
Abstract
Objectives
Chronic limb-threatening ischemia (CLTI) is mostly caused by arteriosclerosis, but is sometimes due to connective tissue disease. However, there is a limited knowledge of clinical outcomes of patients with CLTI with connective tissue disease. The objective of the study was to assess outcomes after distal bypass in these patients using global vascular guidelines.
Material and Methods
Data from distal bypasses performed for CLTI at a single center from 2014 to 2023 were evaluated retrospectively. Clinical outcomes after distal bypass were compared for patients with CLTI with arteriosclerosis (AS group) and those with connective tissue disease (CD group). The primary endpoints were limb salvage and wound healing.
Results
Of the 282 distal bypasses performed for 222 patients with CLTI, 22 were conducted for 21 patients with connective tissue disease (CD group). The connective tissue disease was progressive systemic scleroderma (n = 11 patients), pemphigoid diseases (n = 2), polyarteritis nodosa (n = 2), rheumatoid arthritis (n = 2), and others (n = 4). Compared with the AS group, the CD group included more females (P = .007) and had greater oral steroid use (P < .001) and a higher Global Limb Anatomical Staging System (GLASS) inframalleolar (IM) modifier P2 (P < .001). The mean follow-up period of the whole cohort was 27 ± 22 months with no significant difference between the groups (P = .25), and 22 limbs required major amputation during this period. The 2-year limb salvage rate was significantly lower in the CD group compared to the AS group (75% vs 94%, P = .020). Wound healing was achieved in 220 (78%) limbs, and the 12-month wound healing rate was significantly lower in the CD group (52% vs 86%, P = .006).
Conclusion
The low 2-year limb salvage and 12-month wound healing rates in patients with CLTI with connective tissue disease indicate that distal bypass may be challenging in these patients.
Keywords
Introduction
Endovascular treatment (EVT) is recommended for aortoiliac and femoropopliteal lesions as first-line treatment due to its lower invasiveness, favorable early outcomes, and technical advances.1,2 However, treatment decision-making (open bypass or EVT) for infrapopliteal lesions remains controversial.3,4 Global vascular guidelines (GVGs) recommend surgical revascularization for average-risk patients with greater limb severity and anatomical complexity, and EVT for high-risk patients or those with less limb severity and anatomical complexity. 5 A recent randomized control trial (RCT) showed the superiority of surgical revascularization in patients with an appropriate autologous vein, compared with EVT. 4 However, guidelines and RCTs mainly focus on cases of chronic limb-threating ischemia (CLTI) due to arteriosclerosis. Most CLTI is caused by arteriosclerosis, but some cases may be due to thromboangiitis obliterans (TAO) and connective tissue disease. Connective tissue disease represents a variety of pathologies, including rheumatoid arthritis and systemic sclerosis, that commonly involve tissue inflammation, are frequently due to an autoimmune antibody, and often aggravate atherosclerosis.6–8 However, there is limited knowledge of clinical outcomes, and especially wound healing, after revascularization in patients with CLTI due to connective tissue disease.9–12 Therefore, this study was performed to assess clinical outcomes after distal (tibial and pedal) bypass in such patients based on the GVGs.
Methods
A total of 282 distal bypasses (222 patients) performed for CLTI at a single center from May 2014 to May 2023 were evaluated retrospectively. The subjects were adult patients (≥18 years) with tissue loss (Rutherford class 5 or 6). Cases with ischemic rest pain and TAO were excluded from the study. Cases of redo bypass and bypass with an artificial graft were also excluded. Clinical outcomes after distal bypass were compared between patients with CLTI with arteriosclerosis (AS group, 260 limbs, 201 patients) and those with connective tissue disease (CD group, 22 limbs, 21 patients). The patients in the CD group were diagnosed using American College of Rheumatology criteria. 13 These patients had connective tissue diseases with an autoimmune and likely acquired inflammatory component, including rheumatoid arthritis, systemic sclerosis, pemphigoid diseases, polyarteritis nodosa, mixed connective tissue disease, and vasculitis syndrome. Patients with genetically based conditions such as Ehlers-Danlos syndrome, Marfan syndrome and osteogenesis imperfecta were excluded from the study. Baseline characteristics, procedural details, hospital outcomes, and medium-term outcomes were retrieved from medical records in March 2024. The primary endpoints of the study were limb salvage and wound healing after distal bypass. The secondary endpoints were freedom from major adverse limb events (MALE) and survival.
