
Abstract
Background
To evaluate the feasibility, success rate, and safety of endovascular revascularization of patients with vertebral artery stump syndrome (VASS).
Methods
This single-center retrospective study analyzed clinical and imaging data from consecutive patients with VASS who underwent endovascular recanalization from January 2020 until June 2023.
Results
Our study enrolled 30 patients [mean age 69 (range 51-84) years; 26 men]. The rate of successful technical revascularization was 96.7% (n = 29), and the rate of complications was 3.3% (n = 1). At the 6-month follow-up, the patients with successful endovascular revascularization of VASS did not have any neurological symptoms, and computed tomography angiography showed 3/29 (10.3%) re-occlusions and 4/29 (13.8%) restenosis of the stent, which was confirmed by digital subtraction angiography.
Conclusions
Endovascular recanalization in patients with VASS is feasible in selected patients and has a high procedural success rate and low rate of complications. A large, multicenter, randomized study is warranted to confirm these findings.
Introduction
Vertebral artery stump syndrome (VASS) accounts for 1.4% of acute posterior circulation stroke and has a high stroke recurrence rate (25%) and poor prognosis. 1 VASS is a pathophysiology in which embolic strokes develop in the posterior circulation due to stagnating clot fragments through collateral artery flow after vertebral artery (VA) occlusion. 2 Treatment options for VASS include antiplatelet agents, 3 anticoagulants,1,4 surgical bypass,2,5 and endovascular therapy,6,7 although the optimal treatment for these patients remains controversial. With the development of endovascular interventions, a few case reports have evaluated the feasibility of endovascular recanalization in VASS as a valuable alternative for patients with recurrent stroke or transient ischemic attacks (TIAs) despite optimal medical therapy. However, most of those reports involve single cases, with case series being rare. Therefore, we evaluated the technical feasibility and safety of endovascular recanalization in VASS patients refractory to medical treatment. We retrospectively analyzed 30 VASS patients who underwent endovascular recanalization and proposed a new endovascular recanalization technique.
