
Abstract
Background
Extracorporeal membrane oxygenation (ECMO) through the femoral artery and vein can lead to significant vascular complications. We retrospectively studied the acute vascular complications of Veno-Arterial Extracorporeal Membrane Oxygenation (VA-ECMO) in COVID-19 patients compared to non-COVID patients during the period from January 2020 to July 2023.
Results
Seventy-eight patients underwent VA-ECMO for various indications from January 2020 to July 2023. The studied patients had a mean age of 59.6 ± 6.9 years for non-COVID patients (38 patients), and 62.2 ± 7.6 years for COVID patients (40 patients), with a P = 0.268. In non-COVID patients, The baseline characteristics were similar in both groups. The primary indications for ECMO were cardiac diseases, followed by respiratory failure (78.9% vs 10.5%). Conversely, in COVID patients, respiratory failure due to COVID-19 infection was the main indication (45% vs 40%). The overall incidence of general complications, including cerebrovascular stroke, acute kidney injury, intracardiac thrombi, and wound infection, was comparable in both groups (31.6% vs 45%). The overall incidence of vascular complications in both groups was 33.3%. Ipsilateral acute lower limb ischemia occurred in 5.3% vs 10% of non-COVID and COVID patients, respectively. Thrombosis of the distal perfusion catheter (DPC) occurred in 10.5% vs 15%, respectively.
Conclusion
During the COVID-19 pandemic, an increasing number of patients required VA-ECMO due to associated respiratory failure. Patients undergoing VA-ECMO are at high risk of developing various vascular complications. COVID-19 significantly increases the risk of acute limb ischemia and distal perfusion catheter thrombosis in both upper and lower limbs. However, other VA-ECMO-related vascular complications are comparable between COVID-19 and non-COVID patients.
Keywords
Introduction
Extracorporeal Membrane Oxygenation (ECMO) is a type of life support used in severely ill individuals with severe respiratory or cardiovascular failure. This method diverts blood from the patient’s veins, pumps it across a synthetic membrane to add oxygen and remove carbon dioxide, and then returns it to the patient’s arteries. Extracorporeal membrane oxygenation (ECMO) is the sole method for temporary support for cardiopulmonary functions. It was first described by Hill et al, in 1972 1 Since then, it has gained popularity and established itself in managing cardiac conditions. 2009 it was used for respiratory failure during the H1N1 pandemic. 2 Recently several articles have highlighted its importance in managing respiratory failure associated with coronavirus disease 2019.3-5
While VA-ECMO is a crucial lifesaving technique, it carries significant morbidity and mortality risks. Two major types of complications associated with VA-ECMO are vascular and neurological. Vascular complications refer to problems arising from changes to the blood vessels due to the use of VA-ECMO, such as clots, bleeding, or vessel injury. Neurological complications refer to problems related to the nervous system, such as stroke, seizures, or brain injury, which can arise from a range of factors, including blood flow changes, hypoxia, and clotting. While VA-ECMO can save lives, vigilant patient monitoring and meticulous complication management are essential to enhance outcomes. 2
Vascular complications remain the primary determinant of prognosis. Acute limb ischemia (ALI), arterial dissection, thrombosis, pseudoaneurysm formation, and hemorrhage represent the main cannulation-related complications and are leading causes of mortality. Cannulation of the femoral artery, with reduced blood flow below the cannulation site, may result in ipsilateral limb ischemia.6-8 Acute limb ischemia is the most common vascular complication, with an estimated incidence ranging from 10% to 70%, associated with higher mortality and morbidity rates among survivors after decannulation procedures.9,10
Several risk factors have been suggested in the literature, including age, gender, diabetes mellitus, peripheral vascular diseases, and previous cerebrovascular disease. However, there remains insufficient evidence regarding COVID-19 infection as an independent risk factor for vascular complications in patients undergoing VA-ECMO.2,11 The study compares the management and outcomes of complications in COVID-19 vs non-COVID-19 patients undergoing VA-ECMO, providing insights into their incidence, severity, and potential strategies for management and prevention to enhance patient outcomes. The primary endpoint of this study is the incidence of acute vascular complications, including ipsilateral acute lower limb ischemia and thrombosis of distal perfusion catheters, in COVID-19 and non-COVID-19 patients on VA-ECMO.
