
Abstract
Bow Hunter syndrome (BHS) is a rare disorder characterized by mechanical occlusion of the vertebral artery (VA) during neck rotation, resulting in symptomatic, transient, and positional vertebrobasilar insufficiency. We describe a case of a 76-year-old female who presented with dizziness and right ear tinnitus triggered by right head rotation. Her symptoms would immediately resolve upon returning her head to the neutral position. CT angiogram showed 80% stenosis of the left subclavian artery origin, 50%–70% stenosis of the proximal right internal carotid artery (ICA), and near occlusive stenoses of the origins of the bilateral VAs. After failing conservative management, the patient was treated with left subclavian artery stenting, followed by a right carotid endarterectomy (CEA) 6 weeks later. Follow-up at 1 month showed resolution of paroxysmal symptoms and no neurological sequelae. To our knowledge, there have not yet been reported cases of patients with concurrent BHS, subclavian artery stenosis, and carotid artery stenosis. We suggest that global revascularization via subclavian artery stenting and CEA may be considered as treatment for patients with BHS complicated by other cerebrovascular disease secondary to stenoses of the ICA and subclavian artery. This approach obviates the need for more complex surgery or endovascular intervention of the VA.
Introduction
Bow Hunter syndrome (BHS) is a rare disorder characterized by mechanical occlusion of the vertebral artery (VA) during neck rotation, resulting in symptomatic vertebrobasilar insufficiency.1-4 Symptoms of this syndrome can include dizziness, syncope, tinnitus, diplopia, and focal neurological deficits when the head is turned, though symptoms are generally transient and reversible when the head is returned to its neutral position.4,5 Though there is no standard clinical treatment for BHS, a variety of treatments have been proposed in the literature, including surgical decompression of the VA, C1-C2 fusion, and endovascular interventions such as angioplasty or stenting of the VA.3,6-8 Despite the slowly growing body of literature on BHS cases and potential treatments, there are limited cases involving confounding factors such as concurrent stenoses, and limited reported cases in geriatric women at their eighth decade of life.9,10 The literature on concurrent stenosis in BHS is limited to cases in which stenosis of the internal carotid artery (ICA) or subclavian artery is present, but not together.11-13 Here we present a case of BHS complicated by cerebrovascular disease secondary to stenoses of the ICA and subclavian artery in a 76-year-old woman.
Case Report
A 76-year-old female presented to the vascular surgery clinic with several months of dizziness and right ear tinnitus triggered by right head rotation. Her symptoms would immediately resolve upon returning her head to the neutral position. These episodes were not associated with any other symptoms, including vision changes, numbness, weakness, paralysis, drooping face, slurred speech, or amaurosis. CT angiogram showed 80% stenosis of the left subclavian artery origin, 50%–70% stenosis of the proximal right ICA, near occlusive stenoses of the origins of the bilateral VAs, and mild focal stenosis of the V4 segment of the distal left VA. However, upon further review, the proximal left VA appeared tortuous, but not necessarily stenotic. Though the left VA is more commonly implicated in BHS, 14 dynamic imaging was not obtained for the patient, and it is unknown which of the 2 VAs, or both, is responsible for the patient’s symptoms. However, based on the patient’s symptoms and CT angiogram results, it was hypothesized that the patient’s cerebrovascular disease and atherosclerotic burden predisposed her to a Bow Hunter phenomenon and was largely contributory to her symptoms; the Bow Hunter phenomenon described here may possibly be considered as multifactorial.