Patients and Methods
Patient Selection
Clinical Characteristics of Patients With VASS.
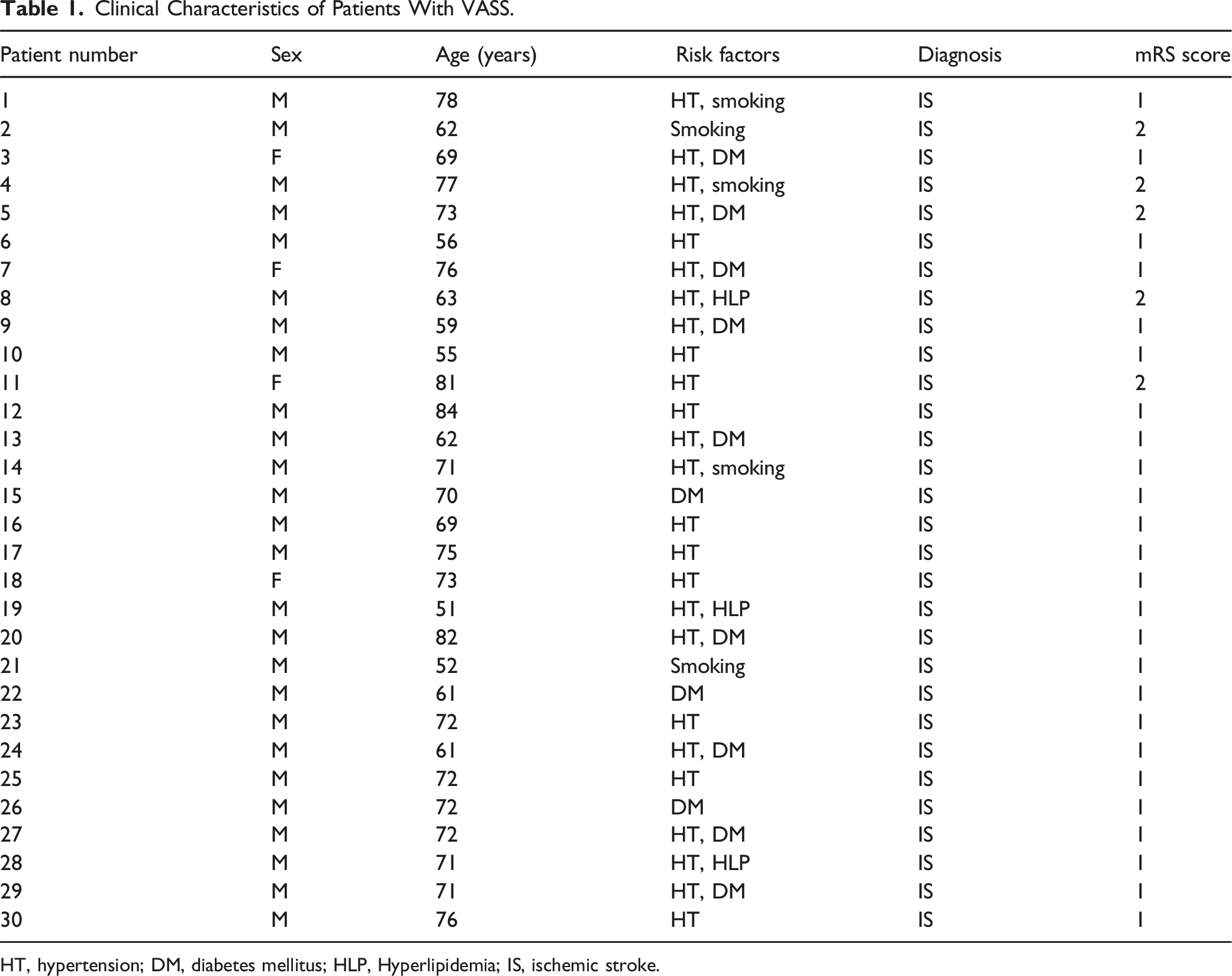
HT, hypertension; DM, diabetes mellitus; HLP, Hyperlipidemia; IS, ischemic stroke.
Patients who met the following criteria were included in this study: Non-acute occlusion of proximal extracranial vertebral artery which was confirmed by digital subtraction angiography (DSA); with or without a vertebral artery stump, antegrade flow were presented in the distal segment of V2 as reconstituted through the thyrocervical trunk branches or deep cervical artery which had adequate distal landing zone to place a distal embolic protection device; symptoms refractory to optimal medication, including dual antiplatelet therapy, lipid-lowering treatment and vascular risk factor modification; atherosclerotic lesions, absence of dissection, vasculitis or radiation angiopathy; and refusal to the bypass surgery. Patients with a history of intracranial hemorrhage, concomitant intracranial aneurysm or suffered a large infarction defined as a posterior circulation Alberta Stroke Program Early CT Score 8 of <6 points (based on magnetic resonance imaging diffusion-weighted imaging) were excluded. All patients provided informed consent before endovascular therapy. This study was approved by the clinical research ethics committee of our hospital.
Endovascular Procedure
After obtaining informed consent for surgery, endovascular therapy was performed under local anesthesia. All patients took aspirin 100 mg and clopidogrel 75 mg as antiplatelet medications for at least 5 days before undergoing the procedure. All patients were tested for CYP2C19 mutations, and if the results indicated clopidogrel resistance, we switched to ticagrelor (90 mg bid). The recanalization procedure was performed via the transfemoral route. After femoral artery puncture, intravenous heparin boluses were administered to maintain the activated clotting time between 250 and 300 seconds during the procedure. Cerebral DSA was performed to evaluate the vascular occlusion location and collateral status.