Methods
After approval from the local ethics committee, a retrospective cohort study was conducted in a single center (Vascular Surgery Unit, Adan Hospital, MOH, Kuwait), including all patients who required VA-ECMO during the period between Jan 2020 and July 2023. Inclusion criteria encompassed all indications for VA-ECMO insertion. Exclusion criteria comprised patients with pre-existing symptomatic arterial vascular diseases necessitating vascular intervention before VA-ECMO insertion. Additionally, patients who succumbed to causes unrelated to ECMO-related vascular complications were excluded from the study. Furthermore, patients on venovenous ECMO, patients who were originally on venovenous ECMO and then developed cardiogenic shock requiring transition to VA-ECMO, and patients with heparin resistance due to antithrombin III deficiency were also excluded from the study. The enrolled patients were divided into 2 groups based on their current COVID-19 infection status: non-COVID group and COVID group. Demographic data, associated comorbidities, drug history, and laboratory tests were collected from medical records. The clinical data of the patients were analyzed using the Chi-square test for categorical variables. For laboratory data, non-parametric variables were examined using the Kruskal-Wallis equality-of-populations rank test, while parametric variables were assessed using the ANOVA test.
The primary objective was to compare the incidence and types of vascular complications between both groups. Vascular complications were defined as new vascular events occurring after VA-ECMO initiation, including: 1) acute limb ischemia, 2) reperfusion cannula-site thrombosis or bleeding, 3) arterial dissection, 4) pseudoaneurysm formation, and 5) venous thrombosis. Secondary objectives included comparing the incidence and types of general complications, the incidence of wound infection, and overall mortality between the 2 groups.
The Procedure of Cannulation and Decannulation of Femoral Artery and Vein
All cannulation procedures were percutaneously performed bedside, US-guided Seldinger aseptic technique except for 2 patients who required surgical exploration. Cannulation to the femoral vein, 19-24-Fr, was introduced over a guidewire till the level of inferior vena cava (IVC). The common femoral artery was cannulated with a 16-20 Fr cannula according to the size of the artery and the required ECMO flow, equivalent to a cardiac index (CI) of 2.2-2.5 L/m2/min. 12
Routinely, a distal reperfusion catheter (DPC) of 5-6 Fr was simultaneously placed in the proximal superficial femoral artery under ultrasound guidance and connected to the side port of the arterial cannula to maintain blood flow and prevent lower limb ischemia. 13 Blood flow on the ECMO machine was regulated based on mean arterial blood pressure, mixed venous oxygen saturation, and urine output. Inotropes and vasopressors were administered minimally to reduce the risk of peripheral ischemia. Continuous heparin infusion was administered to maintain a partial thromboplastin time of 45-55 seconds unless contraindications were present. 14 Vascular assessment was performed daily on all ECMO patients using clinical evaluation and Doppler ultrasound when clinically indicated. Based on clinical indications, all decannulation procedures were conducted in the operating room. Both common femoral arteries and veins were exposed, with control of the common femoral, deep femoral, and superficial femoral arteries. A routine thrombectomy using a Fogarty catheter (size no. 3) was performed in the distal superficial femoral artery for all patients upon decannulation. The common femoral artery was repaired with interrupted 6-0 polypropylene sutures, while the femoral vein was closed using 4-0 or 5-0 polypropylene sutures in a purse-string fashion. In 2 cases, patches were necessary to close the common femoral artery.
Statistical Analysis
Stata/SE © version 14.2 was used for statistical analysis. The Chi-square test was used to compare categorical variables. Mean and standard deviation (SD) were used to describe parametric variables, while non-parametric variables were described as median and interquartile range (IQR). ANOVA and Kruskal-Wallis tests were used to compare parametric and non-parametric numeric variables, respectively. Results were considered statistically significant if P < 0.05.
Results
Baseline Characteristics of Both Groups.
