
Abstract
Loeys Dietz Syndrome (LDS) is an autosomal dominant connective tissue disorder resulting from a mutation in the transforming growth factor beta receptor (TGFBR) family of genes. It is commonly associated with the development of aortic aneurysms and dissections. We report the successful open surgical management of thoracoabdominal aneurysms in a father and daughter with Loeys-Dietz Syndrome after failed endovascular repair. The daughter required stent graft explantation, while the stent graft remained in the father. These cases highlight the importance of early genetic testing of both patients and first-degree family members in those with a strong history of aortic disease, even when there is a lack of typical connective tissue disorder associated physical exam findings and open surgical index operations.
Introduction
Loeys-Dietz syndrome (LDS) is an autosomal dominant connective tissue disorder resulting from a mutation in the transforming growth factor beta receptor (TGFBR) family of genes. 1 It is classically associated with craniofacial, skeletal and aortic complications. Up to 33% of patients with LDS will also develop aortic aneurysms and up to 11% of LDS patients will develop aortic dissections. Though both open and endovascular approaches have been described for repair of thoracoabdominal aneurysms, endovascular approaches are associated with a higher rate of reintervention secondary to endoleak. 2 In this study, we report the open surgical management of a father and daughter with LDS with prior and failed endovascular repair secondary to endoleak.
Methods
Patient 1
A 36-year-old woman with LDS and a history of postpartum type A aortic dissection with ascending aortic replacement and hemiarch in 2012, chronic type B aortic dissection with left carotid to subclavian bypass and zone 2 thoracic endovascular aortic replacement (TEVAR) in 2016, and a composite valve graft aortic root replacement with a mechanical valve, total arch replacement, and stage I elephant trunk in 2021 all performed at an outside hospital presented with right-sided chest pain with radiation to the back and abdomen in 2022. At presentation, the patient was hemodynamically stable. Computed tomographic angiography (CTA) demonstrated type R endoleak, a 9 cm Crawford extent II TAAA (Figure 1), and bilateral tortuous internal carotid arteries.
3
A: Patient 1 CT scan, B: Patient 2 CT scan.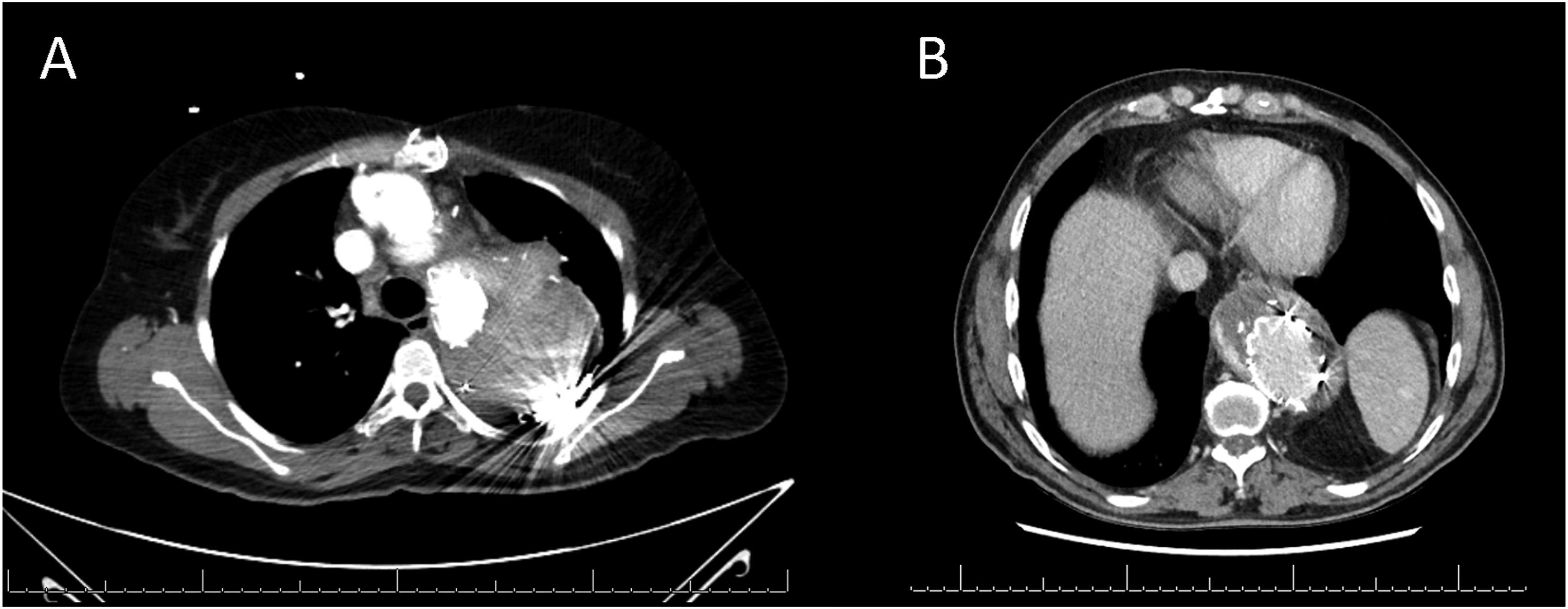
A decision was made to proceed with open repair due to the large size of the aneurysm and risk of rupture. The patient was placed in the right lateral decubitus position and a thoracoabdominal incision was made at the 5th intercostal space. The femoral artery and vein were cannulated and cardiopulmonary bypass (CPB) was initiated. Under deep hypothermic circulatory arrest (DHCA) (20°C), the aorta was transected and the stent was explanted. A 26-mm graft was anastomosed proximally to the previous elephant trunk graft with 4-0 polypropylene suture and retrograde perfusion was established for 3 minutes, followed by antegrade perfusion. The distal anastomosis was completed at the level of the infrarenal aorta and reinforced with teflon felt. The celiac, superior mesenteric, right, and left renal artery were reattached using a 12 × 10 × 10 trifurcated graft (Terumo, Somerset, USA).