An 8.0-Fr guiding catheter or 6.0-Fr Shuttle sheath was placed in the left or right subclavian artery near the origin of vertebral artery. A 5.0-Fr diagnostic catheter (125 cm) was coaxially positioned into the ostial stump as an intermediate support catheter. To keep the system steady, a 0.018-in guidewire (V-18; Boston Scientific, Marlborough, MA, USA) was inserted between the sheath and diagnostic catheter as support into the ipsilateral brachial artery. A 0.014-inch microwire (PT-2, Boston Scientific, USA or Command, Abbott Vascular, USA) and microcatheter (Rebar-18, EV3, Irvine, CA, USA) were then carefully assembled coaxially. The microcatheter was then exchanged over a 0.014-inch microwire to navigate to and across the occlusion. A Sprinter Legend 2.0 × 20 mm balloon (Medtronic, Minneapolis, MN, USA) angioplasty was performed over the exchanged microwire to cross the occlusion. Distal embolic protection device (Spider FX; EV3, Irvine, CA, USA) was advanced over the exchange microwire and deployed distally at the V2 segment of the VA. If angiography showed a filling defect in the vertebral artery lumen, an distal access catheter was used for aspiration (Catalyst6, Stryker, Fremont, California, USA). The diameter and length of the occluded vertebral artery were measured after balloon angioplasty. The balloon-expandable stent was placed as a scaffold in the occlusion. Finally, the stent delivery catheter and protection device were retracted carefully. Postprocedural angiography was conducted to verify patency. A modified Thrombolysis in Cerebral Infarction score of 3 and ≤20% residual stenosis were regarded as successful revascularization.
