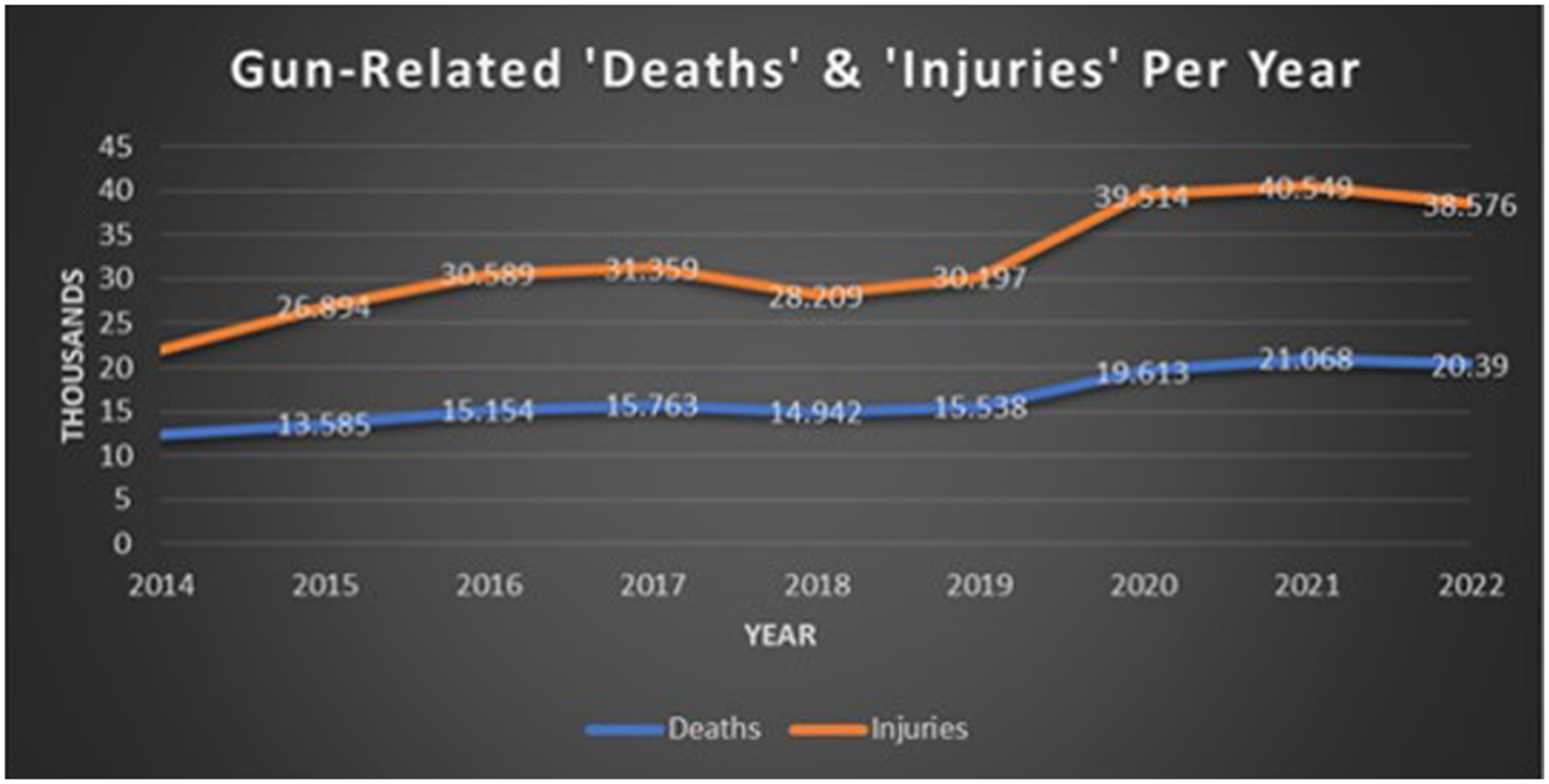
Air pellet injuries should also be considered in the umbrella of firearm-related injuries and can cause significant injury and mortality. Societal appreciation of injuries from air pellets is low, causing the use to expand and be accepted as an enjoyable minimal risk past time. The expanding force of compressed air propels the projectile down the barrel and technological refinements have increased the velocity and power of these weapons leading to serious and fatal injuries.12-14
The energy imparted and thus the type of wound incurred is related to a bullet’s mass and velocity. In general, rifle caliber ammunition tends to be of higher velocity, and often strikes, enters, and exits the body resulting in a straight line of travel. Conversely, pistol caliber ammunition, generally associated with civilian-type weapons, tends to be of lower velocity, often not exiting the body or traveling in a straight line within tissue and complicating the management of patients with complex traumatic injuries when the bullet does not follow the expected trajectory.11,15-17 With low-kinetic-energy weapons, the bullet or emboli pierces tissue upon entering the body, then rapidly loses energy. As the bullet travels, enough energy is sustained to penetrate and house itself within the vasculature resulting in the ability to embolize.11,15-17
Bullet embolizations into the vascular are unusual and, in the past, were associated with military engagements resulting in death when locating into the pericardium.7,18,19 As cases of gun-related bullet vasculature emboli have risen, the use of a developed protocol may formalize and support directional care. A search retrieved from https://pubmed.ncbi.nlm.nih.gov/using the terms “bullet emboli” and “bullet embolus” revealed a total of 90 reported cases of bullet embolizations reported from 1995 to 2010 but increased to 141 for the 12 years from 2011 to 2024. (See Figure 2) A bullet embolus lodged in the pulmonary artery is even more rare but has also increased over