The patient was extubated after 36 hours. After surgery, the patient developed renal failure requiring temporary dialysis. She was discharged home on postoperative day (POD) #16. At 1 year follow-up, CT scan revealed stable aorta.
Patient 2
A 62-year-old man with LDS, who incidentally was the father of Patient 1, presented with back pain in 2023. The patient had a history of prior bentall procedure with a mechanical valve with concurrent mechanical mitral valve replacement and CABG in 2007, followed by hybrid aortic arch repair with TEVAR in 2017 performed at an outside hospital. Of note, the patient endorsed a significant family history of sudden death of unknown cause of his father and multiple brothers. The CT scan demonstrated a tortuous aorta with type 1B endoleak and a 6.9 cm Crawford extent III TAAA (Figure 1), enlarged from 5.7 cm one year prior. The patient elected to proceed with open surgical repair due to the high risk of rupture and associated back pain.
The patient was placed in the right lateral decubitus position and a thoracoabdominal incision was made at the sixth intercostal space. After femoral-femoral cannulation, CPB was initiated. Under DHCA, the aorta was transected at the level of the distal stent, and a 30-mm graft was anastomosed proximally to both the stent graft and the full thickness of the aortic wall. The anastomosis was reinforced with pledgeted sutures. The distal anastomosis was completed at the level of the aortoiliac bifurcation. The celiac, superior mesenteric, and left renal vessels were selectively perfused and then reattached directly to the aortic graft using 8 mm interposition grafts. An additional 8 mm graft was anastomosed to the right iliac artery to perfuse the right renal artery.
Postoperatively, the patient required a sigmoid colon resection for bowel ischemia. He also developed cholecystitis requiring a percutaneous cholecystostomy drain, renal failure requiring temporary dialysis, and tracheostomy. He was discharged to a rehabilitation facility on POD #57. Written informed consent for publication was obtained for both patients.
Discussion
Given the propensity of patients with LDS to develop aneurysm and dissection leading to aortic rupture, the 2022 ACC/AHA guidelines recommends that LDS patients with aneurysms > 4.5 cm undergo aneurysm repair with an additional class I recommendation that open repair over endovascular repair be used for aneurysms of the thoracoabdominal aorta. 4 These cases once again reinforce the high reoperation rates associated with endovascular repair of thoracoabdominal aneurysms in patients with LDS and the need for open surgery as the index operation. Both patients developed endoleak requiring open repair. Patient 1 had type R endoleak resulting from septal fenestrations near the distal stent, which was pressurizing the false lumen, and because of the presence of a prior elephant trunk, the TEVAR was explanted. We chose not to explant the TEVAR for patient 2, instead sewing directly to the stent, because the stent was landed proximally in graft, decreasing the risk of proximal aortic expansion following thoracoabdominal repair. Successful explant and stent preservation have both been reported with mortality as low as 6% in cases without infection.5,6 In both patients, while endovascular repair was done prior to genetic screening, workup was incomplete prior to intervention as genetic screening was only pursued in 2019 after multiple aortic interventions and reinterventions for aneurysm and dissection. The decision-making behind the placement of TEVARs in both patients is ultimately unclear as they were both done at outside hospitals.
Diagnosis of LDS remains a challenge, with aortic manifestations, such as aneurysms, dissection, and tortuosity being the most common physical manifestation. Comparatively, less than 30% of patients present with the chest wall deformity, arachnodactyly, or skeletal abnormalities traditionally seen in connective tissue disorders. Neither of our patients had significant physical exam findings or the hypertelorism, blue sclera, or abnormal uvula more specific to LDS. 7 Despite the lack of physical exam findings, a strong family history was still present. Patient 1 had a peripartum dissection at 26, a complication seen in as high as 4% of patients with LDS, and patient 2 required replacement of an aneurysmal aortic root at 46, and multiple family members had sudden deaths in early adulthood for unknown reasons. Patients like these, with thoracic aortic disease under 60, family history of thoracic aortic disease, or clinical features of connective tissue disorder should undergo genetic screening. These measures may have decreased the number of interventions required for both patients and can guide the surveillance and treatment course of other family members.
Endovascular repair has been sparingly utilized in select LDS patients. Endovascular repair has been associated with an increased risk of stent graft explant, retrograde dissection, endoleak and access site complications.8,9 The radial forces from the endografts in native, fragile aortas results in subsequent dilation, which explains the high reintervention rates in LDS patients.8,9 Consequently, an endovascular approach is most amenable in high-risk patients with multiple comorbidities or prior surgical grafts serving as both proximal and distal landing zones. For example, patients with prior TEVARs and/or frozen elephant trunks may be acceptable candidates for TAAA hybrid repair with the endografts landed in prior surgical grafts, which avoids the risk for retrograde dissection and ensures adequate graft apposition and seal.8,9 Endovascular repair in LDS patients should be only undertaken in select patients after a thorough multidisciplinary discussion as open surgical repair is the gold standard.
Conclusion
Ultimately, these cases are a personification of the saying, like father like daughter, where unfortunately both patients had similar symptoms, presentation, and ultimately treatment course. They highlight the importance of open surgical repair as the index operation in patients with LDS and early genetic testing of both patients and first degree family members in those with a strong history of aortic disease, even when there is a lack of typical connective tissue disorder associated physical exam findings.
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Babak Abai: consultant for Endologix and Cook Medical. All other authors have no conflicts of interest to declare.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.