The procedure was terminated if the microcatheter/microwire system could not pass through the occlusion segment after multiple attempts and the procedure time was more than 30 min. We switched to the retrograde recanalization method through the thyrocervical trunk or deep cervical artery in 2 of our cases after multiple failed attempts at anterograde recanalization (no.6 and 9). An 8.0-Fr guiding catheter or 6.0-Fr Shuttle sheath was positioned in the ipsilateral subclavian artery to the stump of vertebral artery. Then, a V-18 guidewire was passed into the ipsilateral brachial artery as a support to keep the system steady. The coaxial assembly of the microwire (Synchro-2 0.014 inches × 300 cm, Stryker, Cork, Ireland) and microcatheter (Excelsior SL-10, Stryker) was then advanced carefully through the thyrocervical trunk or deep cervical artery to the vertebral ostium and then the subclavian artery. Using the 0.014-inch wire as a marker, we switched to a PT-2 micro-guidewire (0.014 inches × 300 cm) for a more aggressive approach. Finally, we used the routine antegrade method of vertebral artery stenting (Figure 1). (A) The coaxial assembly of the microwire (Synchro-2 0.014 inches × 300 cm) and microcatheter (Excelsior SL-10) was advanced through the thyrocervical trunk or deep cervical artery to the vertebral ostium and then the subclavian artery. (B) Using the 0.014-inch wire as a marker, we