the past decade. From 1995 to 2010, 15 pulmonary artery bullet emboli cases were reported but almost doubled to 27 from 2011 to 2024 with 53% lodging in the right ventricle and 32% in the pulmonary artery tree. The concern is the upward trend and the probability of the cases being underreported, making the capture of accurate data difficult.8,20,21 Tracking bullet embolizations may become necessary with the increase in low-kinetic-energy firearm related injuries in the civilian setting.8,21 Bullet emboli graph.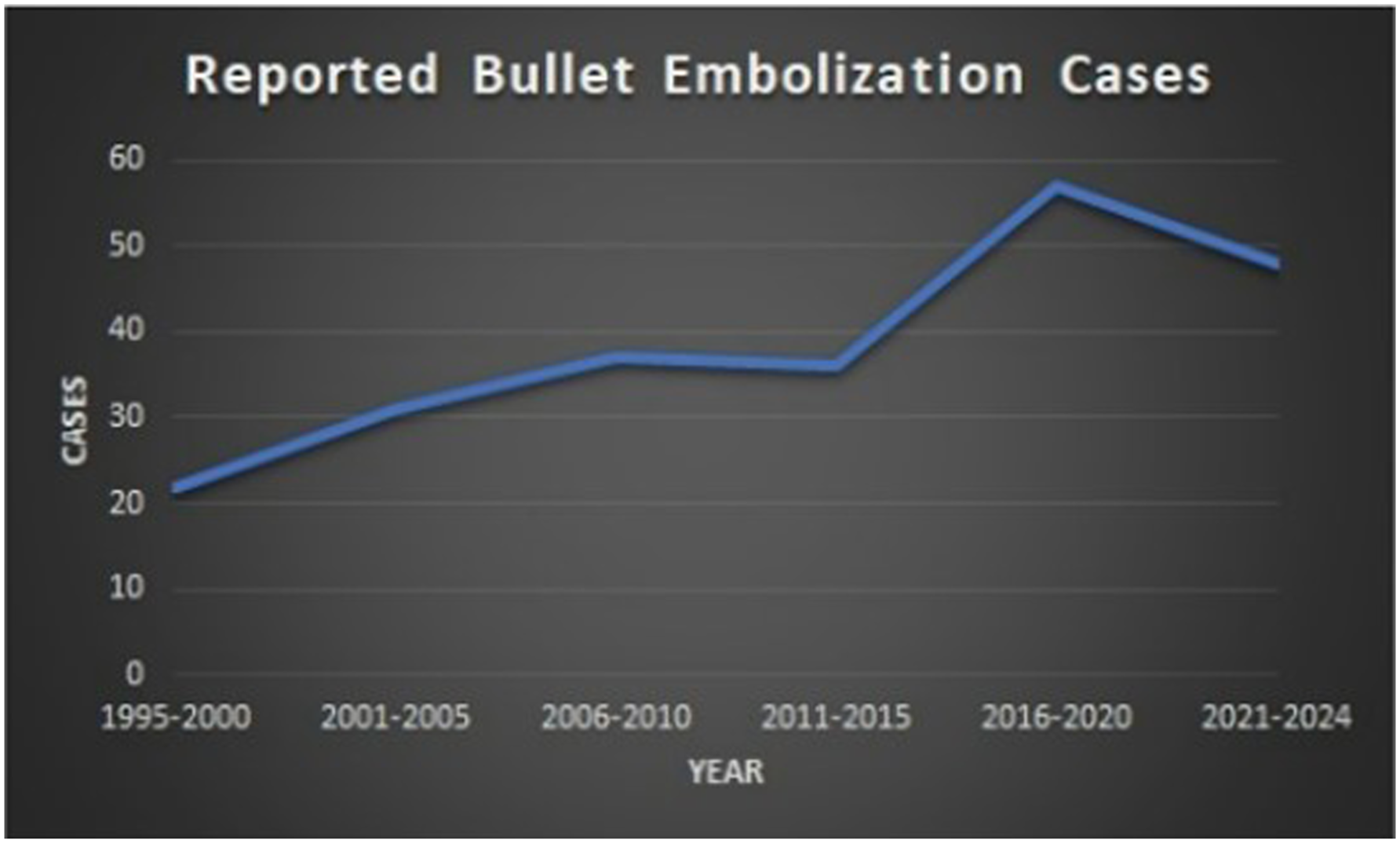
This is a case presentation of a male who suffered a low velocity gunshot to his left flank which resulted in the bullet entering the iliac vein. The bullet then embolized through the inferior vena cava and heart, ultimately resting in his pulmonary artery. The patient was contacted and made aware of the request for his case publication and gave informed consent.
Case Presentation
The patient was an African American male in his late teens who presented to our level 1 trauma center by private vehicle after sustaining a gunshot wound to the lower left flank. The patient was driving when accidentally shot by a passenger in the back seat. He arrived hemodynamically stable complaining of low back pain. His primary survey was unremarkable. The secondary survey was significant only for a gunshot wound to the left lumbosacral area with minimal active bleeding. No other wounds were identified. While in the trauma bay, a Focused Assessment with Sonography in Trauma (FAST) was performed and on the initial cardiac view of the exam, an echogenic foreign body was thought to be visualized, but could not be identified on subsequent views. A chest x-ray was then performed which showed a metallic foreign body (bullet) overlying the cardiac silhouette. He remained hemodynamically stable and neurologically intact throughout the initial evaluation in the trauma bay. He was subsequently sent for a computerized tomography (CT) scan of the chest, abdomen, and pelvis with intravenous and rectal contrast.