Following diagnosis, the patient started conservative management, consisting of dual antiplatelet (ASA and clopidogrel) and statin therapy with instructions to avoid triggers. The patient did well with this approach until 13 months later when she presented again with severe dizziness and vomiting. A repeat CT angiogram at this time showed severe stenosis of the origin of the left subclavian artery, severe focal stenosis of the proximal right vertebral artery, severe stenosis of the proximal right ICA secondary to calcified plaque, mild stenosis of the proximal left ICA, and mild focal stenosis of the V4 segment of the distal left vertebral artery (Figure 1). CT angiogram in 2022. White arrows indicate locations of left subclavian artery stenosis (bottom left arrow), right vertebral artery stenoses (bottom right arrow), and right internal carotid artery stenosis (top right arrow). The gray arrow indicates tortuosity of the left vertebral artery, which was initially read as stenosis during an earlier CT angiogram.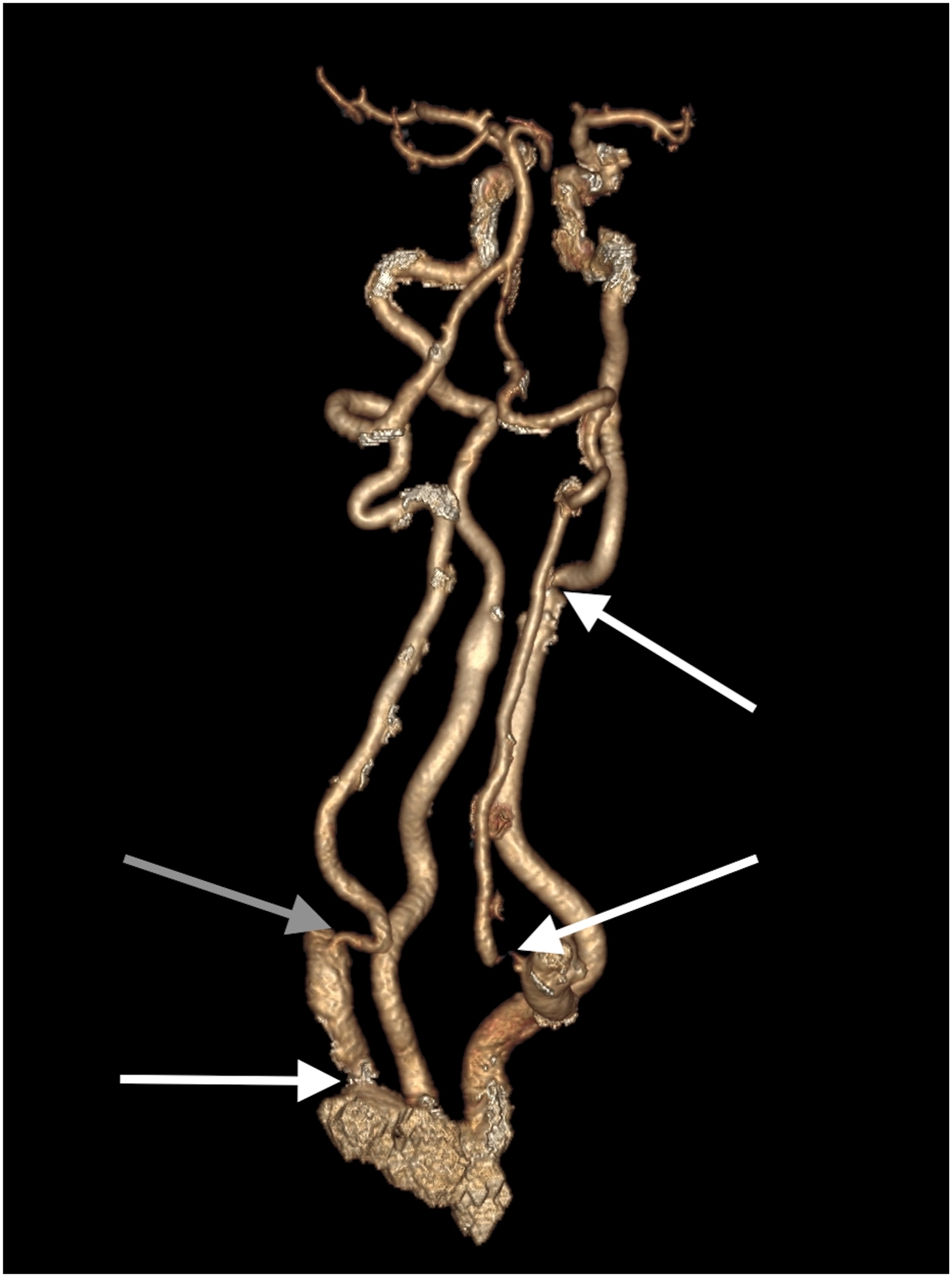
Given her recurrent symptoms and severe subclavian stenosis, she underwent a left subclavian artery stenting to reperfuse the left VA in addition to continuing her dual antiplatelet and statin medications. On the day of surgery, left brachial artery access was obtained, and an angiogram was shot to identify the lesion. An 8 mm × 29 mm VBX balloon-expandable covered stent (W. L. Gore & Associates, Newark, DE) was positioned across the lesion at the proximal left subclavian artery extending just into the aorta proximally and landing just short of the left vertebral artery takeoff distally. The stent was deployed with a great result, showing no significant residual stenosis of the subclavian artery on completion angiogram. There were no periprocedural complications, and the patient tolerated the procedure very well. However, despite successful and uncomplicated stenting of her left subclavian artery, her symptoms persisted at a 1-month post-operative follow-up.