switched to a PT-2 micro-guidewire (0.014 inches × 300 cm) and Rebar-18 microcatheter for anterograde recanalization. (C) After balloon dilatation distal embolic protection device (Spider FX) was deployed distal to the V2 segment of the vertebral artery. (D) The balloon-expandable stent was placed in the occlusion and then the stent delivery catheter and protection device were retracted.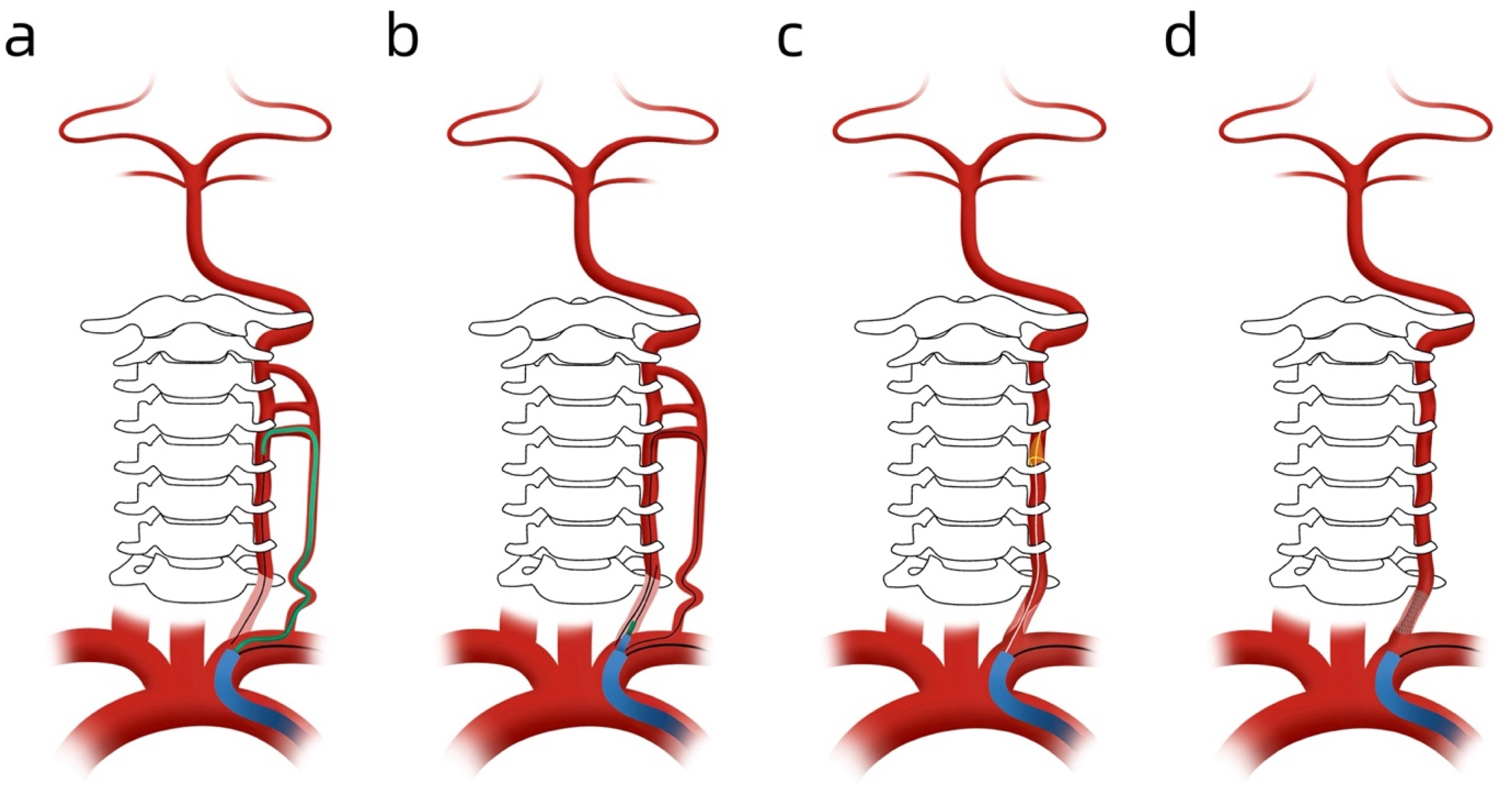
Illustrative Case of Retrograde Recanalization
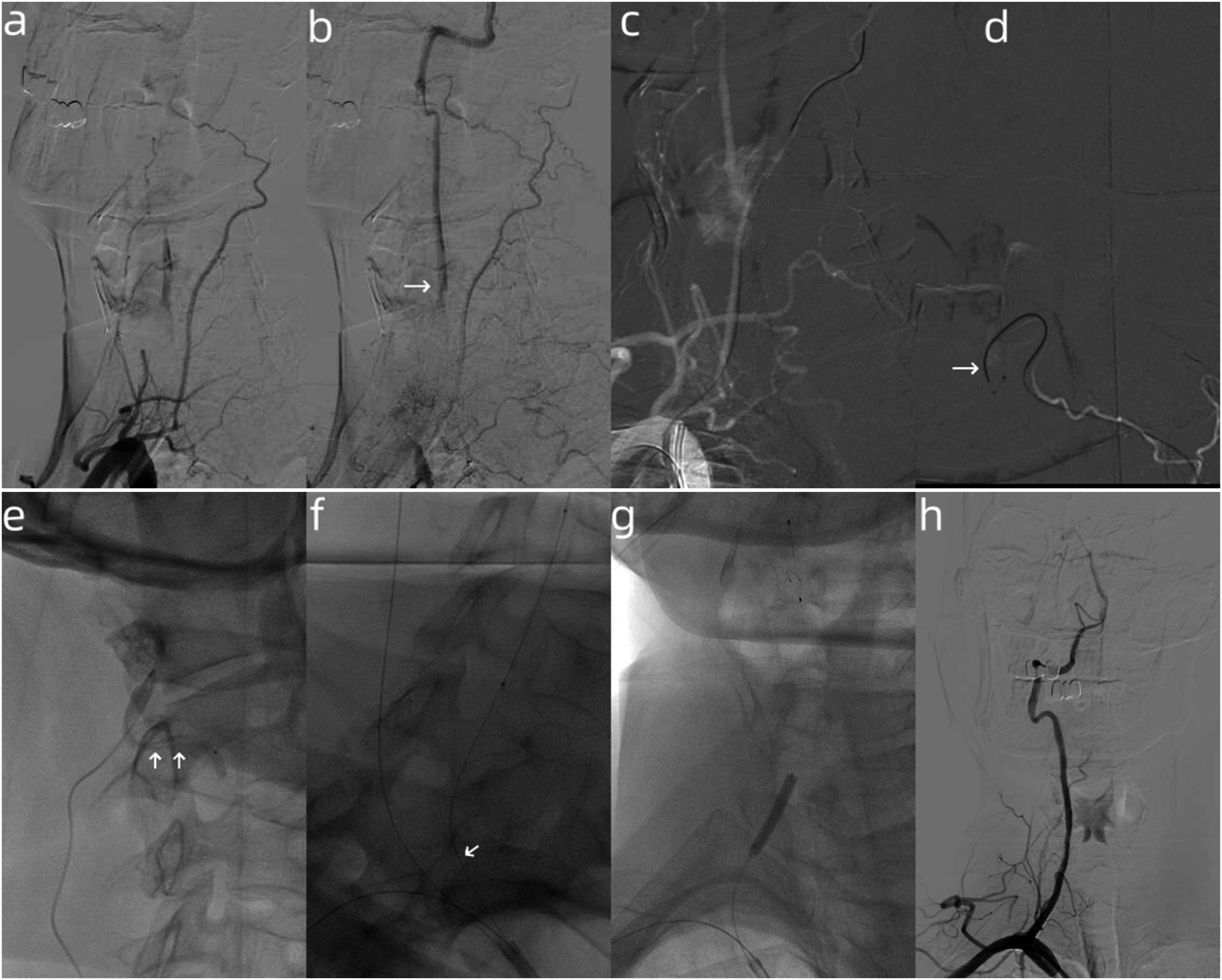
A 56-year-old man with a history of hypertension presented with dizziness. Brain magnetic resonance imaging showed a right cerebellar hemisphere infarction (Figure 2A). Neck CTA revealed occlusion of both vertebral arteries at their origins without obvious stumps, and the left vertebral artery seemed hypoplastic (Figure 2B). Computed tomography perfusion showed bilateral cerebellar hemisphere hypoperfusion, which was more severe on the right (Figure 2C). He was started on aspirin 100 mg daily, clopidogrel 75 mg daily, and rosuvastatin 10 mg at night. While in the hospital, he complained of repeated attacks of dizziness. Finally, endovascular revascularization of the right vertebral artery was performed successfully (Figure 3), and there have been no further events over 6 months of follow-up. (A) Fluid attenuated inversion recovery (FLAIR) imaging at admission showed an ischemic stroke in the right cerebellar hemisphere. (B) Computed tomographic perfusion showed bilateral cerebellar hemisphere hypoperfusion, especially