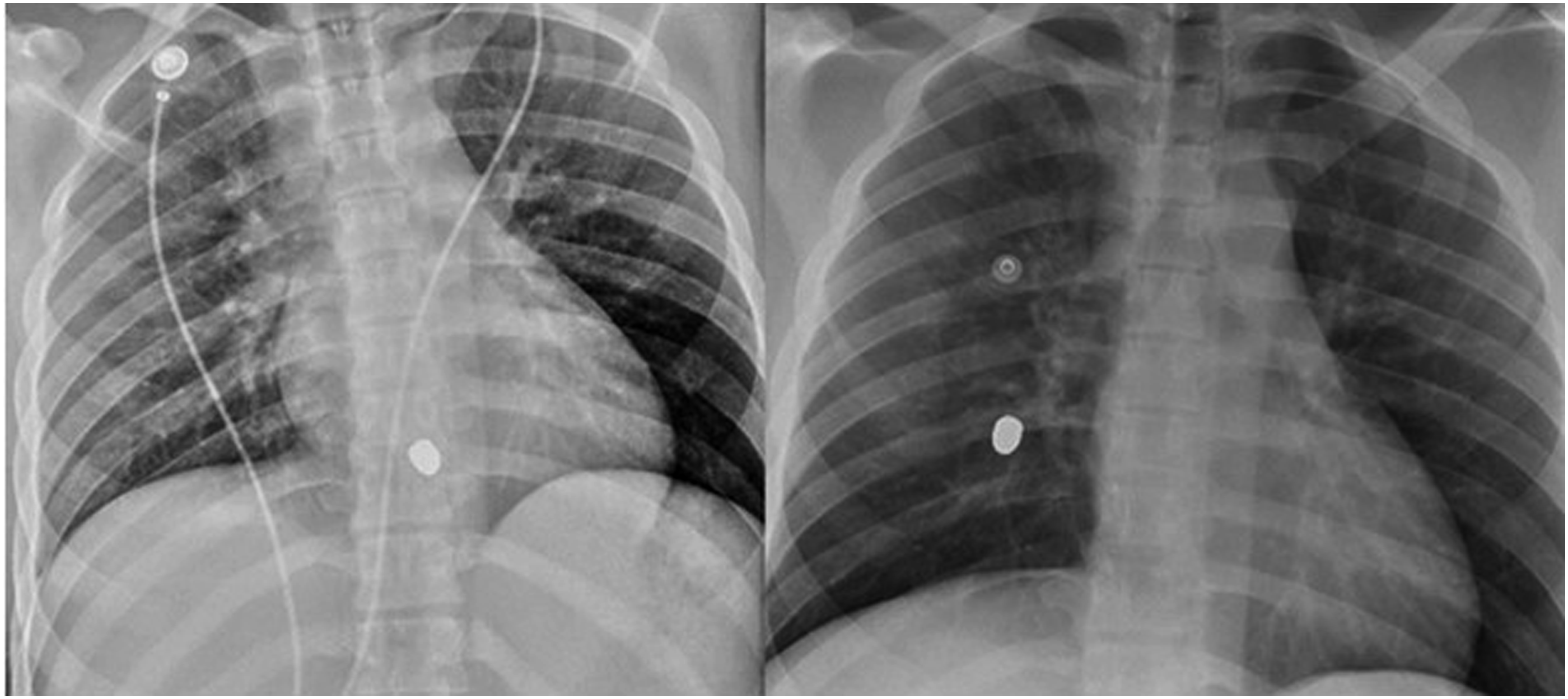
The CT scan demonstrated a soft tissue injury at the level of L5/S1 with associated S1 and S2 fractures and a large pelvic hematoma. No rectal contrast extravasation was seen. A retained projectile was identified in the chest that appeared to be anterior to the left ventricle but was difficult to precisely localize due to metallic streak artifact. No pericardial effusion was identified and no bullet tract between the pelvis and chest could be identified. (See Figure 3) Due to the concern for possible cardiac injury, a bedside echocardiogram was performed. No pericardial effusion, wall motion abnormality, or bullet was identified. A repeat chest x-ray was performed which showed that the projectile had migrated to the right lung since the initial chest x-ray, (See Figure 4), confirming a bullet embolus. Cat scan image. CXR Image.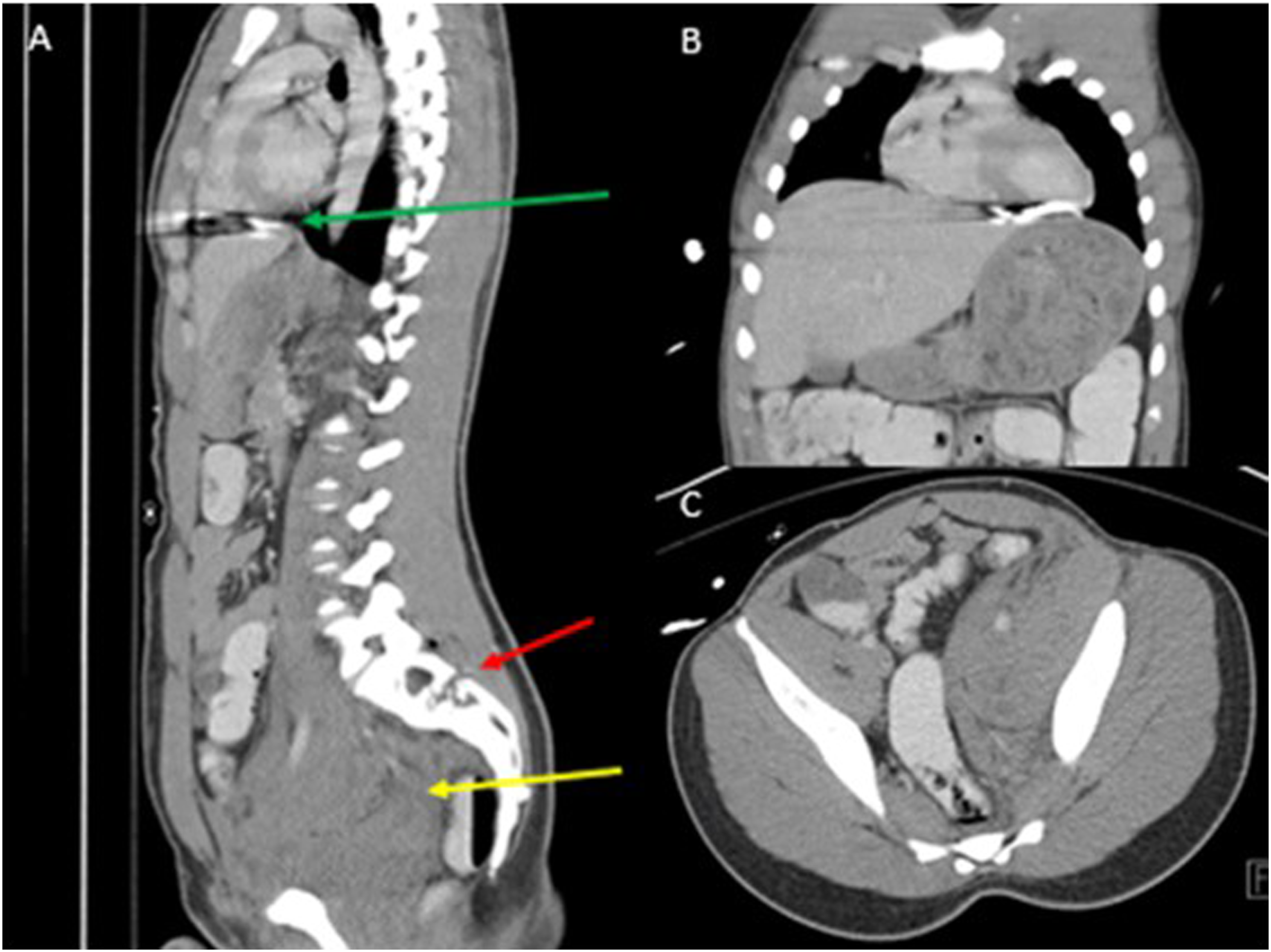
To better localize the bullet, a CT angiogram of the chest was performed (See Figure 5) which showed the projectile now located in the right lower lobe pulmonary artery. There was no associated pulmonary infarction, and the patient remained asymptomatic; however, there was diminished opacification of the right pulmonary artery and its distal branches relative to the rest of the lung. A formal echocardiogram was performed which showed normal systolic function and no evidence of right heart strain. A cardiothoracic surgeon and an interventional radiologist were consulted for assistance in management. After reviewing the case, both physicians determined the projectile should be retrieved to avert possible impending pulmonary infarction and non-surgical retrieval of the embolus would be attempted first. CT Angiogram of chest.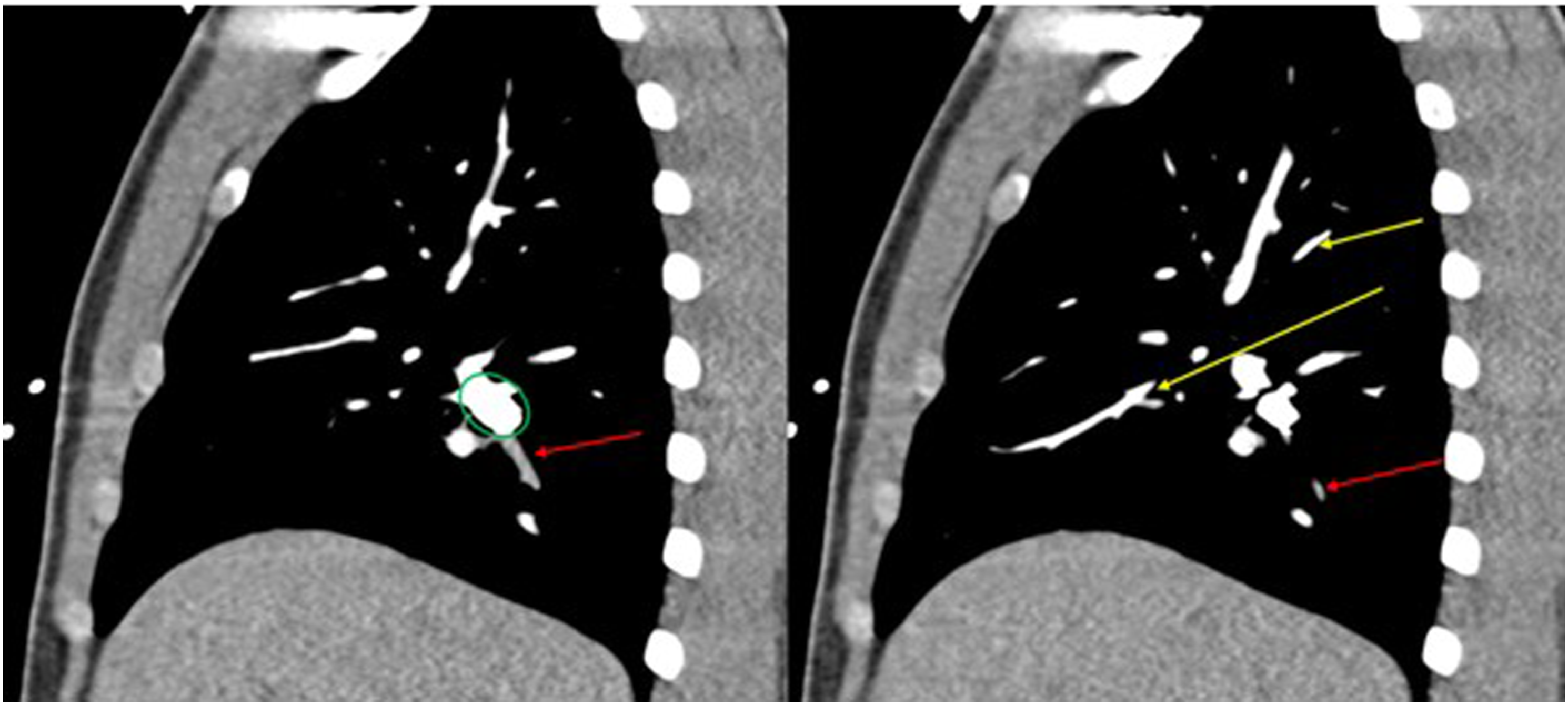
After the risks/benefits of the procedure were discussed and informed consent was obtained, the patient underwent percutaneous retrieval of the projectile by the interventional radiologist. The procedure was technically difficult due to the relatively small diameter of the right lower lobe pulmonary artery in relation to the projectile, however removal of the bullet from the pulmonary artery was eventually accomplished using a 15 mm gooseneck snare via the right common femoral vein. (See Figure 6) The projectile was successfully withdrawn into the right common femoral vein while an occlusion balloon was placed in the IVC via the left common femoral vein. During removal through the venotomy, the bullet released from the snare, migrating into the right internal iliac vein due to retrograde flow from the occlusion balloon. Attempts were made to retrieve the projectile from the right internal iliac vein, but this was unsuccessful. At this point, the decision was made to leave the projectile in the right internal iliac vein where it was of no clinical consequence. Two 14-millimeter vascular plugs were placed in the right internal iliac vein to prevent future embolization of the projectile (See Figure 6). Placement into right internal iliac vein with vascular plugs.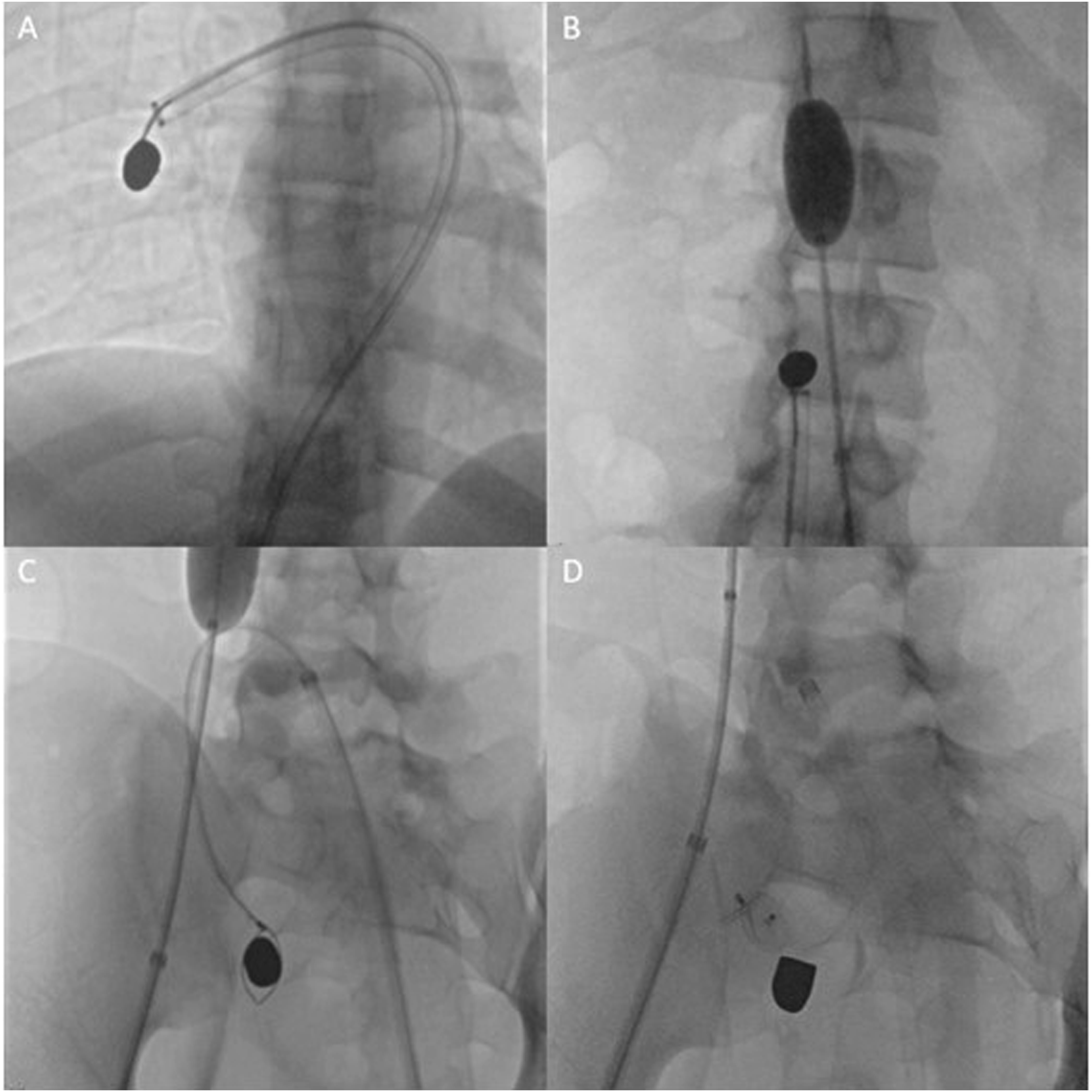