Given that the left subclavian artery stenting restored posterior circular flow, but the patient’s symptoms persisted, we believed that the next step would be to restore anterior circulation and improve overall brain perfusion. At this time, we decided to proceed with a right carotid endarterectomy (CEA). Six weeks after her subclavian stenting, the patient was brought back to the operating room. Intraoperatively, significant stenosis of the carotid bulb and proximal internal carotid artery was observed, and standard CEA with bovine pericardium patch angioplasty was performed. Continuous forward flow in the internal carotid artery was confirmed with Doppler. Her surgery and post-operative course were uncomplicated, and follow-up at 1 month showed resolution of paroxysmal symptoms and no neurological sequelae. Postoperative duplex showed resolution of the stenosis of the right ICA. She has had no return of her BHS symptoms at 1-year follow-up.
Discussion
This report documents the use of global revascularization via subclavian artery stenting and CEA for the treatment of Bow Hunter Syndrome (BHS) complicated by cerebrovascular disease secondary to stenoses of the right ICA and left subclavian artery. This is the first documented case report of BHS with concurrent subclavian artery stenosis and carotid artery stenosis that has been successfully treated.
According to the current literature, BHS is normally caused by the obstruction or compression of the VA during neck rotation. 4 The most common causes are herniated disk, osteophyte formation, and tumors.1,2 Stenosis of the vertebral artery is worsened by head rotation which results in downstream hypoperfusion of brain tissue, alongside other complications. 5 VA stenosis most commonly occurs near the C1-C2 level of the transverse foramina, where the VA enters at the C6 level, travels cranially, and exits at the C1 level. 15 Common symptoms of BHS such as dizziness and syncope tend to be worse in patients with bilateral VA stenoses where neither artery can sufficiently provide adequate perfusion to the brain. 15 Though BHS symptoms most commonly present between the fifth and 7th decades of life and with high male predominance,9,10 there have been recorded atypical cases such as ours, involving female patients nearing their 8th decade of life. 15
Due to the rarity of BHS, there are no clinical guidelines for its diagnosis and no standard treatment. 2 BHS can be diagnosed by a variety of methods, such as a vascular ultrasound, computed tomography angiography, or magnetic resonance angiography.2,16 In the literature, both conservative management and procedural treatment have been performed for symptom management. Conservative treatments include those that restrict the rotation of the head and neck, such as a neck brace or antiplatelet/anticoagulation therapies. 2 Several studies and case reports3,17 have suggested that conservative therapies alone can be effective for some patients.