on the right side. (C) Computed tomographic angiography revealed an occlusion of both vertebral arteries at their origins without obvious stumps. (A)-(B) Early and late phase right subclavian injection, with right vertebral artery occlusion at its origin, reconstituted at C5 by the deep cervical artery (white arrow). (C)-(D) Synchro-2 microwire and SL-10 microcatheter passed through the deep cervical artery to right vertebral artery (white arrow). (E) Microcatheter injection showing in the true lumen of right vertebral artery (white arrow); (F)-(G) Synchro-2 microwire and SL-10 microcatheter reached the left vertebral ostium and then to the left subclavian artery (white arrow), using Synchro-2 wire as a marker, a PT-2 microwire (0.014 in × 300 cm) found the true lumen of the left VA and a distal embolic protection device (Spider FX; EV3, Irvine, CA, USA) was deployed distally in the V2 segment. (H) Angiography after the stent planted.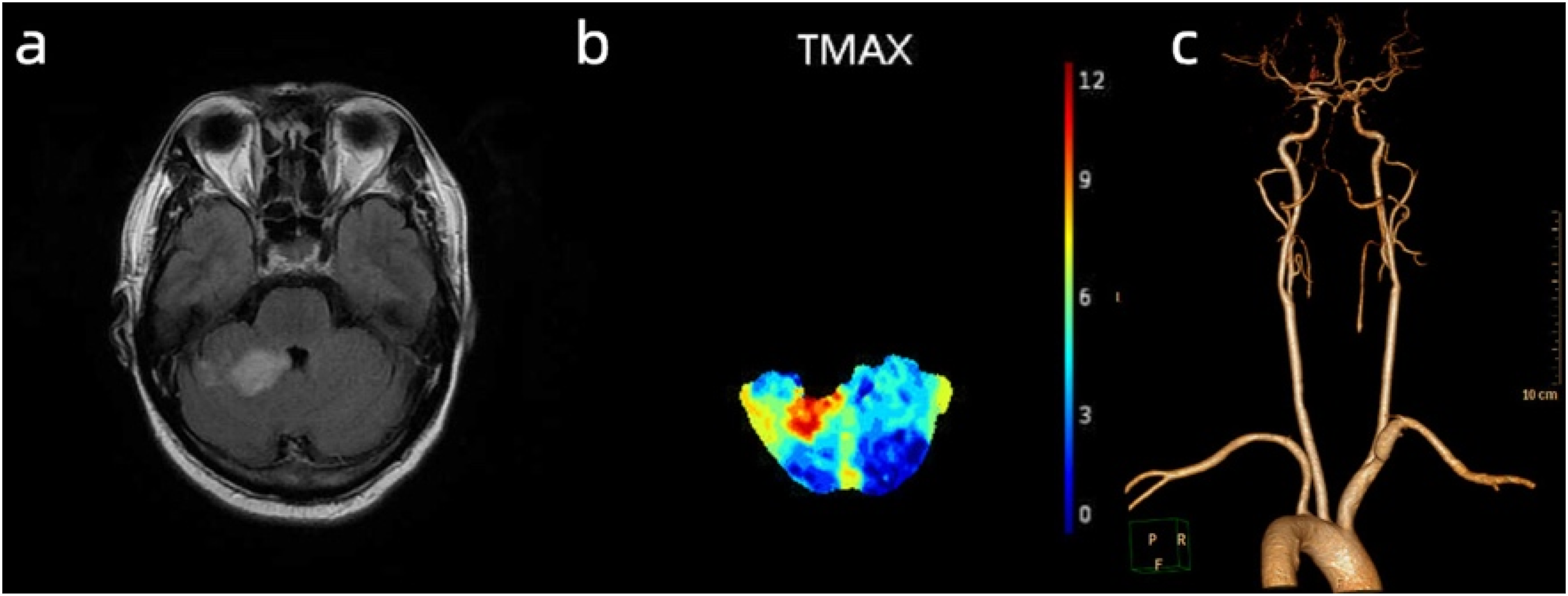
Postintervention and Follow-Up
Postoperative CT scan was performed immediately to exclude intracranial hemorrhage. Patients were placed on dual-antiplatelet therapy for 6 months after discharge, followed by a single antiplatelet drug for lifelong treatment. The 90-day modified Rankin scale (mRS) score 9 was assessed by experienced physicians in the Department of Neurology. A favorable outcome was defined as an mRS score ≤2. All patients did the CTA or DSA at 6-month follow-up.
Results
Summary of Patients With Endovascular Recanalization.