Definitions
Distal bypass was defined as tibial bypass (distal anastomosis to the anterior tibial artery, posterior tibial artery, and peroneal artery) and pedal bypass (distal anastomosis to the dorsalis pedis artery, plantar artery, and their branches). Distal bypass did not include distal anastomosis to the tibioperoneal trunk. Limb salvage was defined as freedom from major amputation (above-ankle amputation). Based on the GVGs, limb severity and anatomical complexity were evaluated by wound, ischemia, and foot infection (WIfI) stage and Global Limb Anatomical Staging System (GLASS) stage.5,14 Below the ankle runoff was assessed using the GLASS inframalleolar (IM) modifier, again with reference to the GVGs. 5 Major adverse cardiovascular events (MACE) was defined as cardiovascular death, non-fatal myocardial infarction, unstable angina, congestive heart failure, stroke, or another cardiovascular event requiring hospitalization. MALE was defined as major amputation (above-ankle amputation), redo bypass, revision surgery, thrombectomy, or thrombolysis. 15
Procedure and Follow-Up Methods
Procedural details have been described elsewhere.16,17 Preoperative duplex ultrasound (DUS) was used to assess the great saphenous vein (GSV), small saphenous vein, and arm veins to confirm a diameter >2.5 mm and suitability for distal bypass. Most bypasses were performed with a single-segment GSV in a non-reversed fashion. Single artery outflow was chosen for all limbs without composite Y grafts. Completion angiography was performed routinely. The graft flow rate was evaluated using a transit time flowmeter just before wound closure. 18 All patients were enrolled in a follow-up program, as described elsewhere. 19 Briefly, this program included DUS graft surveillance, ankle brachial index measurement, and a wound clinic at 1, 2, 3, 4, and 6 months post-procedure and every 3 months thereafter. For cases with significant stenosis on DUS, EVT was performed for graft salvage as first-line treatment. Redo distal bypass or thrombectomy was conducted for symptomatic patients with graft occlusion.
Medication
Patients who were already taking antiplatelet agents continued to take these drugs. For patients who did not take these drugs, aspirin (100 mg daily) and/or clopidogrel (75 mg daily) was started at least 1 week before the procedure. The decision to conduct single antiplatelet therapy (SAPT) or dual antiplatelet therapy (DAPT) was made by the vascular surgeon. Patients with dyslipidemia were treated with a statin. Standard treatment was provided for connective tissue disease. Oral steroids for patients with connective tissue disease were used at the discretion of the specialist.
Ethics
The study was performed under the principles of the Declaration of Helsinki. The protocol was approved by the JA Hiroshima General Hospital Ethics Committee (approval number: 23-98). The institutional review board (IRB) waived the need for informed consent from patients because of the observational, non-interventional, and non-invasive design. The opt out method was alternatively used.