The remainder of the clinical course was uncomplicated except for acute blood loss anemia (hemoglobin and hematocrit dropped to 6.6/17.9). The patient required the transfusion of 2 units packed red blood cells. His hemoglobin stabilized after the transfusions and no further intervention was required. Low molecular weight heparin prophylaxis was started on post-procedure day 2. He was managed non-operatively from an orthopedic standpoint for the sacral fractures and did well with physical therapy. He was able to ambulate with a walker and was discharged home on hospital day 4.
Discussion
The patient met the national pattern as a firearm injury recipient. He was an older teen, African American, and shot with a handgun. The patient also met the criteria of being a younger, productive individual sustaining injury in more than one system which compromises 40% of patients arriving to trauma centers in the U.S. 22 The multiple system injury patterns require the attention of a generalist traumatologist and sub-specialty physicians who are actively engaged as needed.22-24 Early consultation is advisable as consulting specialists may have requests or recommendations regarding specific imaging modalities. 24 As in this patient’s case, the subspecialists (orthopedist, interventional radiologist, and the cardiovascular surgeon) were included in the care in a timely manner for optimal care coordination and management.20-24 Effective and open dialog with consulting specialists is paramount which became evident in this patient’s case as the interventional radiologist and the cardiovascular surgeon reviewed the case together and agreed on the endovascular approach as the first tier and the open approach as the second tier if needed. 22 The combination of musculoskeletal trauma (sacral fracture) with associated iliac vein injury and pulmonary artery embolus is a complex injury that is best treated at a trauma center by personnel who have experience with challenging cases. 22 Orthopedic surgeons are commonly involved with polytrauma patients suffering skeletal injuries and manage patients with pelvic injuries which have high incidence of hemorrhage such as this patient who developed of a large sacral hematoma ultimately requiring blood administration and physical therapy management. 22
Commonly, as in this case, the patient can remain asymptomatic. 15 However, in approximately one-third of the patients, if migration to the heart or pulmonary vessels has occurred, the patient can present with dyspnea, chest pain, and hemoptysis necessitating urgent or emergency intervention.15,18,19,21 This patient remained asymptomatic but was at risk for life-threatening pulmonary infarction and pulmonary artery erosion associated with bullet embolization in younger ages. 25 Migratory travel within the body can vary. A 5-year case