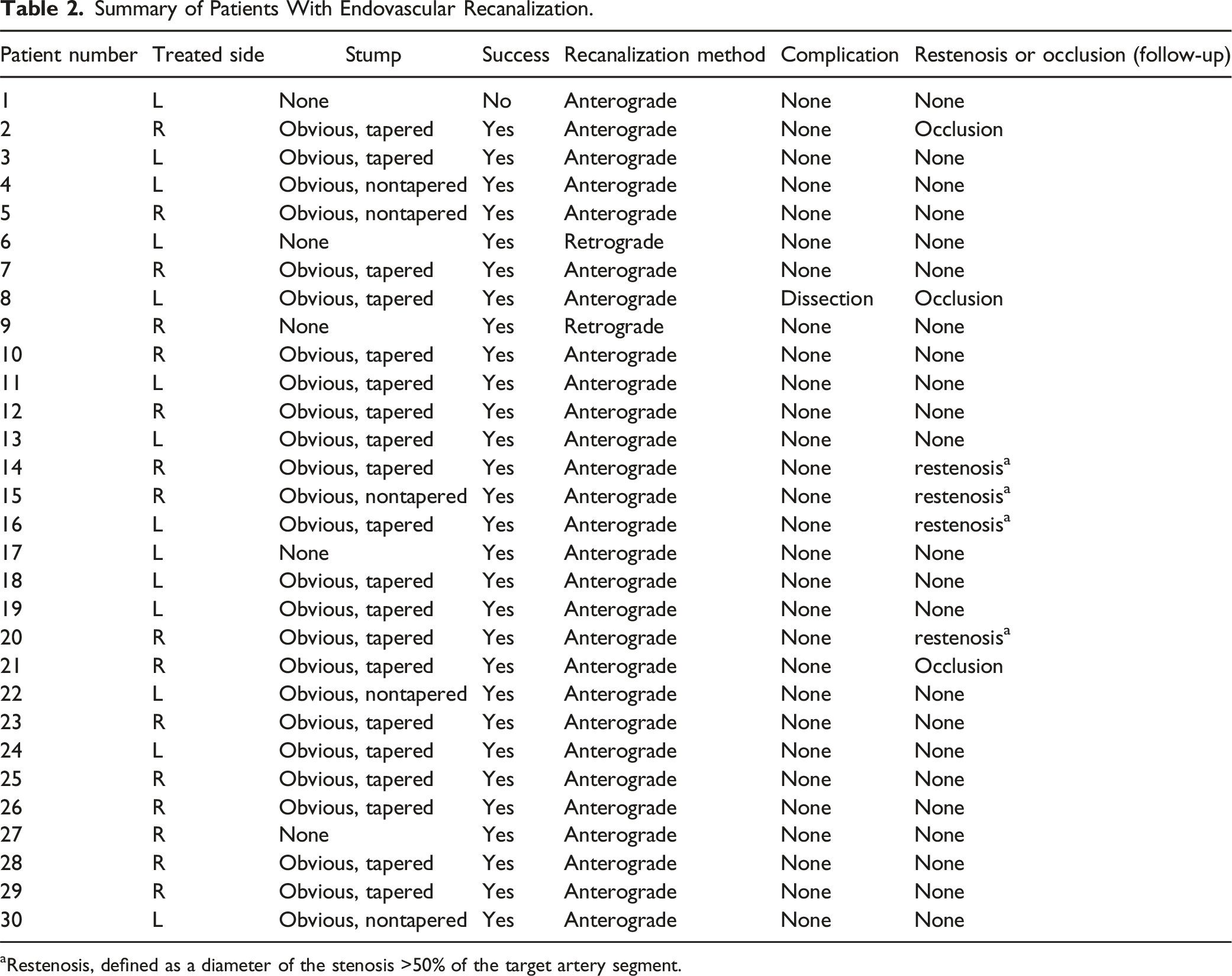
aRestenosis, defined as a diameter of the stenosis >50% of the target artery segment.
Discussion
Posterior circulation ischemic stroke accounts for 25%-30% of all ischemic stroke patients. 10 Kawano et al reported that VASS accounted for 1.4% of acute posterior circulation ischemic stroke cases; recurrent stroke occurred in 25% of patients treated with medical therapy, and 1 quarter of the patients had a poor prognosis (mRS score >2 at discharge). 4 The above studies suggest that this syndrome presents a high recurrence rate and high disability rate. The pathogenesis of VASS can be explainable as follows. The limited distal blood flow can cause propagated thrombus due to the occlusion of vertebral artery. The low-flow state and persistence of antegrade flow distal to the occlusion via the collateral circulation may cause embolization to distal regions from the stagnating clot fragment.1,3,11,12 The optimal treatment for VASS remains unknown. Despite medical therapy, patients with symptomatic extracranial vertebral artery stenosis or occlusion had an 11% annual rate of recurrent ischemic stroke or TIA. 13 For VASS patients, endovascular recanalization may be an alternative.
