
Abstract
Background
Radiofrequency ablation (RFA) is a minimally invasive treatment for lower limb varicose veins. Studies indicate that RFA results in immediate occlusion of 90%–100% of treated long saphenous veins. Evidence suggests that post-operative scans rarely alter patient management or outcomes.
Objective
The aim of this study was to assess the potential necessity of routine postoperative scanning in the treatment of varicose veins.
Method
Retrospective data were collected for the patients who had RFA under a single consultant from November 2015 to June 2018. Descriptive statistics were calculated to summarize patient demographics, procedural details, and outcome measures.
Results
A total of 124 patients underwent radiofrequency ablation (RFA). Most of the patients (n = 114, 92%) demonstrated complete ablation, indicating a high success rate for the procedure.
Conclusion
This study suggested that routine postoperative scanning should be discontinued as this did not alter patient management in over 99% of cases. The resources currently used for postoperative scans could be redirected towards other critical areas.
Introduction
Symptomatic venous insufficiency is a prevalent condition, affecting 1%–15% of adult men and 20%–25% of adult women, with saphenous vein insufficiency being the most common form. Symptoms include pain, edema, fatigue, varicose veins, and venous ulcers. The National Institute for Health and Care Excellence (NICE) published Quality Standard QS67 to enhance the quality of life for people with varicose veins, aiming to prevent progression to varicose eczema, phlebitis, and leg ulcers, and to reduce recurrence risks. NICE’s quality statements mandate that individuals with symptomatic or complicated varicose veins be referred to a vascular service, assessed with duplex ultrasound, and, if truncal reflux is confirmed, treated with endothermal ablation, ultrasound-guided foam sclerotherapy, surgery, or compression hosiery in that order. 1
Radiofrequency ablation (RFA) is a minimally invasive treatment involving the heating of the vein wall using a bipolar generator and catheter with sheathable electrodes. The saphenous vein is accessed via an intravenous cannula or small incision, and the catheter is withdrawn at a controlled rate, maintaining the vein wall temperature at 85°C. Studies indicate that RFA results in immediate occlusion of 90%–100% of treated long saphenous veins. 2 Despite the safety and effectiveness of RFA, it carries well-known risks of side effects, recanalization, and can pose a significant problem for patients’ health outcomes. In these patients, recanalization may be the result of the device settings (eg, number of RF cycles, energy delivered), and/or physician experience. 3 Other factors may also play a role, such as clinical and duplex ultrasound (DUS) findings and patient characteristics. 4
Patients undergoing RFA report less pain and reduced analgesia requirements compared to those who undergo traditional vein stripping surgery. 5 Current evidence supports the safety and efficacy of RFA as an alternative to saphenofemoral ligation and stripping, provided proper consent, audit, and clinical governance are maintained. However, significant resources are currently allocated to post-operative scanning to verify procedural success, which may be unnecessary. Evidence suggests that post-operative scans rarely alter patient management or outcomes, indicating potential for resource reallocation if these scans can be demonstrated as non-essential.
Methods
This study utilized a retrospective data collection method, reviewing outpatient letters and operation notes to gather relevant information. The success of the radiofrequency ablation procedure was assessed through postoperative scans available on the hospital’s online database. The inclusion criteria used were that the patient should have been diagnosed with the chronic venous insufficiency (CVI) and treated by a single consultant from November 2015 to June 2018. The exclusion criteria entailed patients diagnosed with any other condition other than CVI, those diagnosed with CVI in the perforator veins, and those diagnosed outside January 2012 to December 2018. Also excluded were CVI diagnoses that were not treated using RFA. The steps to perform venous ablation using RFA were similar as treated by single consultant. Patients underwent postoperative DUS at 4 weeks postoperatively as per the hospital policy. Procedural success was considered as the lack of colour flow during the DUS. Recanalization was defined by the presence of reflux in the targeted vessel during the scan. Reflux in the tributaries or perforator veins were not considered as recanalization after the procedure.