review from 2019 to 2023 retrieved from https://pubmed.ncbi.nlm.nih.gov/under the search terms “bullet emboli” and “bullet embolization” revealed the sporadic nature of 55 cases of embolic vessel travel. The emboli lodged in multiple areas: pulmonary artery (12); extremity artery (7); mesenteric artery (1); hepatic/renal/iliac vein (10); heart and surrounding veins (13); head/neck (12). Of these, 8 were air-pellet related. Bullets entering through a large vessel, such as via an iliac, renal, or hepatic vein, and traveling to the right atrium can cause chordae tendineae damage and/or arrhythmias to occur.18-20,26 Sarmast et al reported a case of grenade chip migrating to the heart causing a torn anterior common chordae and a perforated anterior leaflet requiring repair. 2 Location dependent, a bullet embolus can result in sepsis, arrhythmias, ischemia, endocarditis, cardiac valvular incompetence, stroke, pulmonary embolism, heavy metal poisoning and arthropathy if left near joints.15,19,26-31 Bullet retrieval located in proximity to the hip joint after 35 years was reported by Rohlfing et al. 31 The patient developed chronic systemic lead toxicity when intra-articular ballistic fragments were retained leading to the development of a pseudotumor. 31 Recent cases have reported unusual migration including smaller pellet gun and metal bullet fragments. Clouse et al described a bullet fragment migrating to the intracerebral circulation causing stroke-like symptoms. 28 Pulsation of an artery against a bullet or fragment can also cause gradual erosion of a vessel and later allow the embolus to enter the arterial system causing arterial embolization, limb, cerebral, or ocular ischemia.15,18 Hussain et al described the retainment of a bullet in the leg in near proximity to an artery which eroded the lumen over time and migrated 10 years later to the heart. 32 The emboli can also enter the venous circulation but end up paradoxically in the arterial circulation thru a patent foramen ovale or another cardiac defect.15,21 There are also reports of projectiles eroding into nonvascular structures, including the urinary bladder and trachea, many years after the initial injury.33-35
Long-term follow-up is scarcely documented. The most qualified study was a 20-year follow up of 40 World War II veterans with bullets/fragments ranging from a few millimeters in diameter to .30-caliber machine-gun bullets. 36 Multiple fragments were found in the myocardium of 3 patients. Most (33) of the missiles were in the wall of the ventricle and one remained in the pulmonary artery. One soldier did incur a mitral valve injury. And one solder had subsequent erosion 15 years later from the pulmonary artery into the adjacent bronchus. Pericarditis and effusion did occur in 25% of the cases. Of the 40 soldiers, 29 returned to full-time work. Two other separate patient-case follow-ups documented the exhibition of no symptoms at 6 months and 1 year.37,38