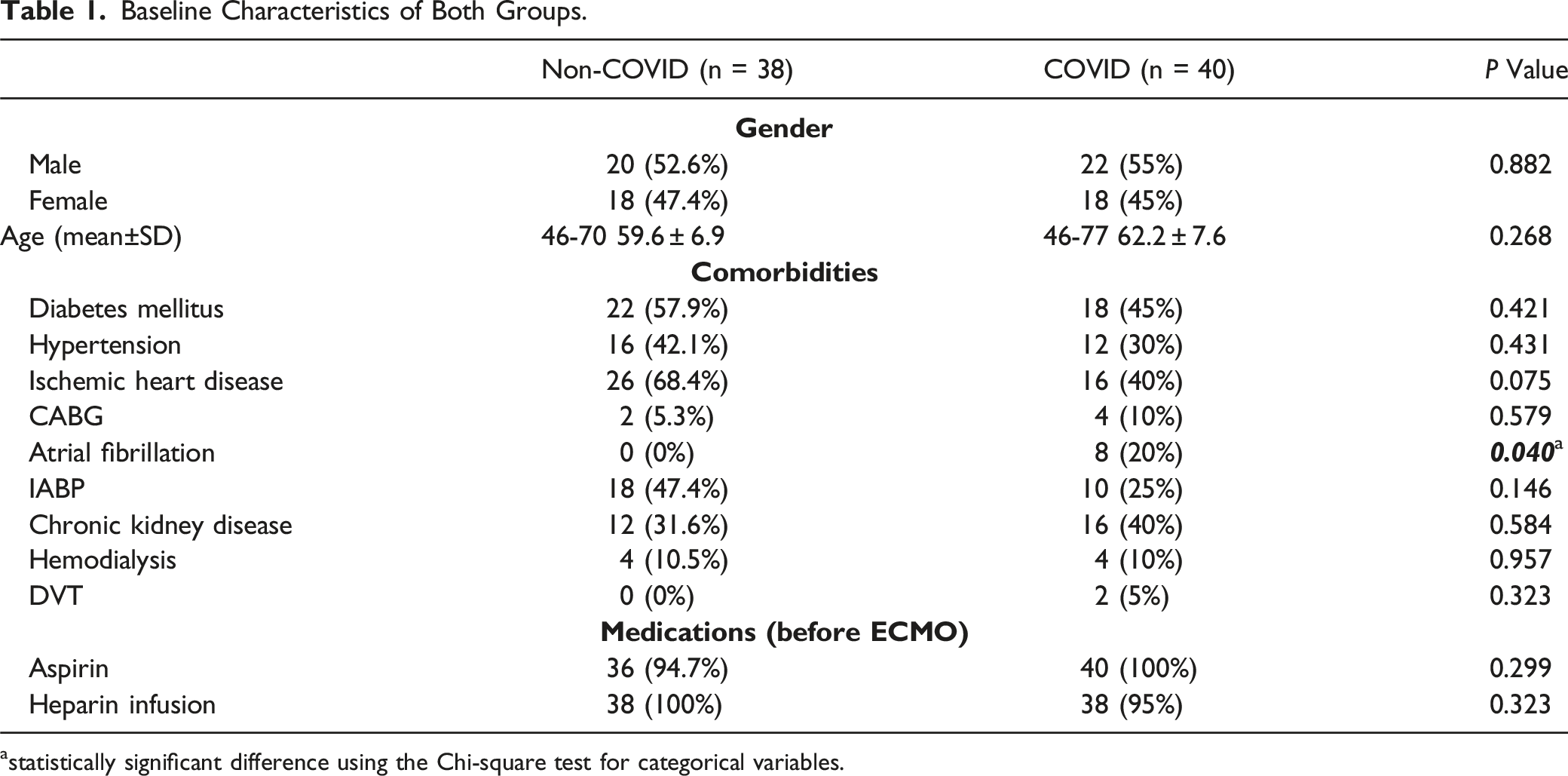
astatistically significant difference using the Chi-square test for categorical variables.
Baseline Laboratory Works of Both Groups.