Statistical Analysis
Continuous values are expressed as the median (interquartile range) or mean ± standard deviation, and categorical values as frequency and percentage. Differences in baseline characteristics, procedural details, and hospital outcomes between groups were compared by Mann-Whitney U test for continuous variables, and by Fisher exact test for categorical variables. Medium-term outcomes (primary patency, secondary patency, limb salvage, freedom from MALE, wound healing, survival) were assessed by the Kaplan-Meier method with a log-rank test. Univariate analysis of risk factors for limb salvage and wound healing was also performed using the Kaplan-Meier method with a log-rank test. Variables used for univariate analysis were connective tissue disease, advanced age (≥80 years), female gender, hypertension, diabetes, coronary artery disease, cerebrovascular disease, hemodialysis, ambulatory, smoking history (ever smoked), SAPT, DAPT, oral anticoagulant, statin, steroid, GLASS stage III, GLASS IM modifier P2, WIfI stage 4, proximal anastomosis to popliteal artery, pedal bypass, GSV use, spliced vein graft, non-reversed fashion, prolonged operation (≥180 min), and low graft flow (≤15 mL/min). Variables with P < .05 in univariate analysis were considered to be potential risk factors for limb salvage and wound healing and were selected for multivariate Cox proportional hazard analysis. P < .05 was defined as significant. Statistical analyses were performed with EZR (Saitama Medical Centre, Jichi Medical University, Saitama, Japan), which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). 20
Results
Of the 282 distal bypasses performed for 222 patients with CLTI at our center from May 2014 to May 2023, 22 bypasses were conducted for 21 patients with connective tissue disease (CD group). The underlying connective tissue disease was progressive systemic scleroderma (n = 11 patients), pemphigoid diseases (n = 2), polyarteritis nodosa (n = 2), rheumatoid arthritis (n = 2), mixed connective tissue disease (n = 2), granulomatosis with polyangiitis (n = 1), and Goodpasture syndrome (n = 1).