Commonly, the patient is lost to follow-up as in this patient’s care. 21 The patient returned to the emergency department twice for complaints of low back pain but did not follow up with the orthopedist. The patient also sought urological care for hematuria but refused an outpatient work up. The hematuria complaint was not mentioned on the following emergency department visits. Regularly scheduled follow-up is vital to identify potential complications, but follow-up cannot be mandated and is at the mercy and discretion of the patient and family. Because of scarce follow-up documentation, long-term imaging recommendations are unavailable. 29
Imaging
Due to the loss of energy inside tissue, the shorter and more erratic travel of lower-kinetic-energy bullets allows direct entrance into the venous system. 15 Entrance wounds occurring without an exit wound allow for the possibility of bullet embolization, especially if the final trajectory does not match the expected line of travel.8,15 If shot multiple times, with imaging demonstrating multiple metallic foreign bodies in various locations, the clinician should have a high suspicion for possible bullet migration. Identification of the bullet location becomes a priority, especially if potentially traveling through the vasculature.8,15,25,38
Multimodal imaging is crucial to identify a bullet’s trajectory and is essential for the patient’s workup. 11 Identifying potential structural damage of tissues is paramount in a trauma patient. 16 In bullet emboli cases,significant migration can occur in as little as 13 minutes. 25 Most commonly, a chest X-ray is performed to quickly identify bullet location, as in this patient’s case, especially if the patient is experiencing cardiopulmonary symptoms. 15 The chest x-ray does not have precise spatial resolution but can reveal the bullet ‘s general location. 15 The multidetector computed tomography scan (CT) which provides cross-sectional imaging and superior anatomic localization is the most valuable imaging modality to evaluate patients with thoracic trauma and is used to assess hemodynamically stable patients with suspected cardiac involvement. 3 The CT images allow spatial, contrast, and temporal resolution with a fast and accurate examination of the entire chest, including the heart, pericardium, and great vessels. 3 Serial scans, which occurred in this patient’s case, with the performance of arterial or venous phase imaging may be required to identify the bullet’s exact anatomic location. 38 Other imaging procedures that may be used to identify the bullet’s location may include transesophageal and transthoracic echocardiography, nuclear medicine and magnetic resonance imaging. 38 The discordance between the entry wound and the bullet’s location in this case caused high concern for embolization, causing the patient to have repeated chest x-rays, a multidetector CT, and an echocardiogram to evaluate for any potential damage that could have occurred.