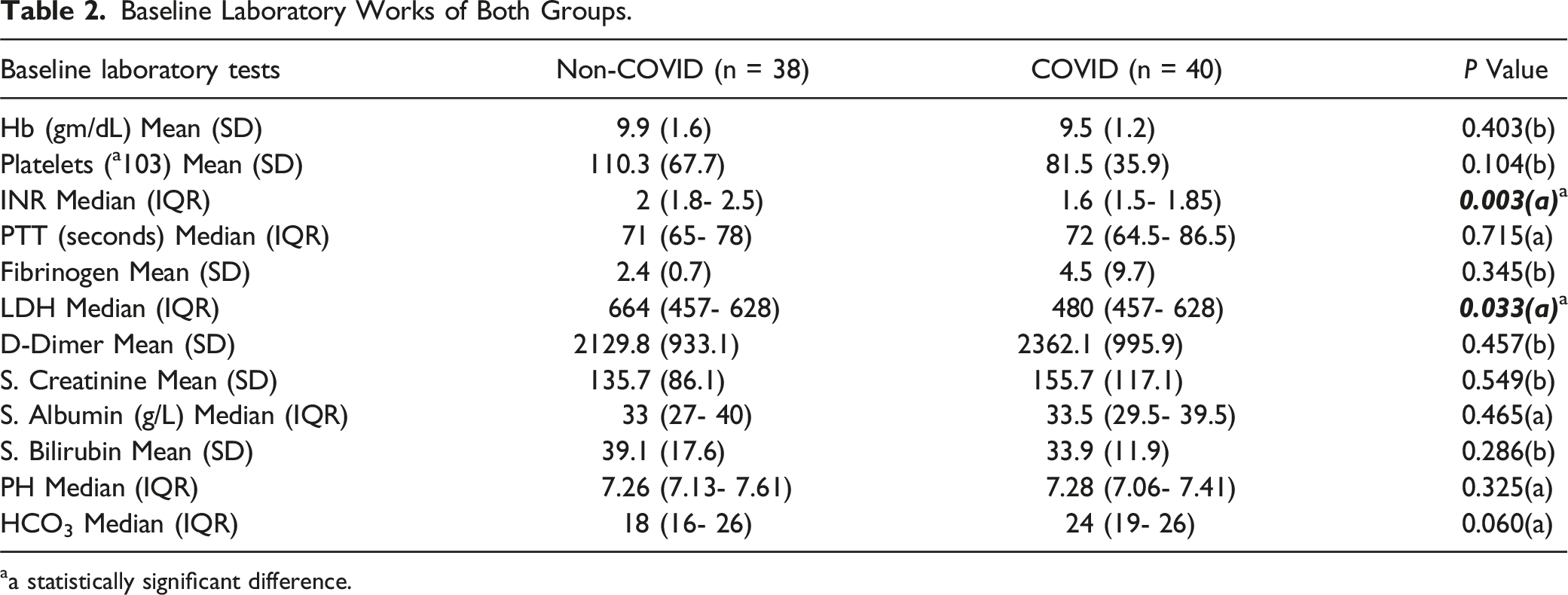
aa statistically significant difference.
Comparison Between Both Groups Regarding Indications of ECMO and ICU Admission.
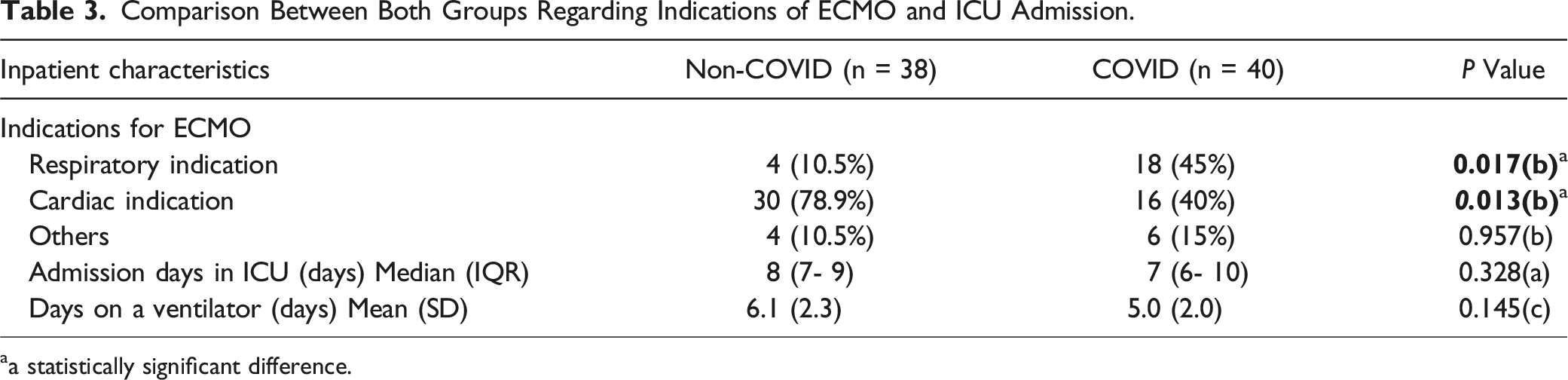
aa statistically significant difference.