Baseline Characteristics of Patients With CLTI With or Without Connective Tissue Disease.
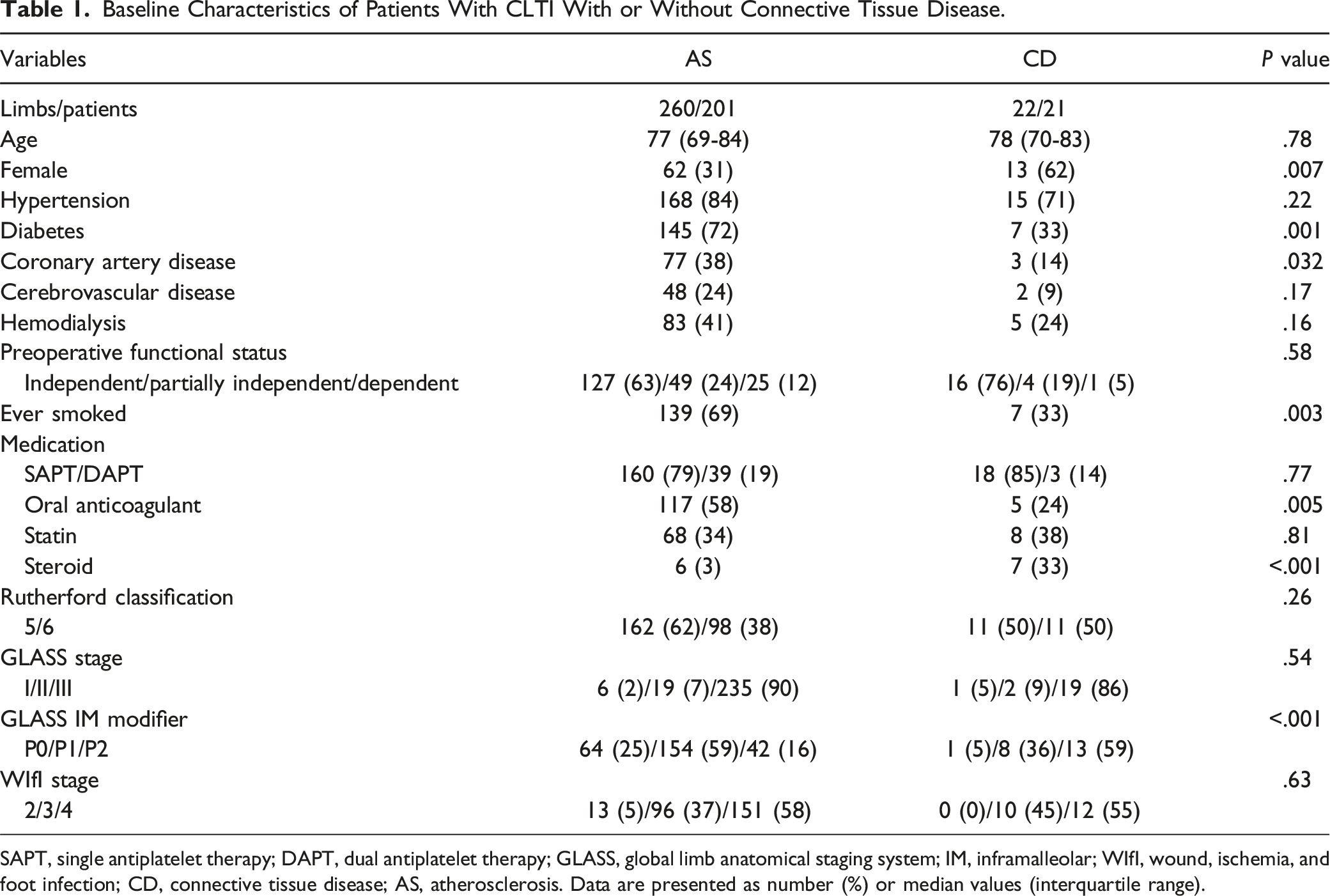
SAPT, single antiplatelet therapy; DAPT, dual antiplatelet therapy; GLASS, global limb anatomical staging system; IM, inframalleolar; WIfI, wound, ischemia, and foot infection; CD, connective tissue disease; AS, atherosclerosis. Data are presented as number (%) or median values (interquartile range).
Procedural Details and Hospital Outcomes in Patients With CLTI With or Without Connective Tissue Disease.
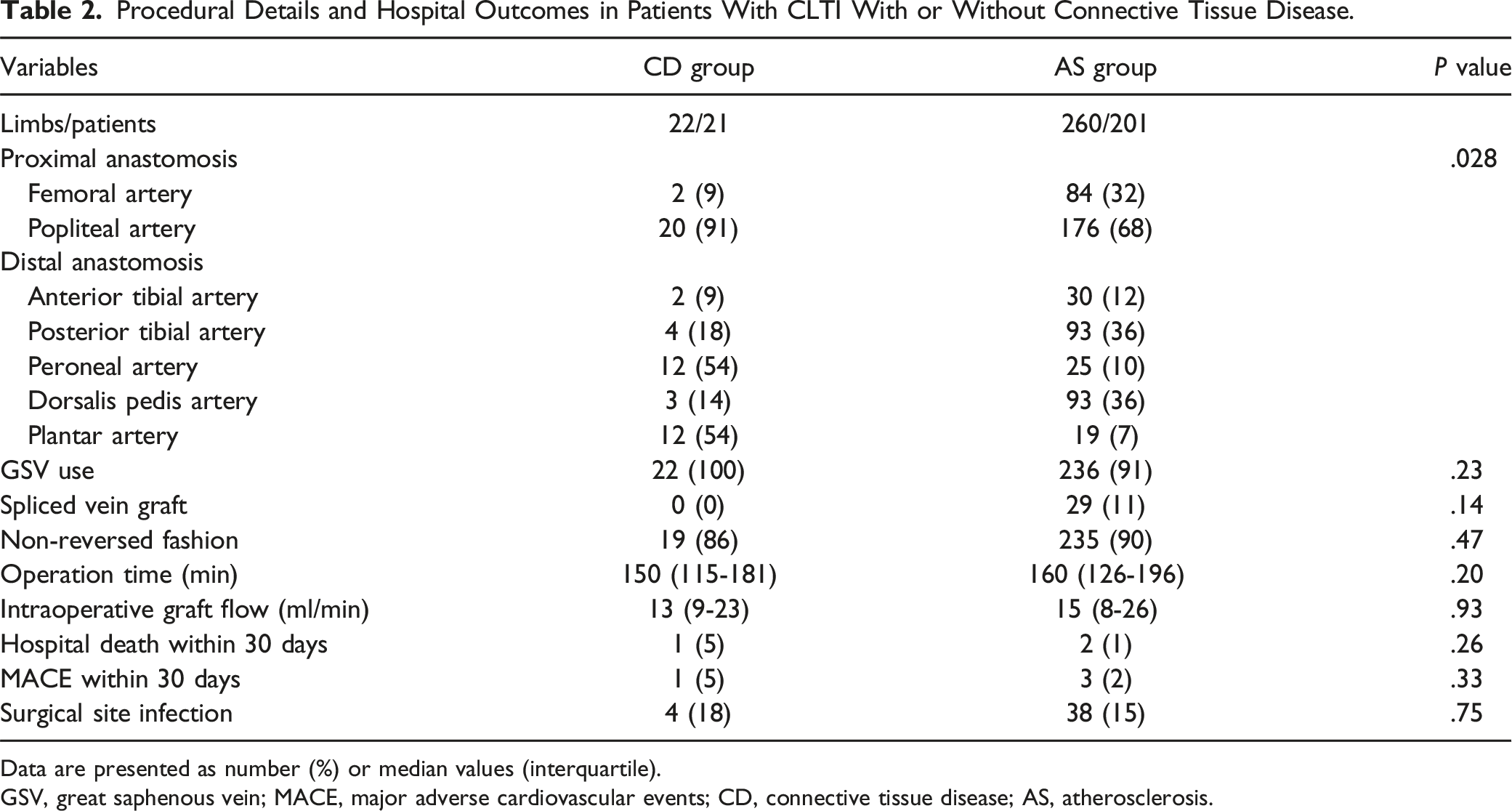
Data are presented as number (%) or median values (interquartile).
GSV, great saphenous vein; MACE, major adverse cardiovascular events; CD, connective tissue disease; AS, atherosclerosis.
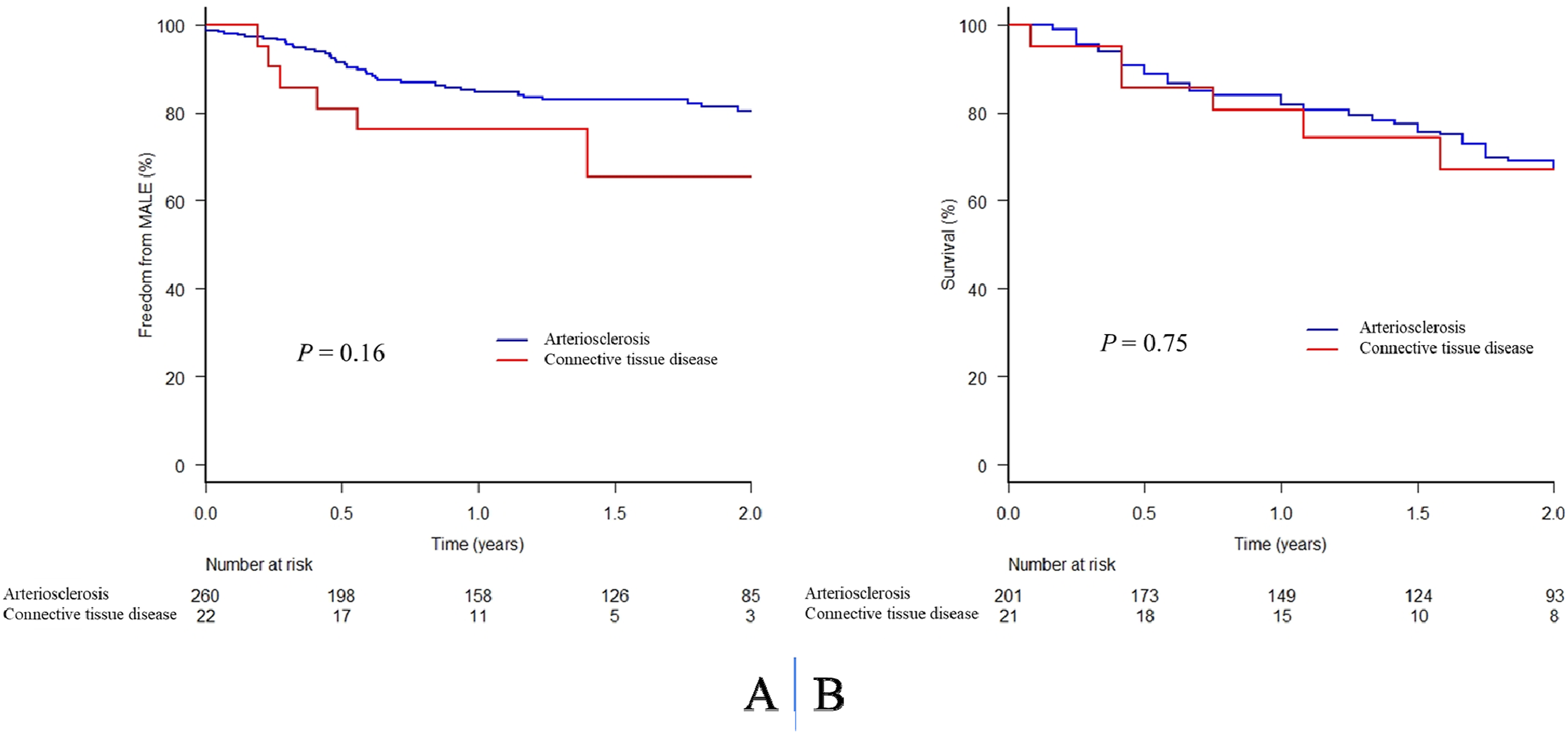