An echocardiogram is used as a primary screening tool to evaluate for blunt cardiac injury and can depict abnormalities suggestive of hemopericardium, cardiac tamponade, traumatic ventricular septal defect, valvular damage, aneurysm development, or intracardiac thrombus. It also permits the evaluation of myocardial echogenicity and focal systolic hypokinesis. 38 The echocardiogram can help identify the bullet location and can aid in selecting the appropriate therapeutic option when cardiac trauma has occurred. A transesophageal echocardiogram can be performed to identify intracardiac anatomy and function, aortic or cardiac valve injury, pericardial effusion, myocardial contusion, atrial laceration, and cardiac valve injury. 38 Electrocardiography and cardiac biomarkers can also be performed to discern cardiac damage which this patient did receive but were negative for abnormalities. 38
Removal of the Bullet or Fragment
Establishing clear guidelines for the removal of bullet emboli has been difficult due to the infrequency and variable geographic occurrence and rare follow-up documentation. 8,15,25,29 More of the geographic regions associated with reporting bullet emboli are regions which have increased firearm related injuries such as the Middle East and the U.S. General considerations for removal by an interventional radiologist include the venous location, ease of access, bullet or fragment size, risk of infection, stroke, hemodynamic effects, arrhythmia or neurological sequalae.11,15,25,32 When safe bullet removal is not feasible or emboli is small and asymptomatic, conservative management with special attention given for possible complications is practical. 15 Generally, bullets in tissue without impingement on vital structures do not require removal. 15 For cardiac embolization, if the patient is asymptomatic, the bullet or fragment is smooth, less than 5 mm, and is firmly lodged in the right side of the heart, non-removal may be appropriate. Over time, the bullet or fragment has the possibility of becoming epithelialized. 15
As care has progressed, survival rates have increased. Removal of bullet emboli by an endovascular approach has emerged as a safe and feasible option when tailored to the patient’s clinical situation, and the expertise is available .8,15,18,21,26,29,32,37 A combination of methods may be required.11,39,40 For this individual patient, a 24 French access sheath was placed in the groin. A 20 French aspiration catheter was used as a guide sheath allowing advancement across the right ventricular and pulmonary outflow tract using standard endovascular techniques. A separate guidewire was left in place to support and stabilize the sheath in the pulmonary artery. A 15 mm gooseneck snare catheter was used, with the wire loop snare carefully manipulated around the base of the bullet in the pulmonary artery. Once retrieved, the ensnared bullet was carefully withdrawn through the pulmonary artery and cardiac chambers.