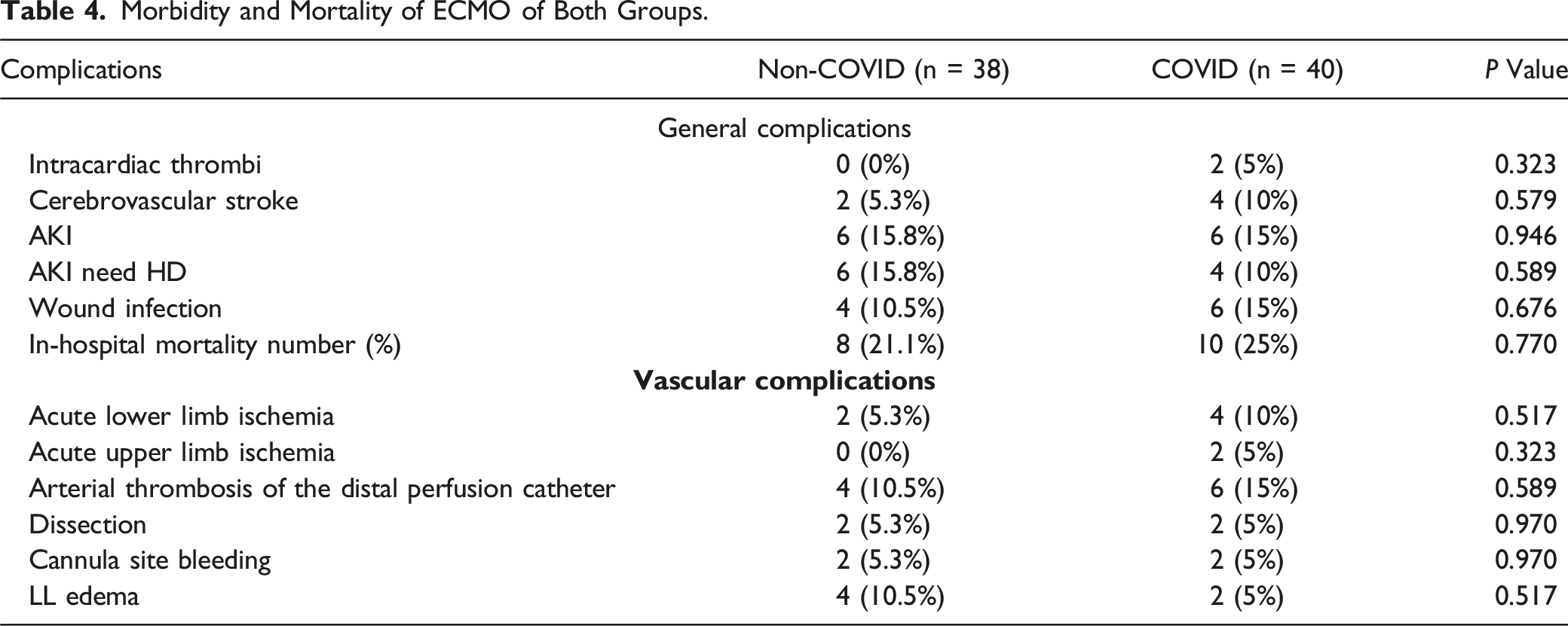
The overall incidence of general complications, including cerebrovascular stroke, acute kidney injury, intra-cardiac thrombi, and wound infection, did not show a statistically significant difference between the groups.” The difference was 13.4% (31.6% to 45%), which is relevant. Due to low sampling, the P-value was not<0.05. The wound infection was caused mainly by Gram-positive cocci and Candida albicans in non-COVID patients and by MRSA and Pseudomonas mirabilis in COVID patients.
The overall incidence of vascular complications in both groups was 33.3%. The overall incidence of vascular complications was 26.3% in non-COVID patients compared to 40% in COVID patients. Ipsilateral acute lower limb ischemia occurred in 5.3% vs 10%, respectively (P = 0.517). All of them had a thrombus during the thrombectomy, which was routinely performed for all patients. Interestingly in 2 patients, the thrombus was tubular, resembling the ECMO cannula shape, and consisted of fibrin and blood elements (Figure 1). Thrombosis of DPC occurred in 10.5% vs 15%, respectively (P = 0.589). Tubular-shaped thrombus resembling the ECMO cannula shape.