Demographic data and the completeness of ablation, as evidenced by a postoperative scan conducted at 4 weeks, were collected. This methodology facilitated the evaluation of procedural success and the potential necessity of routine postoperative scanning in the treatment of varicose veins. The data were organized and managed using Excel for preliminary analysis and subsequently imported into statistical software for detailed analysis.
Descriptive statistics were calculated to summarize patient demographics, procedural details, and outcome measures. In this retrospective cohort study descriptive data sets were presented in the form of mean and proportion. A series of univariate analysis was performed using different data sets. Then multivariate analysis was performed using these results. The ultimate goal was to enhance clinical decision-making processes and improve patient care with appropriate resource utilization.
This retrospective study was conducted in accordance with ethical standards and institutional review board guidelines and was registered and approved by appropriate hospital body (Clinical audit department). This is an observational retrospective study of already entered data in the hospital data base. There was no direct contact with the patient during this study. The data were made anonymised with no identifier and as per the Declaration of Helsinki; research using anonymized does not create an obligation to obtain informed consent. Patient confidentiality was maintained, and all data were anonymized prior to analysis.
Results
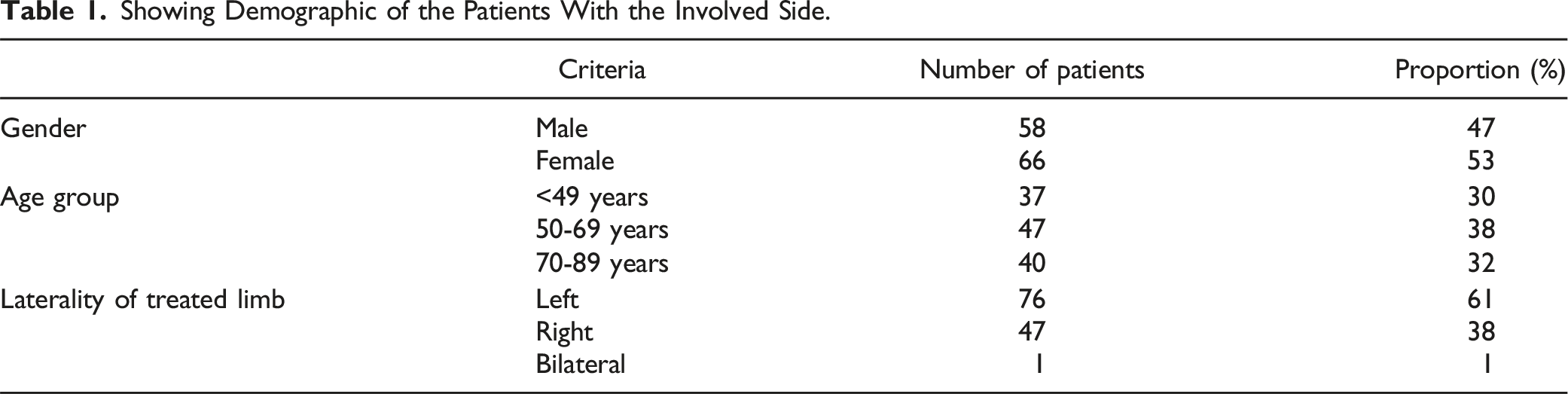
Showing Demographic of the Patients With the Involved Side.