As of date, three algorithms have been proposed for bullet emboli management.7,8,40 The authors stress the need for individualized treatment warranted by careful consideration of all factors. Miller et al focused on location and symptoms.
40
Yoon et al focused on thoracic cavity embolisms while Kuo et al proposed management of emboli based on the left vs right side of circulation.7,8 Having an active interventional radiology program with clinical expertise, and considering each algorithm, we expounded on the algorithm developed by Miller et al focusing on the management of all emboli.
40
(See Figure 7) Bullet emboli management algorithm.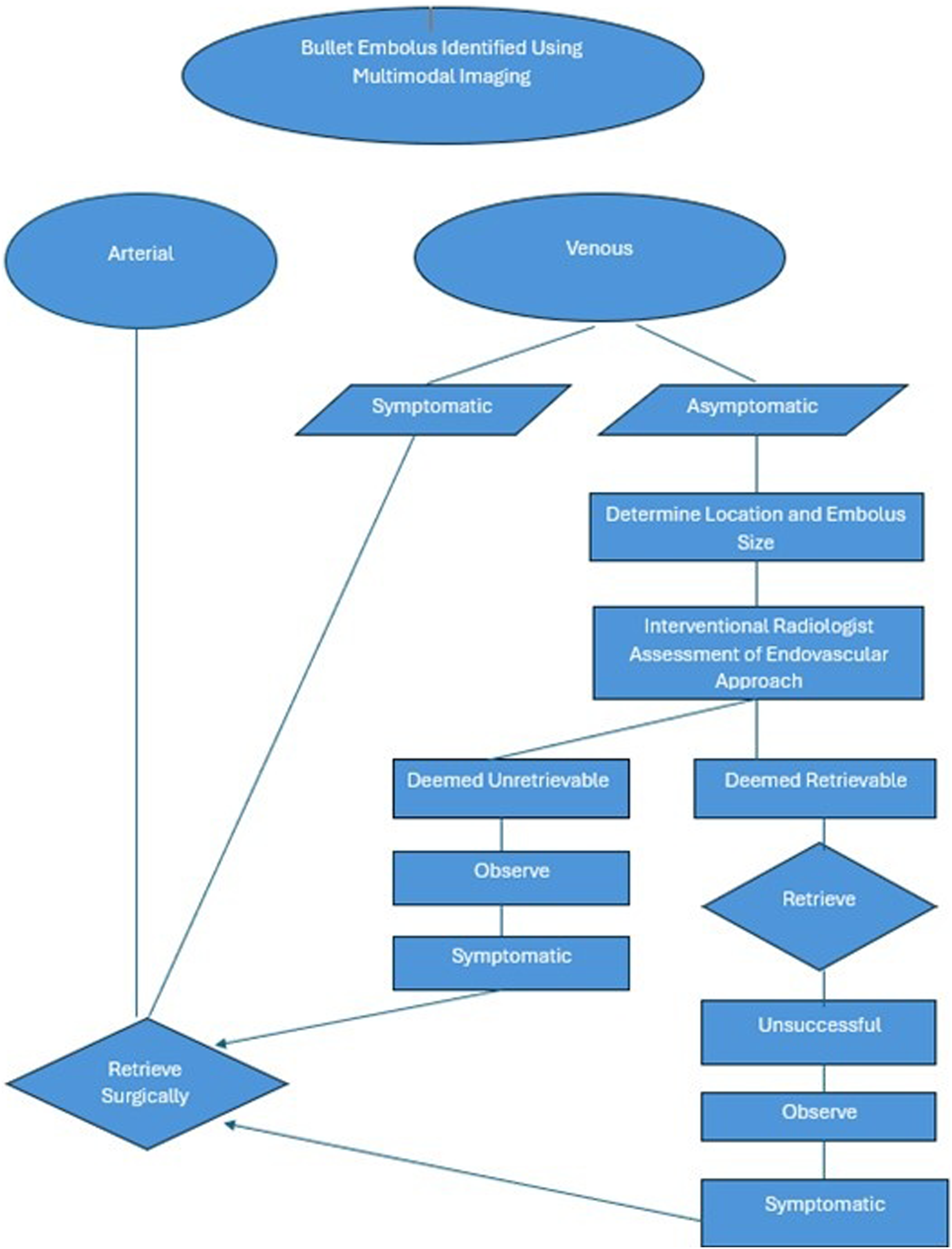
Conclusion
As shootings increase, the varying type of firearm injuries seen in the civilian setting will intensify. Potential bullet or fragment removal by an interventional radiologist should be an available option in a trauma program. Economic and quality of life experience should factor into the impact of clinical decisions when considering interventions for patients with injuries that can be managed with endovascular procedures rather than open surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.