Interestingly, 2 COVID patients (5%, P = 0.323) had concurrent upper limb ischemia, without any connected catheters or cannulas, 1 day after developing ipsilateral acute lower limb ischemia. Two patients in each group developed profuse cannula-related bleeding (P = 0.970); however, only 1 COVID patient required surgical exploration and evacuation of the hematoma. Similarly, 2 patients in each group developed arterial dissection that necessitated surgical repair using a bovine patch during the decannulation procedure (P = 0.970).
Arterial pseudoaneurysm occurred in 1 COVID patient with myocardial infarction followed by severe groin infection after decannulation. CT angiography revealed active extravasation from a large pseudoaneurysm of the right common femoral artery (5*3.7*6.5 cm) that was completely sealed after the deployment of a covered stent (Figure 2). CT showed the right CFA pseudoaneurysm (5*3.7*6.5 cm) with extensive extravasation, wholly sealed after the deployment of a covered stent.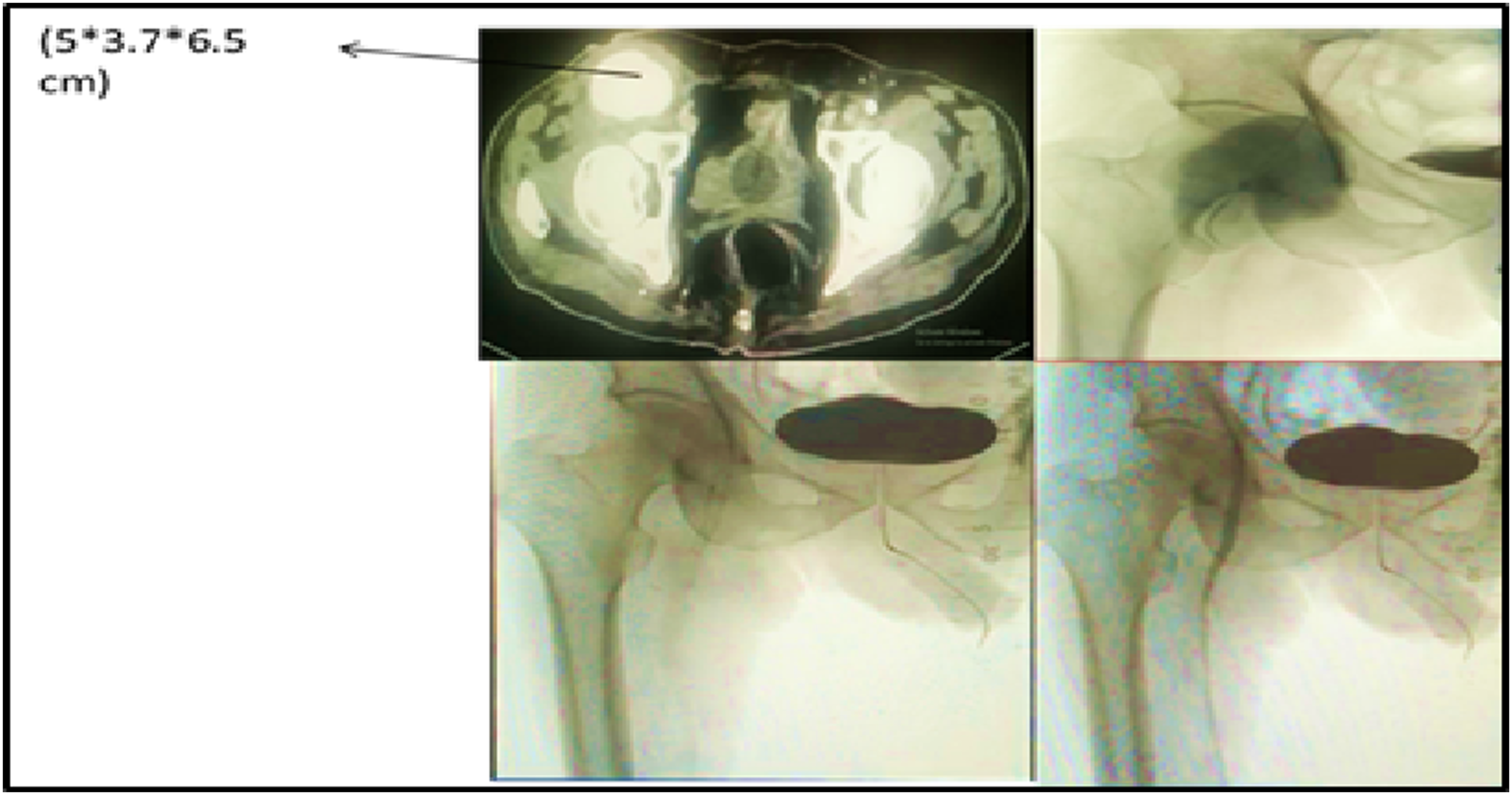
Morbidity and Mortality of ECMO of Both Groups.