When conservative management fails, BHS is classically treated with surgical decompression of the VA, C1-C2 fusion, or endovascular interventions such as angioplasty or stenting of the VA. VA decompression through partial transversectomy as treatment for BHS involves the removal of portions of the vertebral arch at the transverse foramen. Vertebral arch removal helps prevent compression by osteophytes and fibrous bands, without limiting the patient’s range of motion. 8 Another popular surgical treatment, C1-C2 fusion, involves insertion of a bone graft between the posterior arch of the atlas and the lamina of the axis to prevent VA compression, but permanently restricts neck movements. 18 Fusion is known to be amongst the most successful procedures in relieving symptoms; however, it is associated with 50%–70% restriction of head movement.3,6,7 Regardless of treatment choice between decompression, fusion, or a combination of the 2, Jost and Dailey found that procedural treatment resolved symptoms in 87% of patients, with decompression and fusion treated patients having no recurrence of symptoms. 6
Endovascular techniques such as VA stenting have also been used to treat both vertebrobasilar insufficiency19,20 and BHS,13,21 where self-expanding stents increase compression resistance and improve the ability of the VA to return to its original shape post-compression. Darkhabani and colleagues report 4 patients with BHS confirmed by dynamic digital subtraction angiography who were successfully treated with stent placement in the V2 segment (C2-C6) of the affected VA. 21 All patients reported symptomatic relief at 6 month clinical follow-up, and follow-up dynamic imaging demonstrated minor or no residual stenosis. Similarly, Sugiu and colleagues report a case of a patient BHS due to occlusion of the right VA during neck rotation and concurrent contralateral stenosis of the left VA at its origin. 13 The patient was successfully treated with a left VA angioplasty and stent placement with symptom resolution and good patency of the stented left VA at 6 month follow-up, demonstrating that VA stenting may be an effective treatment option in a patient with BHS with contralateral VA stenosis. Despite these case reports, however, there is a general paucity of long-term data on VA stenting for the treatment of BHS specifically, which is an area that warrants further research.
Though our patient presented with near occlusive stenoses at the proximal right vertebral artery, her case of BHS was further complicated by stenoses of the right ICA and left subclavian artery. Because of her global cerebrovascular disease, we pursued subclavian artery stenting and CEA to resolve symptoms via improved global reperfusion. Following both interventions, our patient reported resolution of her BHS symptoms without any post-operative complications. A prior case has been presented in which neck rotation limited perfusion through the left ICA, but not VAs, resulting in transient loss of consciousness; the insertion of a self-expanding stent, followed by carotid injection, successfully treated the patients’ symptoms. 11 Another report describes a patient with bilateral vertebral artery stenoses, thoracic aortic aneurysm, and severe stenosis of the left subclavian artery who presented with head-turning-induced syncope that was successfully treated with total aortic arch replacement and subclavian artery reconstruction alone. 12 These literature suggest that BHS symptoms may not always be due to impaired posterior circulation, as was traditionally thought. Our patient’s symptoms persisted despite partial restoration of the posterior circulation via left subclavian artery stenting, implying that the underlying etiology of her BHS symptoms was multifactorial and may be attributed, in part, to her high atherosclerotic burden. Because of this, we believed that the most appropriate next step would be a CEA of the right carotid artery, which would have been indicated regardless to reduce stroke risk due to her severe stenosis. We therefore suggest that global revascularization and restoration of anterior circulation may be beneficial specifically for BHS patients with similar concurrent cerebrovascular disease. If our patient’s symptoms continued to persist after the CEA, right VA revascularization would have been the next step. Further studies and case reports are necessary to evaluate the general safety and efficacy of subclavian artery stenting and CEA for the treatment of BHS complicated by subclavian and internal carotid artery stenoses.
Conclusion
This case report discusses a unique presentation of a BHS phenomenon in a patient with bilateral vertebral artery, left subclavian artery, and right internal carotid artery stenosis that was treated with left subclavian artery stenting and right carotid endarterectomy. We suggest that global cerebrovascular revascularization, without direct intervention on the VAs, may be considered as a viable treatment for patients with BHS complicated by other cerebrovascular disease. This approach obviates the need for more complex surgery or endovascular intervention of the VA. Subclavian artery stenting and CEA would also avoid the restriction in neck range of motion and risk of VA restenosis that have been reported for C1-C2 fusion and VA decompression, respectively.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, or publication of this article.