The mean follow-up period of the whole cohort was 27 ± 22 months, with no significant difference between the CD and AS groups (P = .25). During follow-up, 22 limbs required major amputation. The limb salvage rate was significantly lower in the CD group than the AS group (91% vs 96% at 1 year, 75% vs 94% at 2 years, P = .020, Figure 1A). Wound healing was achieved in 220 limbs (78%), and the wound healing rate was significantly lower in the CD group (33% vs 59% at 3 months, 52% vs 73% at 6 months, 52% vs 86% at 12 months, P = .006, Figure 1B). In the whole cohort, the 1- and 2-year rates of freedom from MALE were 84% and 79%, and the 1- and 2-year survival rates were 82% and 68%, with no significant differences between the groups (Figure 2A and B). The 1- and 2-year primary patencies were 54% and 46%, and the 1- and 2-year secondary patencies were 76% and 72%, again with no significant differences between the groups (P = .56, P = .53). Limb salvage rate (A) and wound healing rate (B) in patients with CLTI with or without connective tissue disease. Major adverse limb events (A) and survival (B) in patients with CLTI with or without connective tissue disease.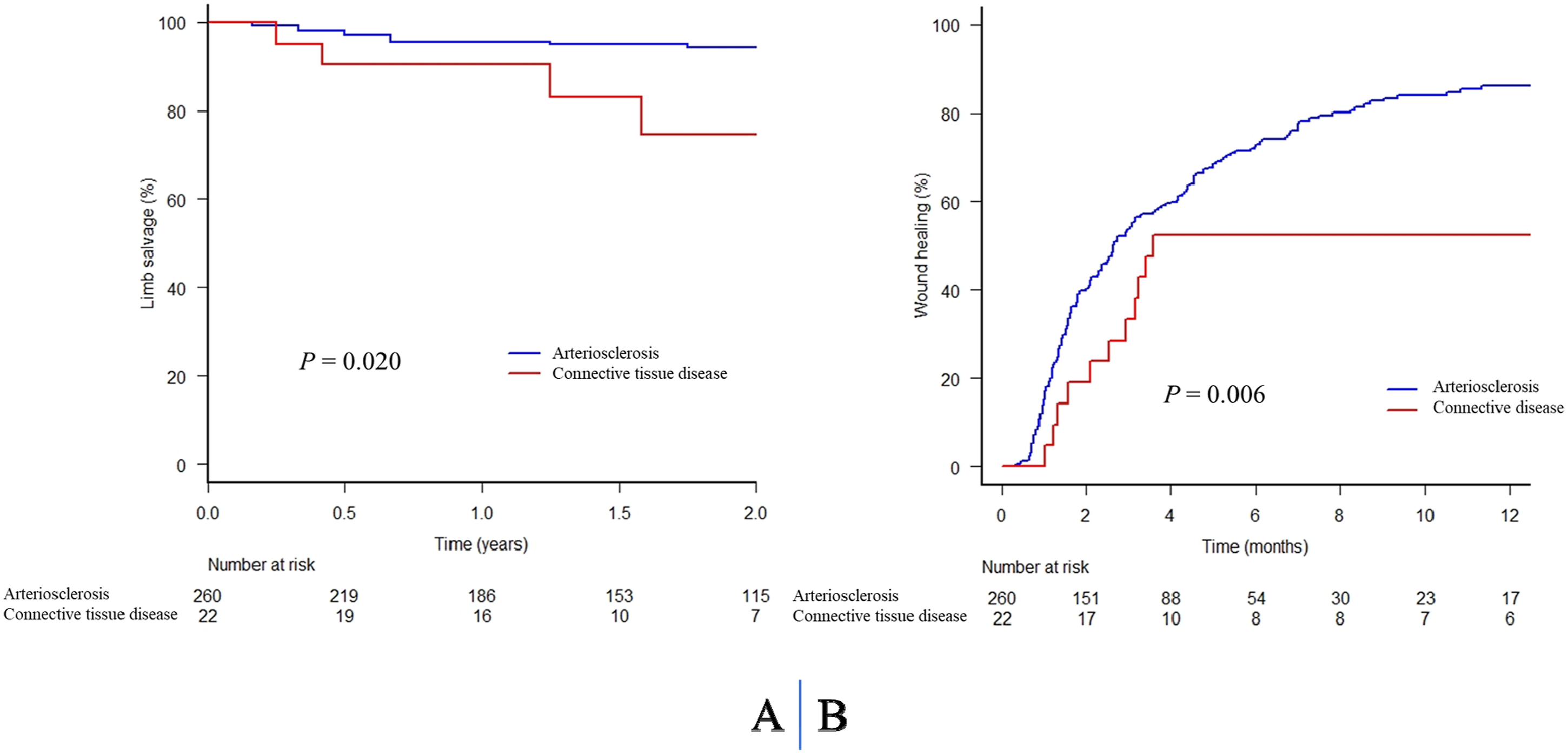
Univariate and Multivariate Analysis of Risk Factors for Limb Salvage and Wound Healing After Distal Bypass in Patients With CLTI.

SAPT, single antiplatelet therapy; DAPT, dual antiplatelet therapy; GLASS, global limb anatomical staging system; IM, inframalleolar; WIfI, wound, ischemia, and foot infection; PA, popliteal artery; GSV, great saphenous vein; HR, hazard ratio; CI, confidence interval.
Data are presented as number (%) or median values (interquartile range).
Prolonged operation time was defined as ≥ 180 min, and low graft flow was defined as ≤ 15 ml/min.
Discussion
There were two main findings in the study. First, the 2-year limb salvage rate after distal bypass of 75% in the CD group was significantly lower than that in the AS group. Second, the CD group had significantly more severe below-the-ankle runoff and a 12-month wound healing rate of 52% that was significantly lower than that in the AS group.