Discussion
As far as we know, this is the first examination to compare the vascular issues post-ECMO in COVID-19 patients with those in non-COVID-19 patients. In general, the literature needs to include a more extensive discussion of vascular complications in COVID-19 patients who require VA-ECMO. SARS-CoV-2 infection is known to affect the respiratory system and cause multi-systemic effects. For instance, spontaneous gastrointestinal perforation has been described. 15 Moreover, multiple articles have suggested a strong association between COVID-19 and hypercoagulable status leading to arterial and venous thrombosis. 2 The associated cytokine storm with the viral infection is the accepted theory for the observed hypercoagulability, as it causes a thrombo-inflammatory state with endothelial dysfunction and activation of the coagulation cascade. 3 This theory is supported by previous observations of hypercoagulability status associated with other respiratory viruses such as severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1) and Middle East respiratory syndrome coronavirus (MERS-CoV).4,5 The high rate of thromboembolic events in anticoagulated COVID-19 patients supports the high viral thrombogenicity. In our study, vascular complications occurred in 33.3% of all patients. In the non-COVID patients, the overall incidence of vascular complications was 26.3%, while in COVID patients, vascular complications occurred in 40%. 3 Acute limb ischemia is the most reported arterial complication of SARS-CoV-2, reaching up to 15% of hospitalized COVID-19 patients, and it occurs on top of arterial thrombosis. 16 In COVID-19 patients, vascular complications have multiple features than in non-COVID-19 patients. Attisani et al reported that ALI could occur in COVID-19 patients with no known risk factors, such as elderly age, arterial fibrillation, peripheral arterial disease, trauma, and dissection.
Furthermore, hypercoagulability is initially not a risk factor for ALI unless associated with atherosclerosis. ALI can occur in multiple upper and lower limb arteries in 15% of COVID-19 patients, and ALI in COVID-19 patients has a higher chance of revascularization failure. The early diagnosis of ALI is crucial to maximize limb salvageability and decrease its associated morbidity and mortality. During VA-ECMO, vascular complications are common, heterogeneous, and significantly affect the outcome. 2 ALI incidence varies from 8.6%–33% in the literature. Multiple risk factors for developing vascular complications have been previously described; however, the mechanism and pathogenesis are still unclear. The ipsilateral peripheral arterial insufficiency, as well as the increased intra-compartmental pressure, is a significant proposed explanation. 17 The incidence of acute vascular complications in Tanaka et al was 20%, including a 12% incidence of acute limb ischemia with DPC that developed the compartmental syndrome, and fasciotomy was done. 10
In this study, the overall incidence of ALI was 7.7%. The incidence of ALI in COVID-19 patients was higher but not significant (P = 0.517 and P = 0.323 for acute lower and upper limb ischemia, respectively). Interestingly, ALI occurred in the upper limb of 1 COVID-19 patient despite the absence of any attached cannulas. This can be explained by the cytokines storm theory associated with the COVID-19 infection.
The physical compression effect was evident in 2 non-COVID patients due to the associated venous hypertension caused by the venous cannula. In this patient, the clinical presentation was classical for compartmental syndrome vs extensive deep venous thrombosis, which was excluded by the venous duplex. He necessitated decannulation and fasciotomy with adjustment of anticoagulation to avoid bleeding complications.