Indications for radiofrequency ablation (RFA) in this cohort were diverse, with the majority being related to skin changes. Specifically, 72% of the patients underwent RFA due to skin changes such as varicose eczema and lipodermatosclerosis. Thrombophlebitis accounted for 13% of the indications, followed by venous ulcers at 10% (Figure 1). Bleeding was a less common indication, representing 2% of cases, while another 2% of cases had unspecified indications (N/A). These statistics highlight the predominant role of skin-related complications in prompting the use of RFA for treating varicose veins. Pie chart showing the indications of the procedure.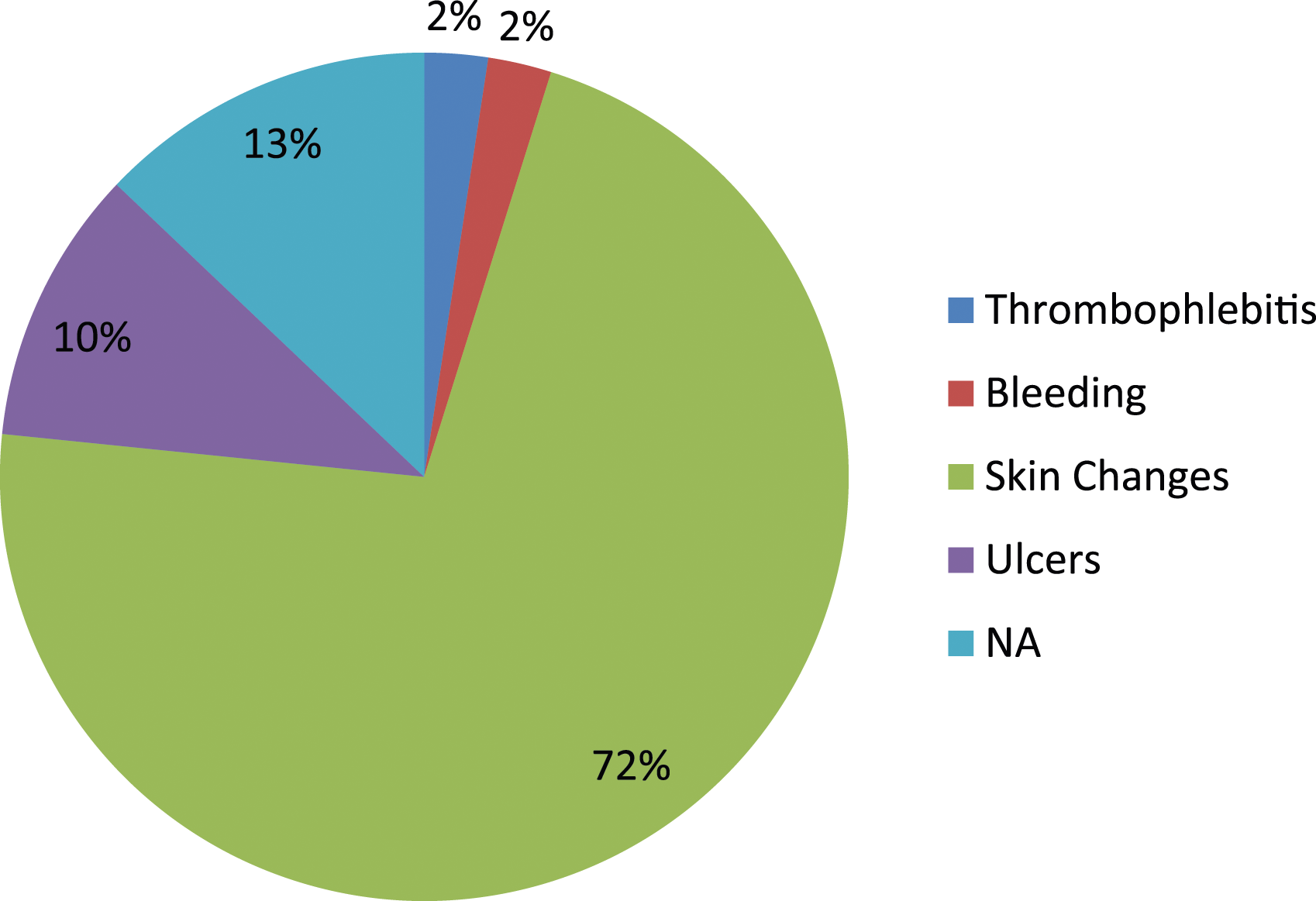
The success of radiofrequency ablation (RFA) in treating varicose veins was notable in this study. Out of 119 patients who underwent postoperative scanning at 4 weeks, 114 cases (92%) demonstrated complete ablation, indicating a high success rate for the procedure (Figure 2). In 4 cases (3%), partial ablation was observed; despite this, 3 of these patients experienced