Limb salvage has been reported to be favorable in patients with CLTI undergoing surgical revascularization.21,22 In a series of 401 malleolar bypasses for CLTI, Kikuchi et al found 2-year limb salvage rates in non-hemodialysis and hemodialysis cases of 99% and 90%, respectively, 21 while in a series of more than 1000 dorsalis pedis bypass cases, Pomposelli et al 22 reported a 2-year limb salvage rate of over 80%. However, the limb salvage rate after surgical revascularization may be lower in patients with CLTI with connective tissue disease.9,11 Thus, Deguchi et al reported that 4 of 8 scleroderma cases with CLTI had limb loss after surgical revascularization, 10 and Yamamoto et al 9 found a significantly lower 2-year limb survival rate after bypass surgery for patients with CLTI with vasculitis or connective tissue-related disease (n = 31, 75%) compared to those with atherosclerosis (n = 162, 94%).
In the current study, the 2-year limb salvage rates were 75% and 94% in the CD and AS groups, respectively, which are similar to those in previous reports. However, the rate was significantly lower in the CD group, despite the patients with connective tissue disease having fewer comorbidities (diabetes, 33%; coronary artery disease, 14%; ever smoked, 33%) compared to those with atherosclerosis. The CD group had significantly poorer below-the-ankle runoff (P < .001), which might have affected the lower limb salvage rate in this group. This suggests that distal bypass for patients with connective tissue disease may be challenging from the perspective of limb salvage. Furthermore, Obara et al 12 found favorable outcomes for 1-year amputation-free survival (89%) and freedom from reintervention (81%) after EVT in patients with CLTI with connective tissue disease. Thus, further investigation of decision-making for treatment of patients with CLTI with connective tissue disease is needed in a future study.
Wound healing in patients with CLTI with connective tissue disease after surgical revascularization has not been widely investigated. In this study, the wound healing rates in the CD and AS groups were 33% and 59% at 3 months, 52% and 73% at 6 months, and 52% and 86% at 12 months, respectively, and were significantly lower in the CD group. The difference in wound healing rate between the groups may be due to below-the-ankle runoff. The GLASS IM modifiers in the CD and AS groups were P0 in 1 (5%) and 64 (25%), P1 in 8 (36%) and 154 (59%), and P2 in 13 (59%) and 42 (16%) cases, and the CD group had significantly poorer below-the-ankle runoff. In our previous series of 254 distal bypasses for patients with CLTI, the wound healing rates in P0, P1, and P2 cases were 86%, 79%, and 68% at 6 months, and 97%, 93%, and 79% at 12 months, respectively, and were significantly lower in P2 cases (P2 vs P0, P = .008; P2 vs P1, P = .027). 16 One other possible explanation may be higher use of oral steroids in the CD group, since long-term steroid use has a negative effect on wound healing due to inhibition of cell proliferation and resulting bacterial and fungal infections. 23 Thus, a further study is needed for patients with CLTI with connective tissue disease who are taking long-term steroids.
Limitations
This study has several limitations, including the relatively small cohort and retrospective observational design. We were unable to evaluate the effects of steroids on limb salvage and wound healing due to the small number of steroid users. Also, the median age in the CD group was higher than that in previous reports, which might have affected the clinical outcomes. Although the CD group had more females and lower rates of diabetes, coronary artery disease, and a history of smoking, survival rates did not differ between the groups. The similar survival might be reflective of the autoimmune burden compared to atherosclerosis effects. Also, we assessed acquired connective tissue disease only, which might have affected the outcomes. Finally, the study was performed only in Japanese patients, and the results require assessment in other ethnic groups.
Conclusion
The 2-year limb salvage rate and 12-month wound healing rate in the CD group were 75% and 52%, respectively, and both were significantly lower than those in the AS group. These results suggest that distal bypass for patients with CLTI with connective tissue disease is challenging, and further investigation of the appropriate treatment for these patients is needed in a future study.
Footnotes
Acknowledgments
We gratefully acknowledge the work of past and present members of the vascular team (i.e., physical therapists, wound nurses, certified diabetes educators, pharmacists, nutritionists, clinical engineers, ultrasound technicians, medical technologists, radiological technologists, medical secretaries, and prosthetists).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.