Endovascular interventional therapy is less invasive and is used increasingly for the treatment of subacute or chronic occlusion of extracranial vertebral artery disease, as a valuable alternative for patients with recurrent stroke or TIA despite optimal medical therapy. Chen et al. reported the overall recanalization rate was 91.3% (21/23) with an incidence of perioperative complications of 4.3% using endovascular revascularization in treating patients with VASS. 14 Gao et al. conducted a multicenter study of endovascular recanalization for patients with medically refractory VASS, the results showed that technical success rate was 86% (43/50) with an incidence of periprocedural complications of 12%. 15 In this study, we obtained a technical success rate of 96.7% (29/30) using endovascular revascularization in patients with posterior circulation ischemia caused by VASS, although 1 patient had asymptomatic dissection of the treated vertebral artery. Taking above into account, it seems that endovascular revascularization has a high successful recanalization rate and low rate of complications.
During a mean follow-up of 6 months, three patients (10.3%) exhibited re-occlusion of the treated vertebral artery, as confirmed by CTA, and 4 patient (13.8%) had in-stent restenosis on DSA. However, there were no cerebral ischemic events during follow-up in any patient. Therefore, endovascular recanalization is a promising therapeutic strategy for select patients treated by experienced interventional physicians. It is essential to perform a comprehensive perioperative evaluation to identify proper patients and lesion characteristics that favor high success rates. Gao et al. proposed classifying symptomatic non-acute extracranial vertebral artery occlusion into 4 types based on the occlusion stump morphology (tapered or non-tapered) and occlusion length (≤50 or >50 mm). 15 In the 4 groups, the recanalization rate declined gradually from type A to D (100%, 94.7%, 80%, and 63.6%, respectively). Similarly, the respective rates of periprocedural complications in types A to D were 0%, 15.8%, 0%, and 27.3%. 15 According to previous literature combined with our single center experience, a tapered stump of ipsilateral VA, short and straight occlusive lesion, mild or absent calcification, and visible of distal V2 segment with collateral filling via the branches are considered to be predictors of successful recanalization for VASS patients. 14 During the procedure, posterior circulation embolization is most concerning because it may lead to severe disability or death. Considering the high risk of thromboembolism, embolic protection devices were used in our cases (29/30), except for 1 patient failed with recanalization. We used distal protection devices (Spider FX) to effectively prevent embolisms. None of the patients experienced ischemic stroke of posterior circulation during the operation.
We usually use the antegrade revascularization method. However, if the stump cannot be visualized, and the microwire fails to enter the true lumen after many attempts, we may switch to retrograde recanalization, which we performed successfully in 2 VASS cases after failed antegrade recanalization. However, to perform the procedure, the large collateral branches (usually the thyrocervical trunk and deep cervical artery) should not be too tortuous to enable smooth passage of the micro-guidewire and microcatheter. Note that retrograde recanalization has risks. As the cervical collaterals are relatively small, vasospasm or occlusion of these branches may occur due to manipulation of the micro-guidewire and microcatheter, which may have disastrous consequences, especially in patients with contralateral vertebral artery occlusion or hypoplasia.
Limitations
Limitations of this study should be noted. First, our study was a single-center retrospective study and the sample size was small. Second, MRI was not routinely performed after the procedure, some silent cerebral infarction including embolic infarction could have been missed. Furthermore, the follow-up period was short, and the long-term prognosis of these patients is unknown. Further research is needed in this area.
Conclusions
Endovascular revascularization of patients with VASS is technically feasible in selected patients and has a high procedural success rate with low incidence of complications. A future, large, multicenter, randomized study should confirm these findings.
Footnotes
Acknowledgements
None
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Renjie Ji, Hanfeng Chen and Ziqi Xu. The first draft of the manuscript was written by Renjie Ji and revised by Benyan Luo, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.