Vascular injuries that may occur during the insertion or removal of arterial or venous cannulas are bleeding, dissection, or developing a pseudo aneurysm. The incidence of these complications in most of the literature is 7%-14%, which happens according to different patients’ demographic data, risk factors, and cannulation techniques of VA-ECMO, including distal perfusion cannulas.18-23 In our study, percutaneous cannulation failed in 2 patients in each group who required surgical exploration. The overall incidence of arterial dissection was 5.1%. (P = 0.970) These complications were attributed to morbid obesity, the associated hypotension with arterial spasm in these patients.
This study’s overall incidence of profuse cannula-related bleeding was 5.1% (P = 0.970). In 1 patient, the profuse bleeding was attributed to leaking from the site of arterial cannulation.
In our study, the overall incidence of groin infection was 12.8% (P = 0.676). According to the local hospital protocol, multiple organisms were isolated from the cannula sites despite being inserted under a complete aseptic technique under antibiotics coverage. In literature, the infection rate of the groin cannulas has been reported from 1.1%-24%.24-27 Multiple risk factors have been postulated, including the original indication for VA-ECMO insertion, prolonged intubation, prolonged ICU stay, malnutrition status, and obesity. The groin infection may worsen the bad general condition with subsequent bacteremia and septicemia. The medical community’s reaction to the SARS-CoV-2 pandemic can be characterized as resourceful, adaptable, and resilient. Although COVID-19’s intricacies are still evolving, and many questions about its pathophysiology remain unanswered, it is evident that older patients, those with underlying cardiovascular disease, and those with secondary infections are at a higher risk of mortality. While VV ECMO has been consistently employed to treat respiratory failure, its success rate varies. VA ECMO’s efficacy in refractory cardiogenic shock remains a question. The authors suggest that the decision to use VA ECMO for COVID-19 should be based on the same standards applied by specialized centers for patients with cardiogenic shock. VA ECMO is a complicated procedure requiring experienced personnel, and it should always be conducted with a multidisciplinary approach, considering individual patient factors. Given the current understanding of COVID-19’s impact on the cardiovascular system, otherwise, appropriate candidates experiencing refractory cardiogenic shock should be considered for VA ECMO to give them a fair chance of full recovery.28-31
Limitations of the Study
The main limitation of this study is its design as a retrospective single-center study. However, to our knowledge, it does not impact its findings. It is the first study to report the different vascular complications associated with VA-ECMO and compare them in COVID and non-COVID patients. The second limitation was the relatively small sample size, particularly considering the rarity of VA-ECMO use and the specific subgroup of COVID-19 patients. A multi-center study with a larger sample size could provide more statistical power and allow for a more robust analysis of differences between COVID-19 and non-COVID patients in terms of vascular complications associated with VA-ECMO. Moreover, the study primarily focuses on acute vascular complications associated with VA-ECMO, but it may overlook other important factors such as long-term outcomes, quality-of-life measures, or specific management strategies employed for these complications. A more comprehensive analysis that includes a broader range of clinical endpoints would provide a more holistic understanding of the implications of VA-ECMO in both COVID-19 and non-COVID patients.
Conclusion
During the era of the COVID-19 pandemic, more patients are kept on VA-ECMO for the associated respiratory failure. Patients on VA-ECMO are at high risk of developing different vascular complications. COVID-19 increases the risk of acute ischemia in both upper and lower limbs and thrombosis of distal perfusion catheters. However, other vascular VA-ECMO-related complications are comparable between COVID and non-COVID patients.
Footnotes
Authors’ Contributions
Conception and design: Mohammed Alsagheer Alhewy. Alhussein M. khedr, Abdelhalim A. Abdelmohsen, Mohammed S. Foula. Collection: Hassan Gado, Wael Abdo Abdo Abd-Elgawad, Ahmed Atef Khamis, Abdelaziz Ahmed Abdelhafez, Ibrahim Hanbal hanbal, Ehab Abd elmoneim Ghazala. Writing the article: Mohammed Alsagheer Alhewy, Alhussein M. khedr Critical revision of the article: Alhussein M. Khedr, Abdullah El Sayed, Awad Ibrahim, yasser Elghoneimy. Final approval of the article: Mohammed Alsagheer Alhewy, Alhussein M. Khedr. Statistical analysis: Ehab Abd elmoneim Ghazala.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.