symptomatic relief and required no further intervention, underscoring the clinical benefit even in partial ablation scenarios. Only 1 case (0.8%) was identified as a failed ablation (Figure 2). These results underscore the efficacy of RFA, with a significant majority achieving complete vein closure and symptomatic improvement even in cases of incomplete or failed ablation. Bar graph showing success of RFA.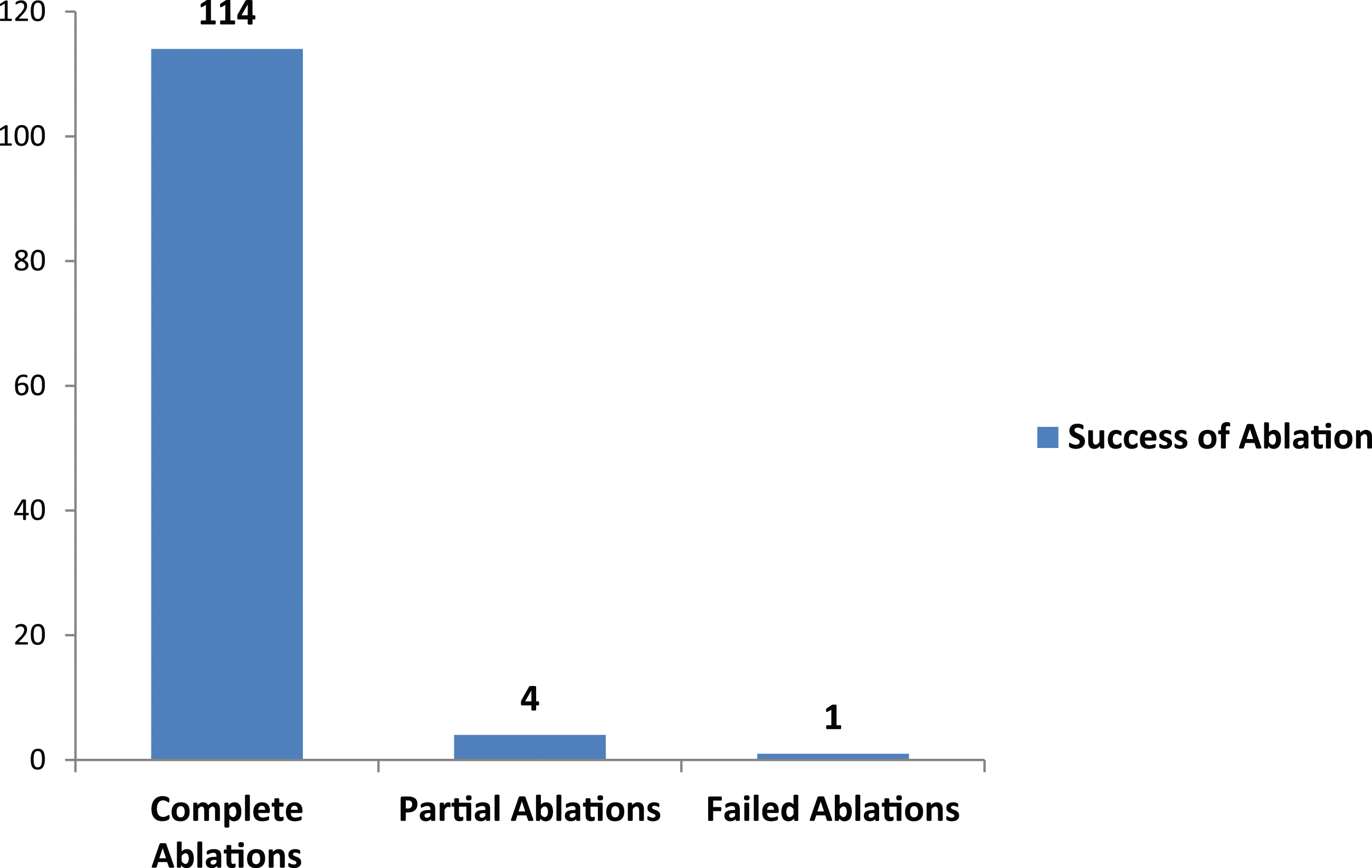
Discussion
Radiofrequency ablation (RFA) is a minimally invasive technique that serves as an effective alternative to conventional stripping surgery for treating varicose veins. Our experience with the RFA procedure has shown fewer perioperative complications compared to traditional methods. While numerous studies on RFA have been conducted in Europe and the United States, there is a scarcity of research focusing on the mid-term results of this approach in other regions. Our study observed excellent mid-term clinical outcomes, indicating that RFA is a safe and effective procedure for varicose vein treatment.
The treatment of varicose veins with radiofrequency ablation (RFA) in this study met the standards set by NICE Interventional Procedure Guidance and demonstrated high success rates consistent with published data. With 92% of patients achieving complete ablation and symptomatic relief observed in nearly all cases of partial or failed ablations, RFA proves to be a highly effective treatment modality. Importantly, this study found that postoperative imaging did not alter patient management in over 99% of cases. This suggests that routine postoperative scanning, which involves significant resource allocation, may not be necessary for the majority of patients.
In this study, only 4 patients showed evidence of partial ablation on follow-up, and 1 case was noted as a failed ablation. This procedure led to successful vein occlusion in 92% of patients. Although studies specifically addressing recanalization rates in RFA are limited, our findings align with the study involving postoperative scanning after RFA, who noted an occlusion rate of 99% during their follow-up period. 6 In another observational study, a 3.7% rate of recanalization or incomplete occlusion with RFA was observed. 7 These findings were comparable to the findings of this study.
Minor complications associated with RFA include muscle cramping, localized hot flashes, induration, numbness, skin discoloration, and persistent pain. Our study observed similar complications, and at the end of the follow-up period, the Venous Clinical Severity Score (VCSS) had significantly improved without the need for antithrombotic therapy. Importantly, no major complications, such as nerve injury, were noted.
Given the findings from this study, it is recommended that routine postoperative scanning be discontinued, and the resources currently used for these scans be redirected towards other critical areas in the health care system. This reallocation could enhance overall patient care by focusing resources where they are more urgently needed. However, it is also recommended that postoperative scanning be retained for selected patients. These patients might include those with atypical clinical presentations, those who do not experience expected symptomatic relief, or those with other complicating factors that warrant closer monitoring.By adopting a more selective approach to postoperative imaging, health care providers can ensure that high standards of patient care are maintained while optimizing the use of available resources. This strategy not only aligns with evidence-based practices but also promotes more efficient and effective patient management. Overall, the findings of this study support the continued use of RFA as a primary treatment for varicose veins and advocate for a more judicious use of postoperative imaging, enhancing both patient outcomes and health care resource management.
Limitations
Despite the promising results, our study had several limitations. Limitations of the study included those associated with small sample size and a single-centre retrospective analysis, performed by 1 surgeon following a standardized preoperative, intraoperative, and postoperative protocol. Selection bias may have been present, because patients chosen for the procedures were treated at the discretion of the surgeon. Further studies are needed to address the outcome of the asymptomatic patients in the long term.
We did not have the Venous Clinical Severity Scores retrospectively. Further, this dataset did not include patient-reported outcomes. Given that we did not perform weekly DUS examination and given our patient population, we may not have the granularity to identify most accurately when the recanalization first occurred. This factor may change the timeline from when the recanalization first occurred to when it resolved, slightly.
Further prospective studies with larger cohorts are needed to validate these findings and potentially refine the clinical guidelines for the use of RFA in varicose vein treatment.
Conclusion
Finally, this study showed that postoperative imaging after radiofrequency ablation (RFA) of varicose veins did not alter patient management in over 99% of cases. This suggests that routine postoperative scanning, which involves significant resource allocation, may not be necessary for the majority of patients. Given these findings, it is recommended that routine postoperative scanning be discontinued, and the resources currently used for these scans be redirected towards other critical areas in the health care system. This reallocation could enhance overall patient care by focusing resources where they are more urgently needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This retrospective study was carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki) and is in line with the Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work in Medical Journals. This study was approved by the clinical audit team of the hospital (registration number- P0100) and all data were anonymised in view of data protection.